


Abstract
Soft-tissue attenuation of γ-photons is the most common source of artifacts and remains an intricate problem for myocardial perfusion imaging (MPI) by SPECT. Breast and subdiaphragmatic artifacts are the most frequent cause of false-positive findings in women. Many methods of overcoming attenuation artifacts have been introduced, including prone positioning to avoid breast attenuation or use of hybrid SPECT/CT systems. The purpose of this study was to evaluate the role of prone images in attenuation correction (AC) when CT AC is compared with MPI. Methods: Forty-four patients were initially included in the study. Statistical analysis was done for 30 patients with suspected or confirmed ischemic heart disease. All patients underwent ordinary supine stress/rest SPECT MPI followed by additional stress/rest prone SPECT and stress/rest SPECT/CT. Each study was interpreted separately, and their results were compared. Results: It was found that 58% (31/53) of the depicted defects were attributable to attenuation artifacts; the CT AC imaging technique was able to correct 52%, versus 49% for prone imaging. Sensitivity, specificity, and diagnostic accuracy were 100%, 90.3%, and 94%, respectively, for CT AC, versus 100%, 83.8%, and 91%, respectively, for prone imaging. Inferior wall defects were more common in men (95%), in whom CT AC performed better than prone imaging (i.e., 92.9% in CT AC vs. 90.9% in prone imaging). On the other hand, anterior wall defects were more common in women (83.3%), in whom prone imaging was better than CT AC. Conclusion: Both CT AC and prone imaging increased the specificity and diagnostic accuracy of MPI without affecting the sensitivity.
SPECT myocardial perfusion imaging (MPI) is considered a useful noninvasive imaging modality in the evaluation of suspected or established coronary artery disease (CAD). Moreover, it has an important role in risk assessment, management decisions, and prognosis for patients with ischemic heart disease. Radionuclide myocardial perfusion scintigraphy has become established as one of the main functional cardiac imaging techniques for ischemic heart disease, constituting approximately one third of all nuclear medicine procedures done annually in the United States, with substantial growth annually. The increasing use of myocardial perfusion scintigraphy for the diagnosis of clinically important CAD is the direct result of its strengths; myocardial perfusion scintigraphy is a robust and highly validated technique, is widely available, and has a clear role in the assessment of patients investigated for CAD, as stated by internationally published guidelines (1). However, imaging artifacts can limit the utility of the study. These artifacts can be technical or patient-related. Many additive techniques have been used to overcome this drawback.
Patient motion and soft-tissue attenuation are the two most common sources of artifacts in MPI. Researchers are focusing on attenuation artifacts and how to overcome them to improve diagnostic accuracy by reading physicians and certainty about the final report. Patient-related artifacts remain an issue of concern. The location of an attenuation artifact depends on the position of the soft-tissue attenuator in relation to the left ventricle. The severity of the artifact depends on the size and density of the attenuator in relation to adjacent tissue. Within the acquired SPECT image, the artifact may appear as a fixed or reversible defect, depending on whether the attenuator is in a constant or variable position in stress and rest image acquisitions (2). Several methods have been added to conventional SPECT imaging for attenuation correction (AC). Acquiring additional prone SPECT images, as well as upright (erect) images, has been described for subdiaphragmatic attenuation to differentiate attenuation artifacts from true hypoperfusion defects, thus improving the quality and increasing the specificity and accuracy of MPI.
Now, in the era of hybrid imaging, SPECT/CT devices are used to produce an integrated CT AC image to discriminate between true perfusion defects and artifacts. The instrumentation, radiopharmaceuticals, and methodology used for myocardial perfusion scintigraphy have evolved over the years. Multiview planar imaging was followed by SPECT and then gated SPECT, SPECT/CT, and PET/CT. However, the underlying physiologic principles that make MPI an important diagnostic tool remain unchanged (3).
Although SPECT imaging of myocardial perfusion provides a sensitive means of detecting and localizing CAD and assessing left ventricular function, the method suffers from the potential for poor specificity due to image artifacts related to both patient and technical factors (2). Technical artifacts include patient motion, gating problems, and reconstruction and processing errors. On the other hand, soft-tissue attenuation, breast attenuation, diaphragmatic attenuation, subdiaphragmatic activity, and lateral chest-wall fat attenuation are among the patient-related artifacts.
AC Methods
Attenuation within the body is not uniform; therefore, accurate AC requires a precise estimate of the patient-specific attenuation distribution (3). For this reason, many attempts have been made to overcome attenuation artifacts. Attenuation maps have been generated sequentially on simultaneous acquisition of emission and transmission images, using the gadolinium source and hybrid SPECT/CT devices (2).
Low-dose CT, the preferred AC method, is performed sequentially after the emission scan but may cause misregistration artifact due to motion during the emission scan and different breathing patterns between the long emission scan and the very short CT AC scan.
Another AC method, which is employed in D-SPECT imaging protocols, is the use of two-position comparison (upright and supine). In one study, MPI using a D-SPECT camera (ultra-high sensitive CZT crystals with solid-state technology) increased confidence about the interpretation, compared with stress-only supine MPI.
