


Abstract
90Y radioembolization is a safe and efficacious treatment option for many patients with unresectable hepatocellular carcinoma. Potential candidates for radioembolization, based on clinical criteria, undergo 99mTc-labeled macroaggregated albumin imaging to determine the extent of hepatopulmonary shunting. Dose selection is based on results from shunt imaging and can exclude patients from radioembolization therapy. We present a case of miscalculated lung shunt fraction and the circumstances that led to the critical error.
- 90Y radioembolization
- lung shunt fraction
- 99mTc-labeled macroaggregated albumin
- hepatocellular carcinoma
Millions of individuals worldwide have hepatocellular carcinoma, the most common primary liver malignancy. In addition to resection, safe and effective treatment options for many patients include transplantation, radiofrequency ablation, chemoembolization, and systemic chemotherapy (1). In 90Y radioembolization, glass or resin beads fixed with the β-particle–emitting radioisotope 90Y are selectively injected via a microcatheter to deliver high doses of radiation to the tumor. Before treatment, patients undergo important planning studies, including mapping angiography and 99mTc-labeled macroaggregated albumin (99mTc-MAA) imaging. Information from these studies is used to minimize the risk of nontarget radiation injury to the gastrointestinal tract and lungs (2).
Radiation pneumonitis is a known complication of 90Y radioembolization, and the risk of this complication is related to radiation delivered unintentionally to pulmonary tissue via hepatopulmonary shunting (3). 99mTc-MAA imaging is therefore critical for 90Y patient selection, a requirement for shunt reduction intervention and radioembolization dosing. After 99mTc-MAA injection, anterior and posterior planar imaging is performed. The geometric mean is calculated as the square root of the product of counts for regions of interest (ROIs) from anterior and posterior planar images (Fig. 1). Many vendors’ software generates a single geometric mean image, which is a composite of the anterior and (flipped) posterior images, and from this the geometric mean counts for each ROI are obtained. The lung shunt fraction (LSF) is