Acquiring additional nongated and non-AC SPECT images with the patient prone has been an effective AC method but is not possible in every patient because of physical limitations, despite the shorter acquisition time than for supine imaging. It yields more accurate scintigraphic interpretations without any additional cost, is inexpensive, and does not deliver any extra radiation to the patient. Prone positioning is associated with increased inferior and septal wall counts and less patient motion (2). Patient discomfort should be considered a limiting factor in this additional-acquisition protocol, being less suitable for women with large breasts and obese patients (2). The addition of prone positioning to stress supine myocardial scintigraphy could decrease false-positive rates and lead to more accurate results. Furthermore, it was postulated that prone positioning increases specificity without compromising sensitivity for the diagnosis of CAD. There is also the key benefit of reducing the number of unnecessary rest studies performed while minimizing radiation exposure, investigation time, and costs (5).
Use of a transmission line source (153Gd), with emission and transmission scans obtained simultaneously for better registration between the two, is another possible AC method. However, quality-control testing of the transmission source needs to be done separately, and the fact that the source needs to be replaced every 18 mo represents an additional expense. In addition, occasional mechanical issues with the line source could cause camera downtime.
Evaluating wall motion and wall thickening (with or without myocardial contours) from gated images could also help distinguish attenuation artifacts from true defects on perfusion images.
SPECT/CT AC
The advent of hybrid SPECT/CT technology gave rise to the potential for CT images to serve as transmission maps for the AC of SPECT data. Images produced by CT hold many advantages: they are obtained in seconds or a few minutes (depending on the CT device) and generally provide high-quality transmission maps, there is no radioactivity cross-talk with emission images, and the life of the x-ray tube is very long. The additional radiation dose to the patient varies considerably among scanners and protocols but is generally low, with low-dose CT devices being used in the first generation. Hybrid SPECT/CT systems, in particular, have a low effective dose of about 1 mSv or less (6).
Low-dose CT AC allows review of chest CT image (nondiagnostic quality) for incidental findings (cardiac or noncardiac) and assessment for the presence of calcium (with or without scoring). If 4-row (or more) multidetector CT (MDCT) is used, coronary artery calcium scoring can be added to improve diagnostic certainty, especially in an equivocal MPI study with a score of 0 versus an extensive calcium score. With 64-row MDCT, state of the art coronary CT angiography can be added as well.
Common factors that may degrade CT maps are patient movement during the acquisition and excessive beam hardening created by selective low-energy x-ray attenuation in bone structures or metallic implants. Also, in hybrid systems with a CT field of view smaller than that of SPECT, exclusion of part of the thorax from CT slices, so-called body truncation, inevitably has an impact on the accuracy of AC in patients with a large body habitus. Motion artifacts are common when slow-CT devices are used. Fast multidetector CT scanners acquire images of the chest within a few seconds while the patient is holding the breath, thereby avoiding such artifacts (6). Misregistration of emission–transmission slices can result from a software misalignment error or, more frequently, from patient motion between the SPECT and the CT acquisitions, a change in the breathing pattern between acquisitions, misalignment of the examining table as it moves inside the gantry, and upward creeping of the heart after cessation of vigorous stress (7). SPECT/CT misregistration of some degree is unavoidable with fast CT scanners that take frozen images of the chest, because SPECT acquisition is much slower, includes several respiratory cycles, and represents an average of the chest motion during respiration (8). Actually, misregistration of emission and transmission slices is quite common in MPI SPECT/CT studies (9,10). This misalignment may introduce false defects in MPI images and give rise to interpretation errors if left uncorrected. These are considered case-specific and thus hardly predictable (11). Software tools for manual correction of misregistration have been developed by γ-camera manufacturers.
After use of CT AC, the reconstructed SPECT slices look somewhat different from the non-AC, uncorrected, slices. Apart from elimination of attenuation artifacts, another common feature of corrected images is apical thinning; apical defects frequently create interpretation uncertainties, particularly when these extend to the apical portion of the anterior wall or appear partly or fully reversible at rest. Also, more intense delineation of the right ventricular wall and accentuation of extracardiac subdiaphragmatic activity are common features of CT attenuation, and the myocardial wall of the left ventricle appears thicker and the cavity smaller. These normal patterns should be kept in mind when interpreting AC studies (12). In addition, true perfusion defects, particularly in the inferior and inferolateral walls, usually appear smaller in corrected images than in uncorrected images.
CT AC is a valuable innovation, particularly helpful in men and obese patients. Moreover, inspection of nondiagnostic CT images may reveal unsuspected concurrent pathology and thereby foster further investigation. Nevertheless, CT AC studies should be interpreted with caution, side by side with non-AC images and in the context of clinical data.
MATERIALS AND METHODS
This prospective study was performed in the Nuclear Medicine Unit of the Kasr El-Aini Center of Radiation Oncology and Nuclear Medicine, Cairo University, from January 2017 to June 2017.
The selection process was approved by the ethical committee and included identifying those patients who fulfilled the inclusion criterion (referral for an MPI scan). Patients were excluded if they had undergone a pharmacologic stress study, had a left bundle branch block, or had undergone or were a candidate for coronary artery bypass grafting.
All patients underwent the 2-d protocol (rest and exercise stress) for conventional electrocardiography-gated 99mTc-sestamibi SPECT MPI. Then, additional CT AC images and prone images were added. An intravenous injection of 555–925 MBq (15–25 mCi) of 99mTc-sestamibi, according to body weight, was used for each study. Cardiac medication, including β-blockers, theophylline derivatives, nitrates, and calcium channel blockers, were discontinued for 48 h before the study, and the patients fasted for 4–6 h before the study.
Rest/stress gated images were acquired with a commercially available dual-head γ-camera equipped with an integrated x-ray transmission system (Siemens). Emission data were acquired using parallel-hole low-energy high-resolution collimators, with the patient in the supine and prone positions. The acquisition orbit was the body contour over a 180° arc, via 30 stops and 30 s per stop. The image acquisition matrix was 128 × 128. Images were acquired on the 140-keV photopeak with a 20% symmetric window. Resting SPECT images were acquired with the patient supine 45–60 min after administration of the radiopharmaceutical, followed by acquisition of prone images. Stress SPECT images were acquired first in the supine position and then in the prone position 30–45 min after exercise and after administration of the radiopharmaceutical. The resting and stress SPECT images were gated via 8 frames per cycle, and the R–R time acceptance window was 20%. The stress and supine SPECT images were corrected for attenuation by the use of a low-dose CT-based transmission scan acquired at a slice step of 1 mm and a current of 80 mA. The total SPECT/CT time was approximately 25 min. All raw datasets were corrected by the isotope decay factor and checked for patient motion by reviewing a rotating cine display.
The projection data from the electrocardiography-gated SPECT scan were summed, and perfusion images were reconstructed with 3-dimensional ordered-subsets expectation maximization and built-in processing that preserved the linearity between photon counts in projection data and pixel values in reconstructed images. The cardiac suite SPECT software of Cedars-Sinai Medical Center (quantitative perfusion SPECT and quantitative gated SPECT) reconstructed cross-sectional cardiac images along the short and long axes of the heart to form short-axis images (from apex to base), horizontal long-axis images (from inferior wall to anterior wall), and vertical long-axis images (from septum to lateral wall).
An experienced physician with more than 15 y of experience in nuclear cardiology interpreted the stress/rest no-AC images, stress/rest CT AC images, and stress/rest prone images separately. The final diagnosis (i.e., whether the elicited hypoperfusion defect was attributable to an attenuation artifact or a true defect) was concluded on the basis of these imaging findings along with the patient’s risk level and other available investigations, including echocardiography and coronary angiography.
Statistical Analysis
Statistical analysis used Microsoft Excel (version 2016) and SPSS software (release 22; IBM Corp.) for Microsoft Windows. Quantitative data were summarized as mean and SD, whereas frequency data were summarized as percentage. Agreement was tested using the κ-statistic. P values of less than 0.05 were considered statistically significant.
RESULTS