calculated as the counts from the lung ROI divided by the total counts for the lung and liver ROI (from the geometric mean image) (Fig. 1). For radioembolization therapy, an LSF of more than 20% or an LSF that results in an estimated lung radiation exposure of more than 30 Gy (based on the planned 90Y dose) is considered a contraindication (4) or requires a significant dose reduction at the risk of reduced treatment efficacy.

Formulas used for calculating geometric mean (for designated ROI) and LSF.
CASE REPORT
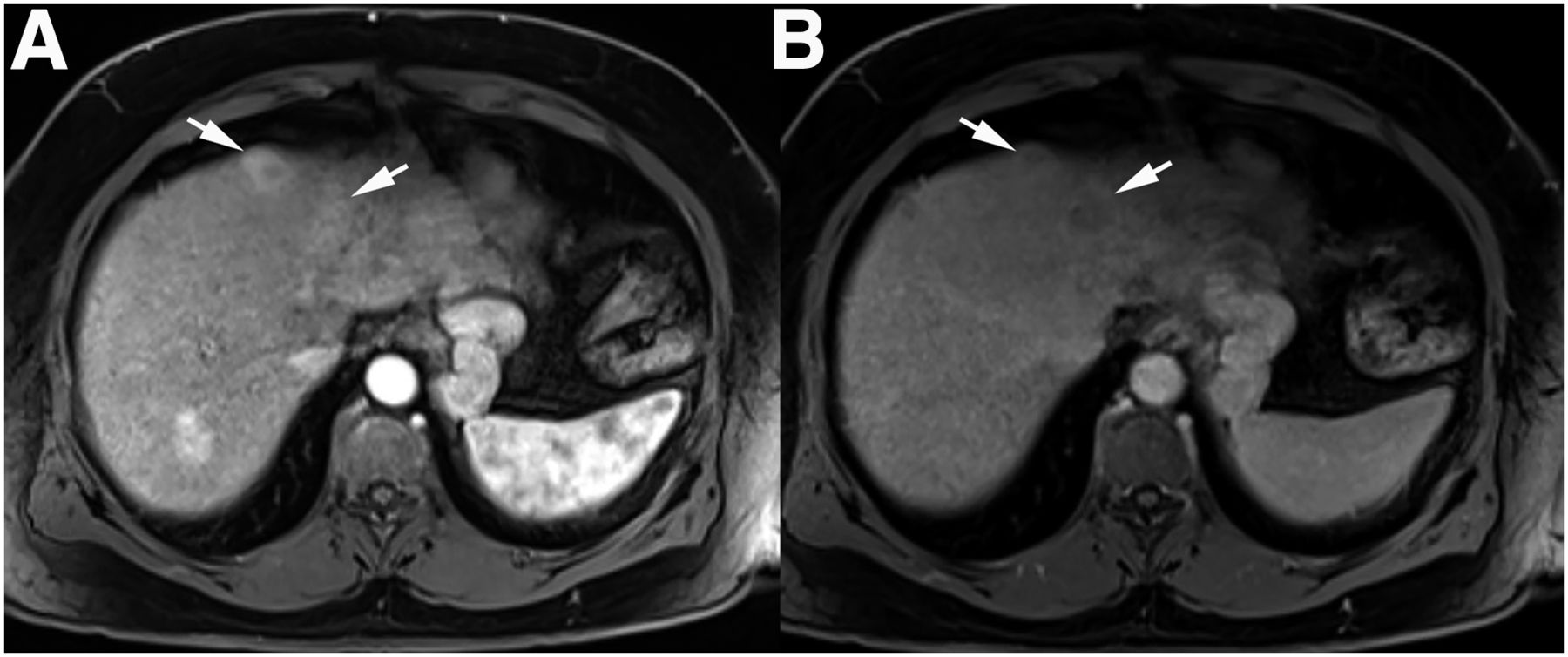
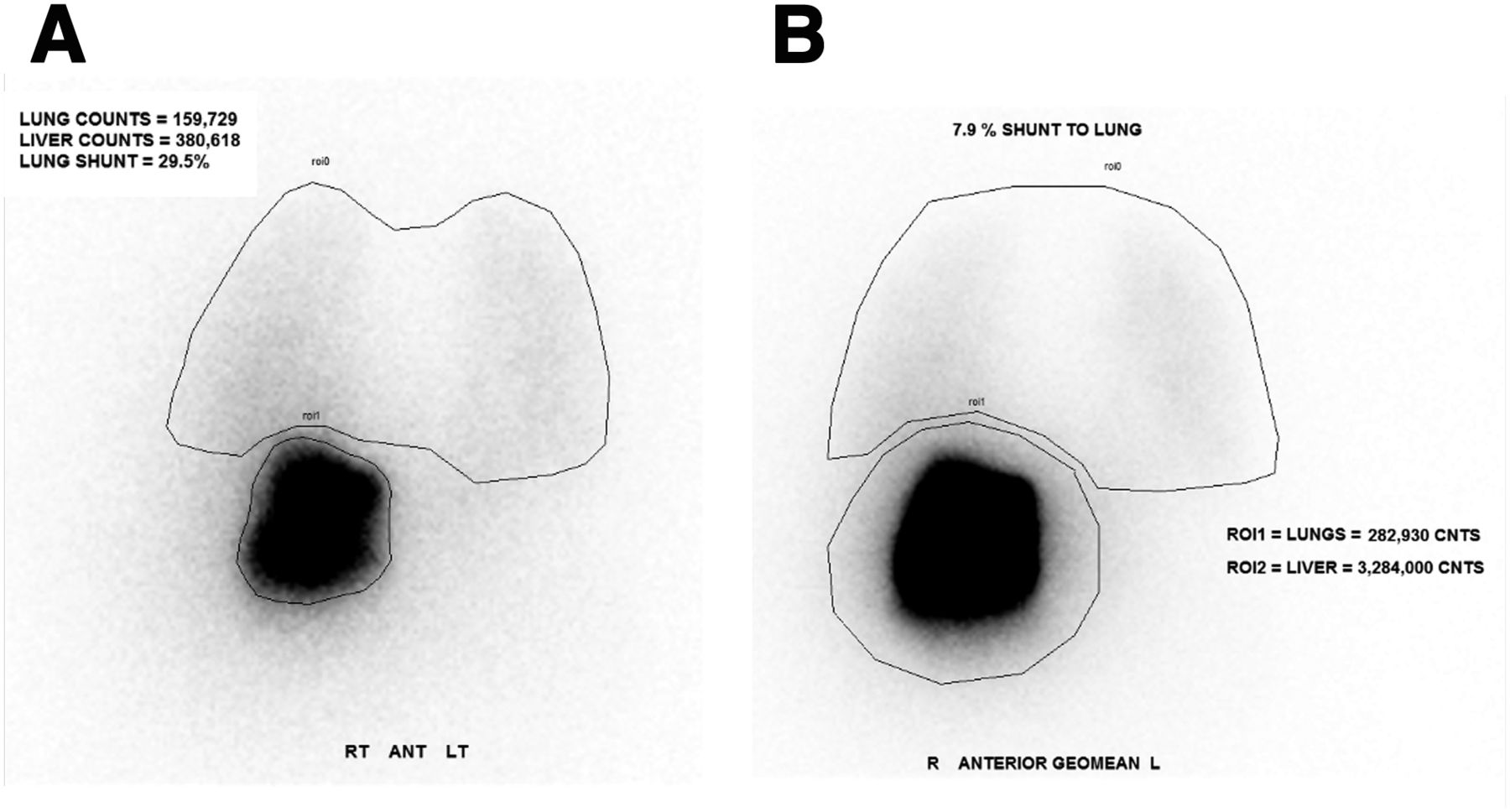
A 65-y-old man with multifocal hepatocellular carcinoma (Fig. 2) underwent evaluation for potential treatment with 90Y radioembolization. Pretreatment 99mTc-MAA imaging was performed to assess hepatopulmonary shunting. ROI determination and postprocessing were completed per standard procedures, and the LSF was initially calculated as 29.5% (Fig. 3A). The nuclear medicine physician noted a potential error in shunt fraction based on visual assessment and requested that the image be reprocessed. After reprocessing, the LSF was recalculated as 7.9% (Fig. 3B). The patient ultimately received a successful 90Y radioembolization.

Contrast-enhanced axial T1-weighted images during arterial (A) and delayed (B) phases demonstrate washout within 2 adjacent hepatocellular carcinomas (arrows) located anteriorly within segment 4A of liver.
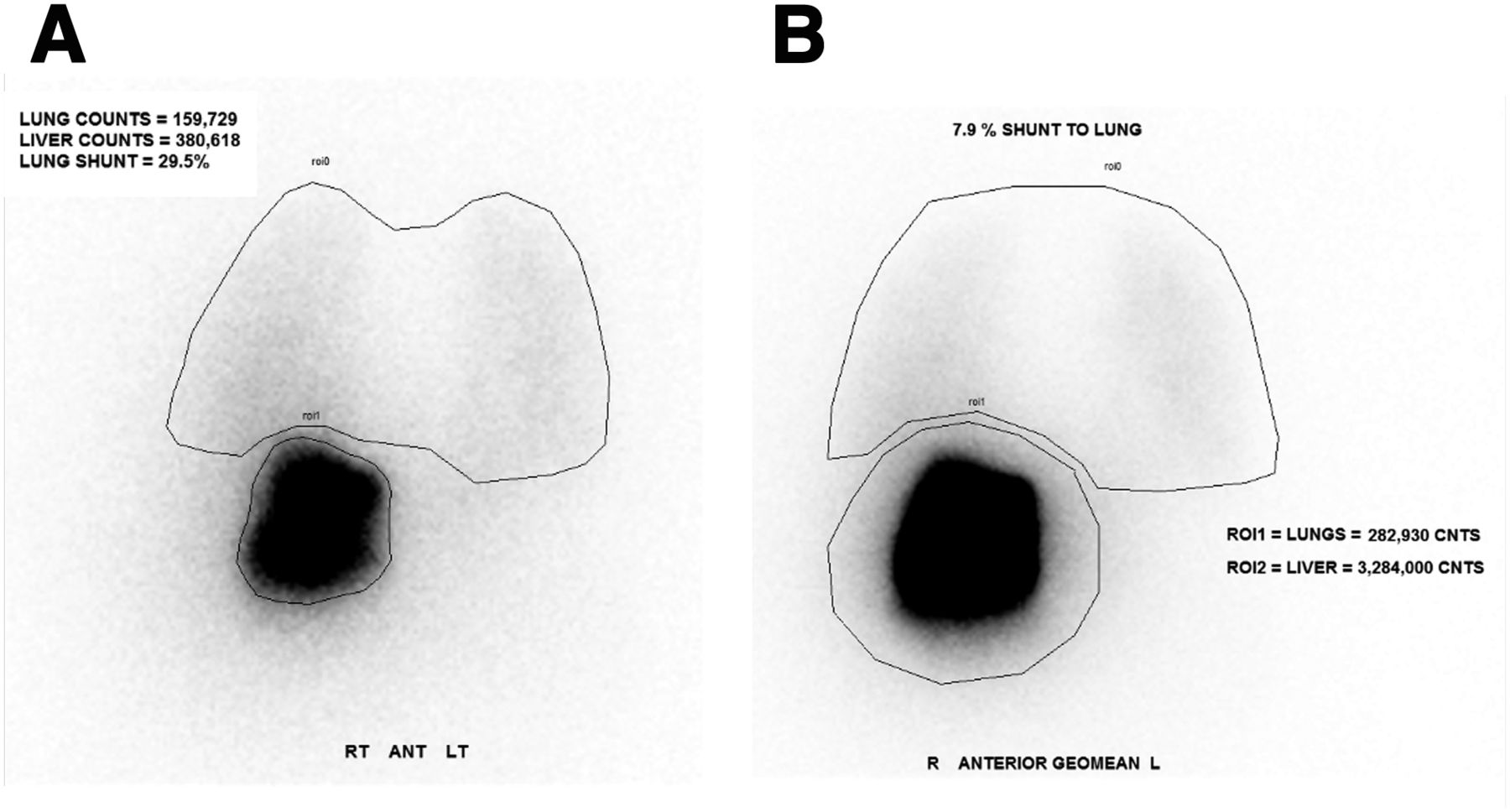
(A) Initial 99mTc-MAA (flipped) posterior planar image with lung and liver ROIs. Incorrect LSF calculated was 29.5%. (B) 99mTc-MAA geometric mean image with lung and liver ROIs. Correct LSF calculated was 7.9%.
DISCUSSION
This case highlights a critical source of error that can occur during LSF calculation by 99mTc-MAA imaging. Initially, the nuclear medicine technologist mistakenly labeled the raw data from a posterior flipped view as the geometric mean image; thus, the ROI contained counts from only the posterior view. The initial incorrect LSF (using only the flipped posterior planar image) was 159,7289 ÷ (159,7289 + 380,618) = 0.295 (Fig. 3A). The correct LSF (based on counts from the geometric mean image) was 282,930 ÷ (282,930 + 3,284,000) = 0.079 (Fig. 3B).