The study initially included 44 patients with suspected or confirmed myocardial ischemia. After the MPI images had been interpreted and correlated with clinical risk and other available diagnostic modalities (stress electrocardiography, stress echocardiography, cardiac catheterization), the results for 4 patients were found to be normal (with no perfusion defect) on non-AC, CT AC, and prone imaging, and 10 patients were found to have multivessel disease (a non-AC defect not corrected by either CT AC or prone imaging). These 14 patients did not benefit from the additional images and hence were excluded from the statistical analysis (Table 1). The remaining 30 patients included 20 men (67%) and 10 women (33%), with a mean age of 53 ± 12 y (Table 2).
Presence or Absence of Myocardial Ischemia in the 14 Excluded Patients
Age and Sex Distribution of the 30 Patients
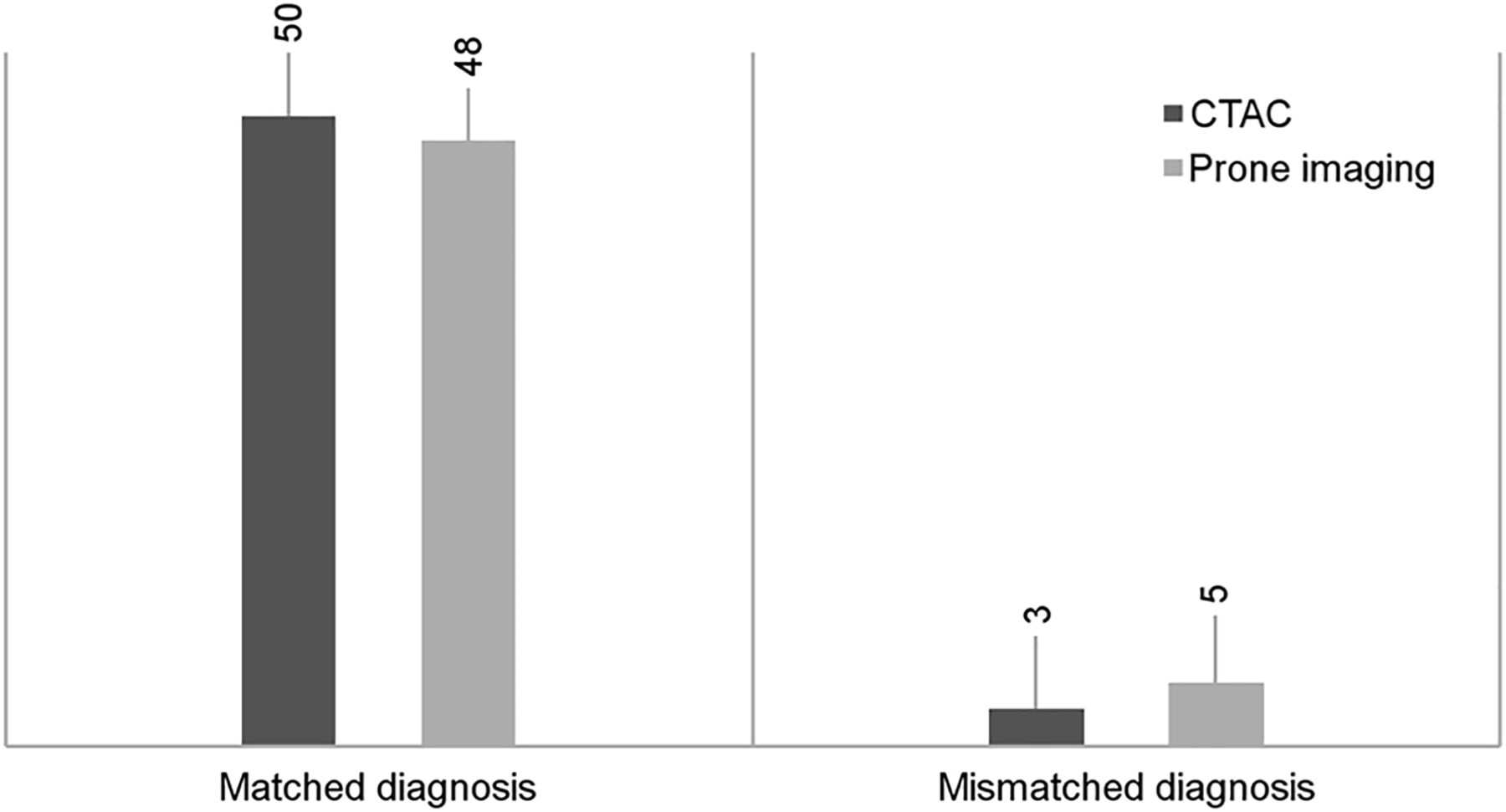
For each patient, the left ventricular myocardial wall as a whole was divided into 5 parts (i.e., apex, anterior wall, inferior wall, lateral wall, and septal wall). The number of hypoperfusion defects elicited in the uncorrected images in the different myocardial walls totaled 53; 39.6% of these were in the inferior wall, and 22.6% were in the anterior wall. After the scan findings had been correlated with the final diagnosis (i.e., attenuation artifact versus true hypoperfusion defect), 31 (58%) defects were finally interpreted as attenuation artifacts and 22 (42%) as true ischemic defects (Table 3). Using the 2 AC techniques, we found that among the 31 non-AC attenuation artifacts, 28 were corrected by CT AC and 26 by prone imaging (Fig. 1).