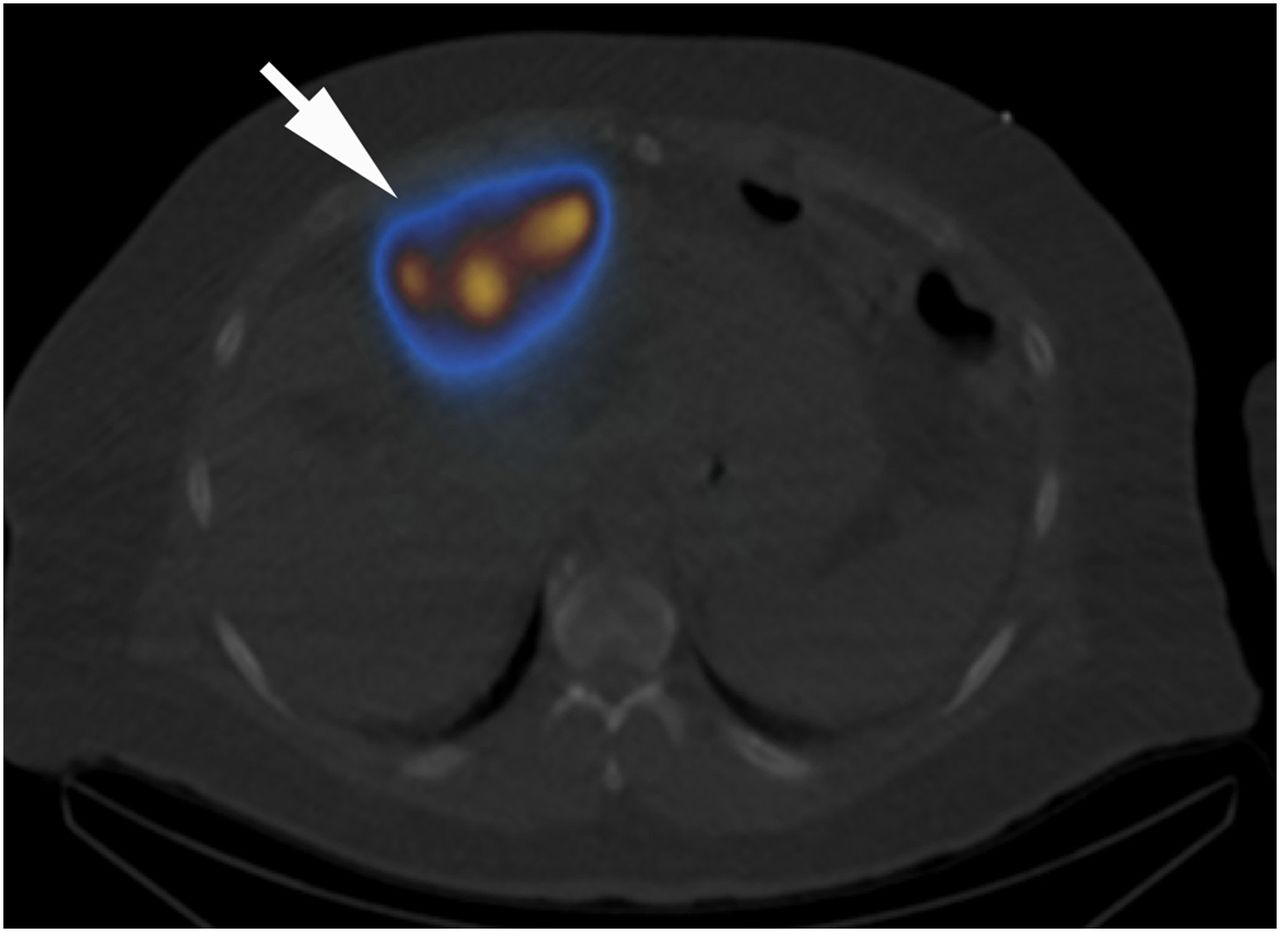
The initial shunt fraction of 29.5% would be a contraindication to 90Y radioembolization, and the error thus would have mistakenly precluded the patient from therapy. Although differences in ROI size can alter count totals, the variance in this case was too large to be attributed to this factor alone because the error led to a 3.5 greater discrepancy between the calculated LSFs. The initial artifactually low liver count was especially exacerbated by the anterior position of the tumor (Fig. 4), as only the (flipped) posterior planar image was used for the initial LSF calculation. Our nuclear medicine laboratory has scanners from multiple vendors, and this error likely occurred because of confusion over how the geometric mean is displayed or calculated among different vendors.