Agreement Between Correction Technique and Uncorrected Images in All Wall Defects

Corrected and uncorrected artifacts using CT AC and prone imaging.
In CT AC images, 50 of 53 defects (94.3%) were correctly diagnosed: 28 (52.8%) as attenuation artifacts and 22 (41.5%) as true defects. The 3 defects (5.7%) that were not correctly diagnosed were due to a mismatch between the final diagnosis and the CT AC interpretation because CT AC failed to correct the attenuation artifacts. There was a high level of statistical agreement (P < 0.001) between the CT AC findings and the final diagnosis regarding the number of corrected artifacts (Table 4).
Matching Between Correction Technique and Final Diagnosis
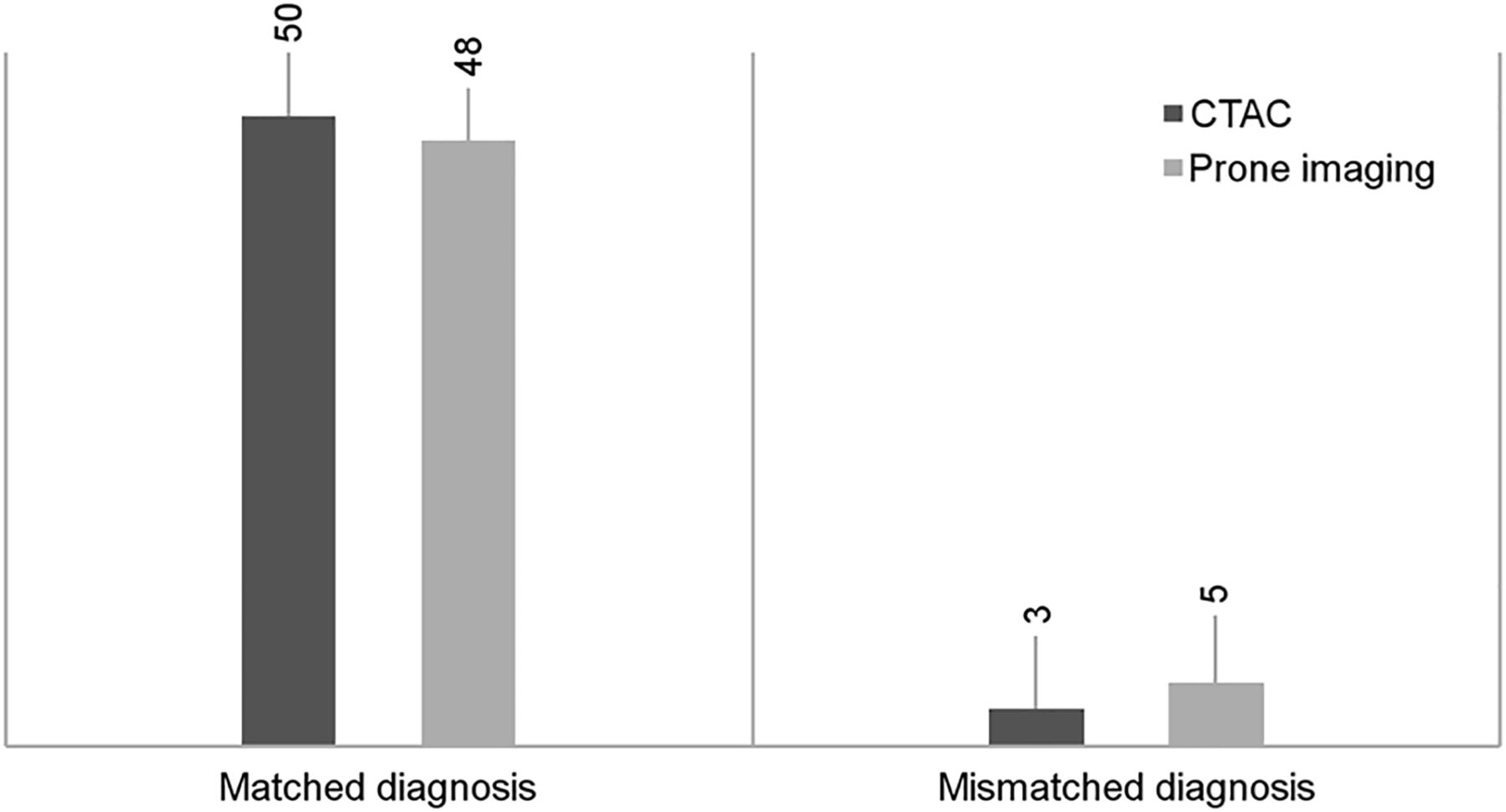
On the other hand, in prone images, 48 of 53 defects (91%) were correctly diagnosed: 26 (49%) as attenuation artifacts and 22 (42%) as true defects. The 5 defects (9%) that were not correctly diagnosed were due to a mismatch between the final diagnosis and the prone interpretation because the prone images failed to correct the attenuation artifacts (Fig. 2). Prone imaging showed statistical agreement with the final diagnosis, with a P value of less than 0.001.
Matching between correction technique and final diagnosis.
Although the sensitivity of the study was almost unaffected by the additional CT AC or prone imaging, the calculated specificity for detection of true defects in the CT AC study was 90.3% and that of the prone images was 83.8% (Tables 5 and 6).
Correlation Between Wall Defects and Final Diagnosis
Specificity and Sensitivity
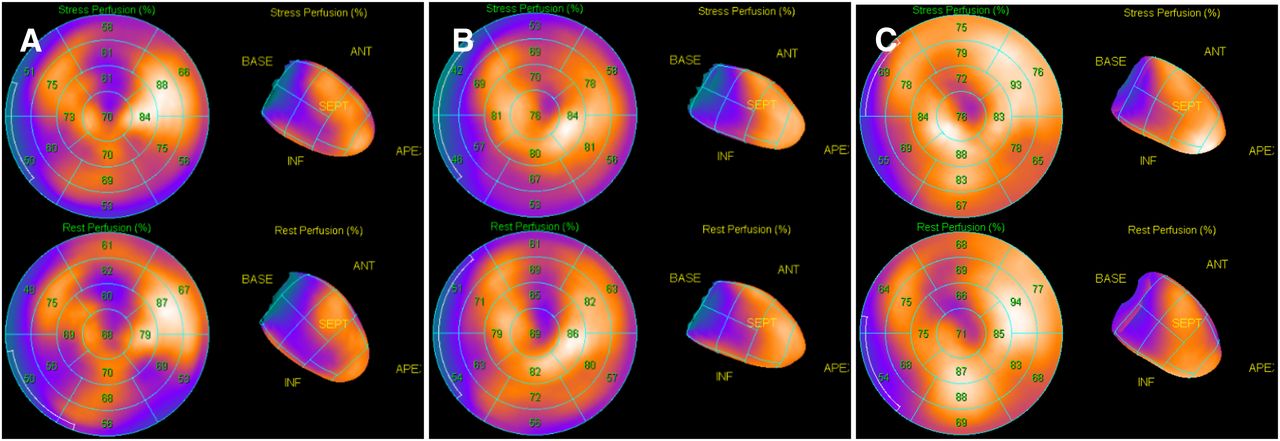
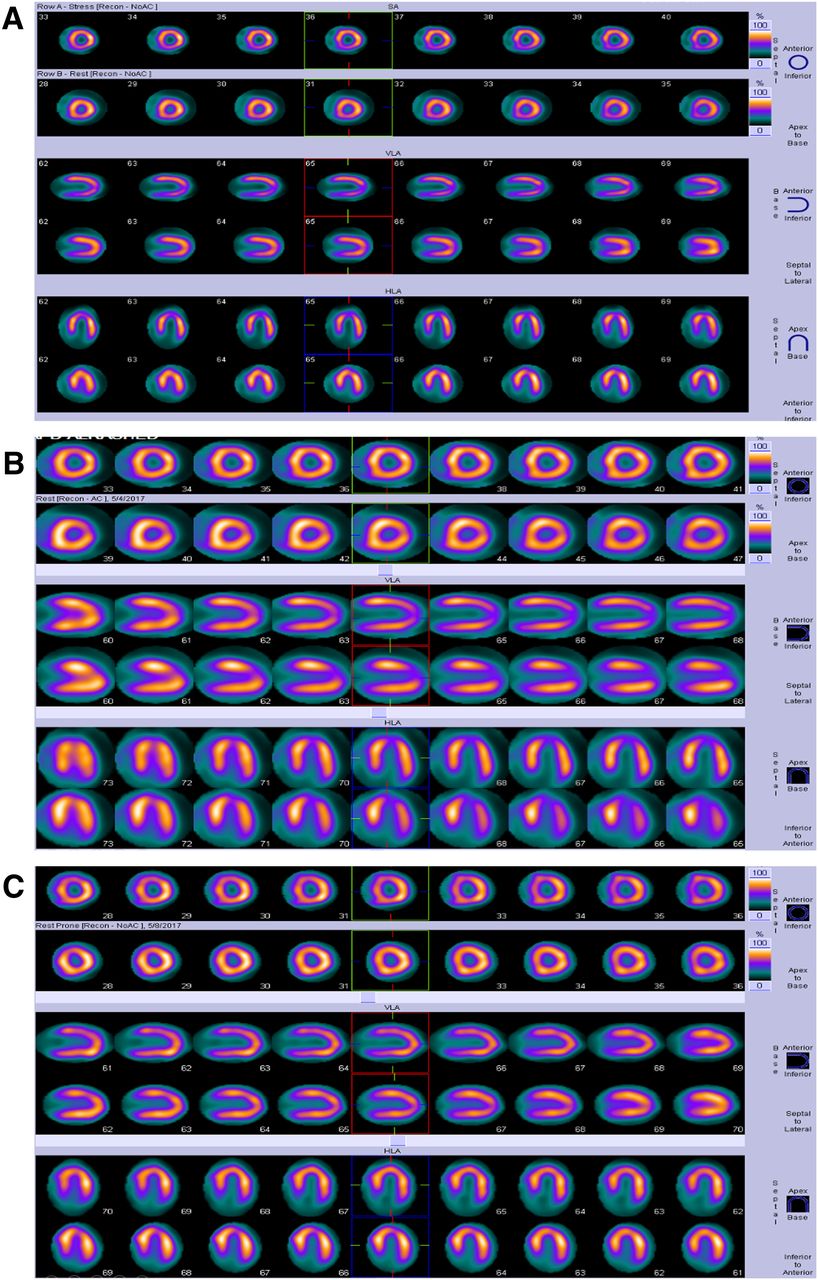
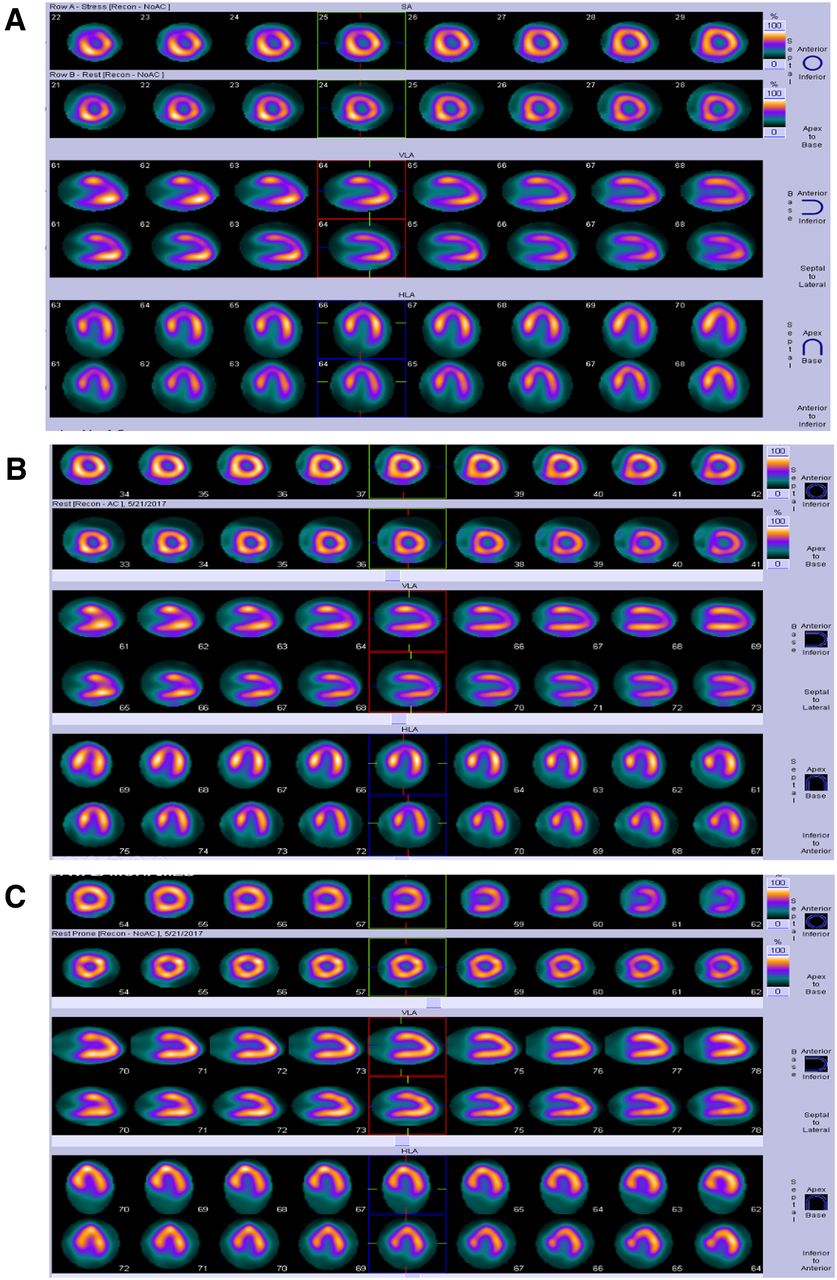
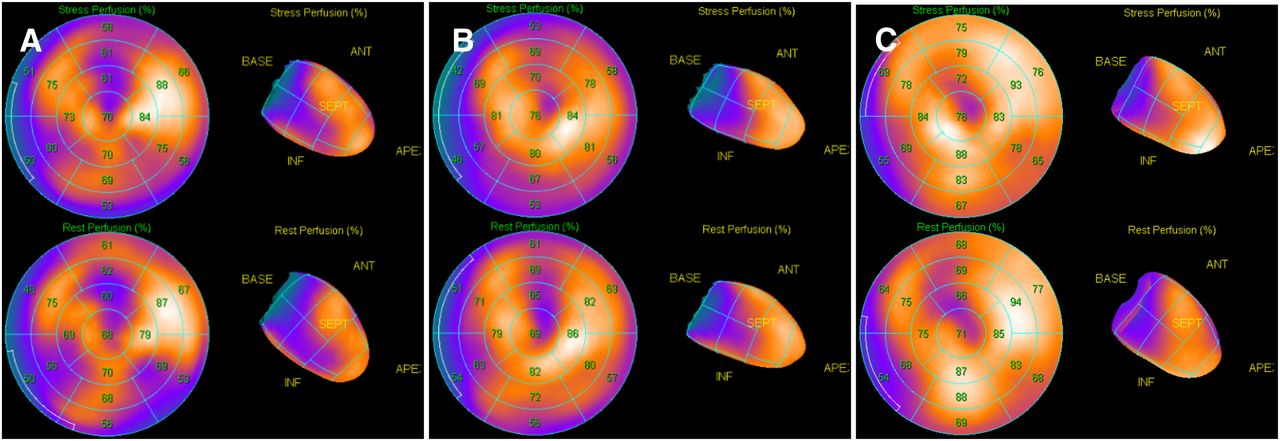
As an example, Figure 3 shows images of a 41-y-old man who was neither diabetic nor hypertensive, had complained of tachycardia and chest pain for 2 mo, and had an ejection fraction of 61%. A hypoperfusion defect seen in the inferior wall, which was subsequently normalized on CT AC and prone images. In another example, Figure 4 shows images of a 50-y-old woman who was neither hypertensive nor a smoker but had a recent history of diabetes and presented with atypical chest pain for 4 mo and an ejection fraction of 63%. Coronary angiography showed atherosclerotic vessels with no significant stenosis. A hypoperfusion defect in the anteroseptal wall improved with CT AC and prone images. Finally, Figure 5 shows images of a 51-y-old man who was neither diabetic nor hypertensive but complained of chest pain for 2 mo and had an ejection fraction of 58%. A hypoperfusion defect in the inferior wall normalized with CT AC and prone images. Polar maps showed the differences between no-AC, CT AC processing, and prone processing.
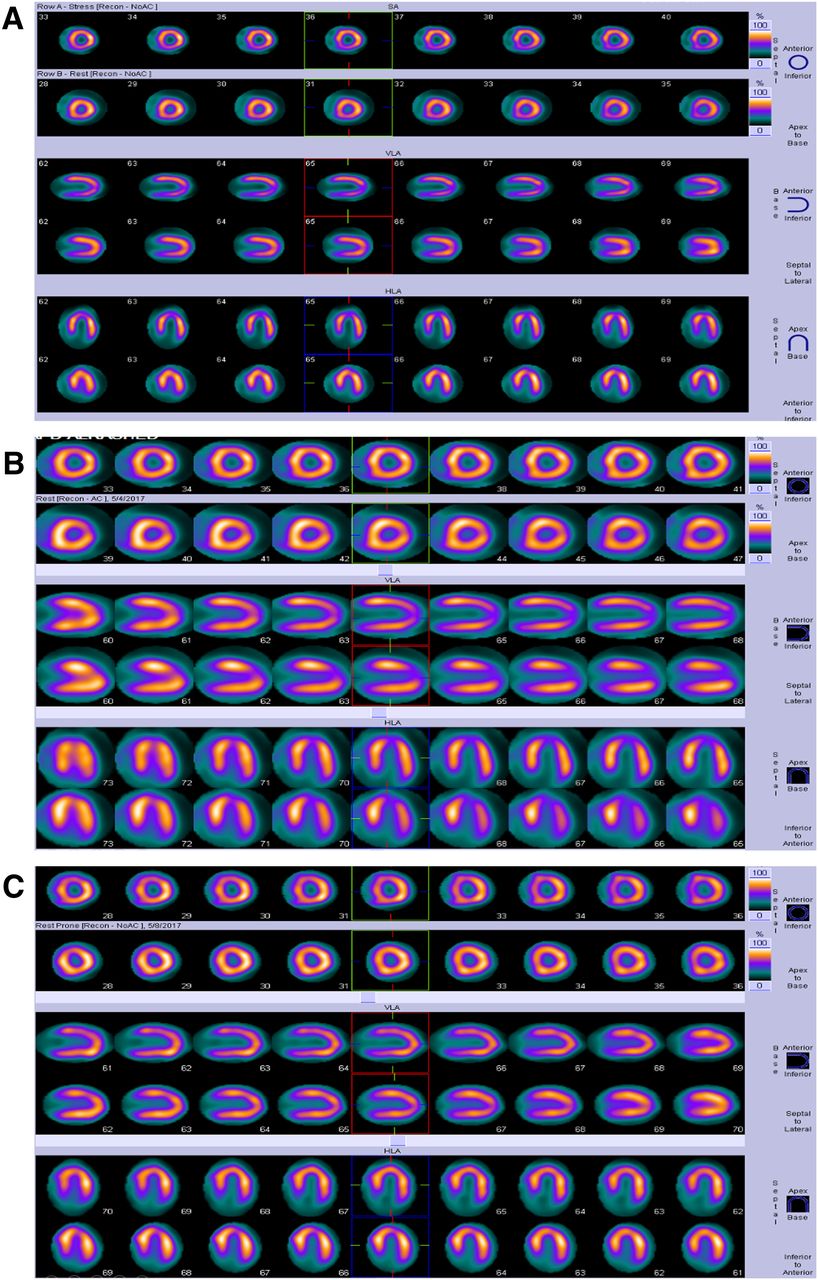
(A) No-AC images showing mild reversible inferior wall hypoperfusion defect. (B) Stress/rest CT AC images showing normalization of inferior wall hypoperfusion defect. (C) Stress/rest prone images showing normalization of inferior wall hypoperfusion defect.