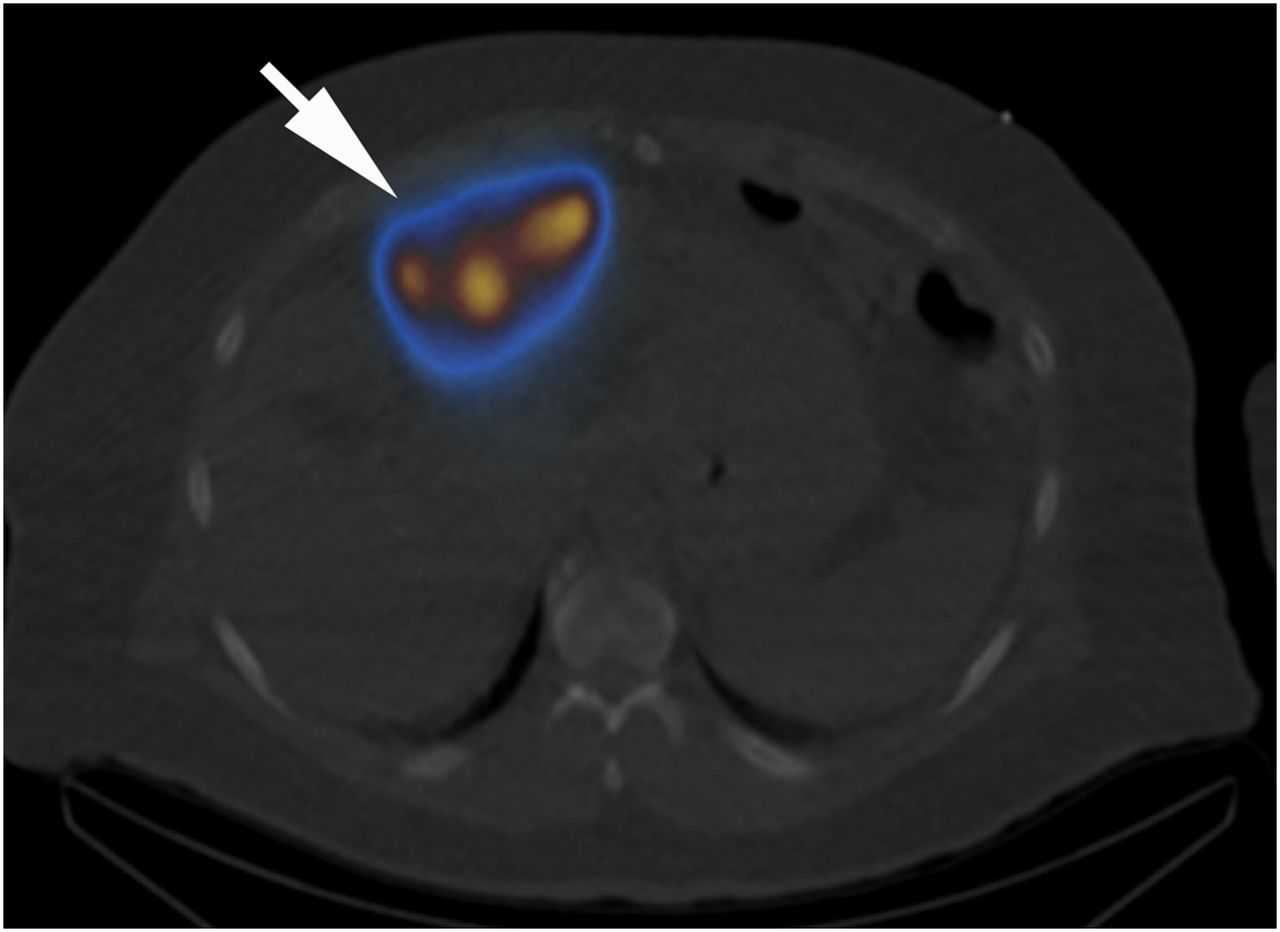
Selected axial 99mTc-MAA SPECT/CT image confirming radiotracer delivery to anteriorly positioned hepatocellular carcinomas (arrow).