(A) No-AC images showing moderate reversible hypoperfusion defect in anteroseptal wall. (B) Stress/rest CT AC images showing partial improvement of anteroseptal wall defect. (C) Stress/rest prone images showing complete resolution of anteroseptal wall defect (C).
(A) No-AC images showing hypoperfusion defect in inferior wall. (B) Stress/rest CT AC images showing partial improvement of inferior wall defect. (C) Stress/rest prone images showing complete resolution of inferior wall defect.
DISCUSSION
Soft-tissue attenuation is considered one of the main limitations of MPI. Therefore, the use of additional techniques to overcome this problem has been proposed. In our study, we evaluated the role of prone and CT AC imaging and tried to postulate which technique is collectively better. We found that more than half of the hypoperfusion defects elicited in uncorrected images would have been falsely interpreted as true defects in the absence of additional AC techniques. Prone imaging corrected 49% of these defects and CT AC corrected 53%, for an overall accuracy of 91% for prone imaging and 94.3% for CT AC imaging.
Mathur et al. found that 581 of 1,383 (42%) initial stress MPI studies showed normal results, whereas subsequent use of CT AC increased the normal rate to 90% (1,247/1,383). According to our results, CT AC imaging results were largely comparable to those of prone imaging (13).
Malkerneker et al. compared supine stress/rest no-AC with supine stress/rest CT AC and stress/rest prone imaging in 334 patients (14). They found that the percentages of studies yielding normal results were 61.4%, 82.9%, and 90.4% for no-AC, prone imaging, and CT AC, respectively. The authors proved that the combination of supine no-AC and CT AC images is superior to that of supine no-AC and prone images (P = 0.01) (14). They also postulated that the addition of prone imaging does not significantly alter the number of equivocal interpretations, compared with the CT AC results. However, in the absence of CT AC images, prone imaging provides significantly fewer equivocal results than standard supine no-AC imaging (14). This conclusion largely coincides with our results, but although CT AC was slightly better than prone imaging, both techniques showed statistically significant agreement.
Stathaki et al. showed comparable results proving that prone imaging improved the specificity and normalcy rates in anterior wall defects, with 63.1% of the defects disappearing in the prone images (5).
Furthermore, our study revealed that sensitivity, specificity, and diagnostic accuracy were 100%, 90.3% and 94.3%, respectively, for CT AC imaging versus 100%, 83.8%, and 91%, respectively, for prone imaging. The 100% sensitivity is attributed to the small sample size; moreover, we did not encounter any false-negative results for either CT AC or prone imaging. In fact, many papers have revealed an increase in specificity and diagnostic accuracy without any effect on sensitivity. Slomka et al., who evaluated the value of quantitative supine–prone imaging in detection of CAD and normalcy rates in women, indicated that it increased the specificity and normalcy rate without altering sensitivity (15). Slomka et al. also reported that CT AC improved sensitivity, specificity, and diagnostic accuracy for detection of CADs (15).
On the other hand, Sharma et al. found that CT AC had advantages in ruling out significant CAD and reducing false-positive results but that, nevertheless, its use might have compromised the sensitivity of the study (16). Their results are truly different from ours; likely due to our small sample size. Also, Raza et al. showed that sensitivity, specificity, and diagnostic accuracy for detection of CAD were 100%, 11%, and 79%, respectively, for no-AC images and 66%, 78%, and 68%, respectively, for CT AC, implying that CT AC decreased both the sensitivity and the diagnostic accuracy—a finding that is totally different from our results (17).
The main limitation of our study was the small sample size. Also, the prone position was not comfortable for many women or for extremely obese patients. Moreover, all included patients were derived from one center. In addition, quantification data were not statistically analyzed, but they were taken into consideration when the cases were being interpreted.
CONCLUSION
The use of SPECT/CT and prone imaging as AC techniques increased the specificity and diagnostic accuracy of MPI; this increase, in return, could raise the possibility that a stress-only study might be performed. The use of prone imaging as an AC method was relatively better than CT in correcting anterior wall attenuation, while CT as an AC method was relatively better than prone imaging in correcting inferior wall attenuation. Both AC methods agreed well with the final diagnosis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Dec. 24, 2020.
REFERENCES
- Received for publication August 27, 2020.
- Accepted for publication October 22, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.