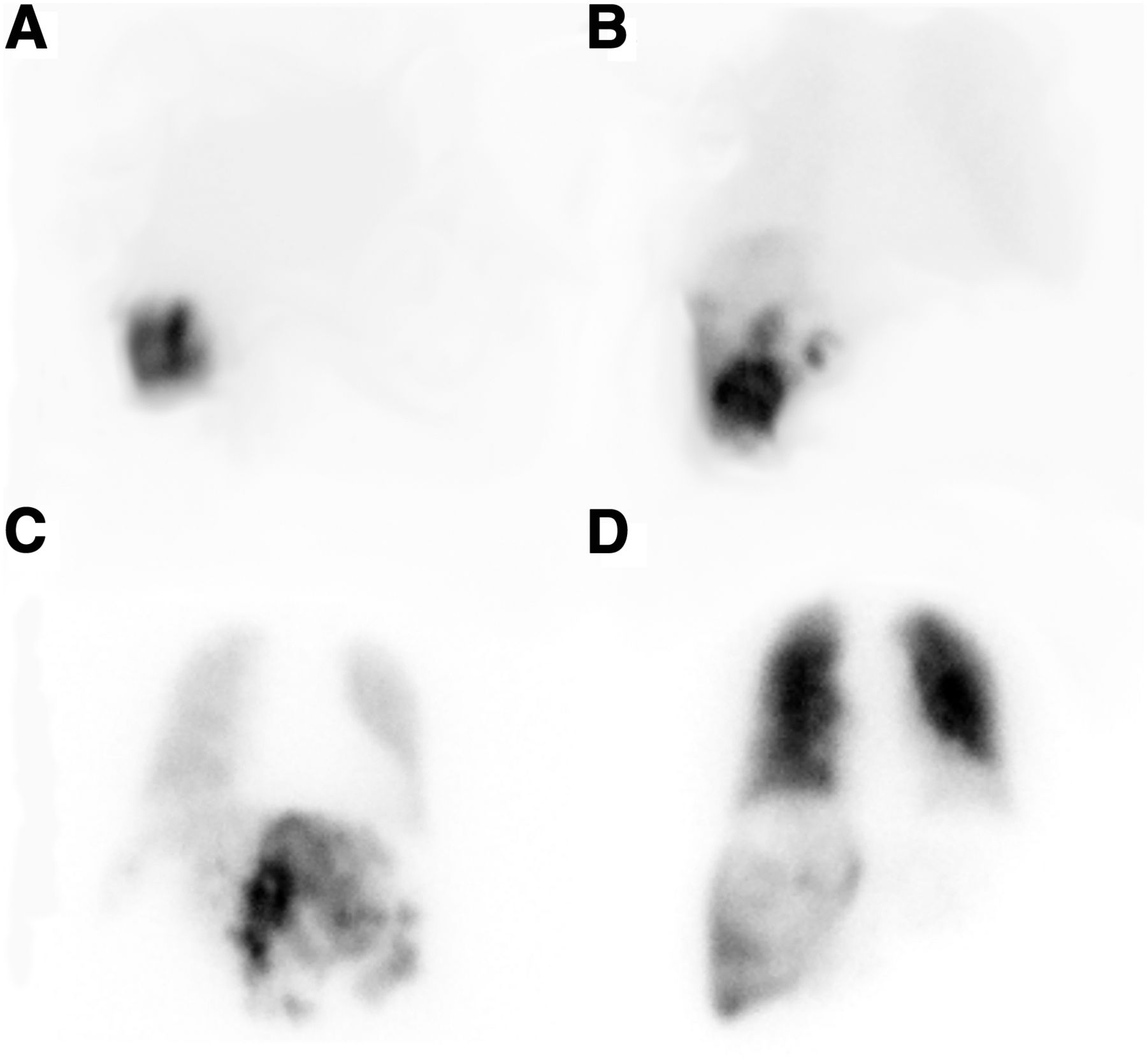
To overcome this potential error, the nuclear medicine technologist may benefit from having easy access to a vendor-specific guide for the accurate calculation of LSF. Labeling the images with “geometric mean” instead of “ROI” or “counts,” as in our case (Fig. 3), may act as a reminder to use the correct data source. Further, if the nuclear medicine technologist (or nuclear medicine physician) needs to actively window the raw data to discriminate the lung ROI (or liver ROI) from the background, then the LSF should be low. Nuclear medicine technologists and nuclear medicine physicians may also use the provided LSF visual reference (Fig. 5) as a guide when visually assessing the adequacy of the LSF from the raw data images.
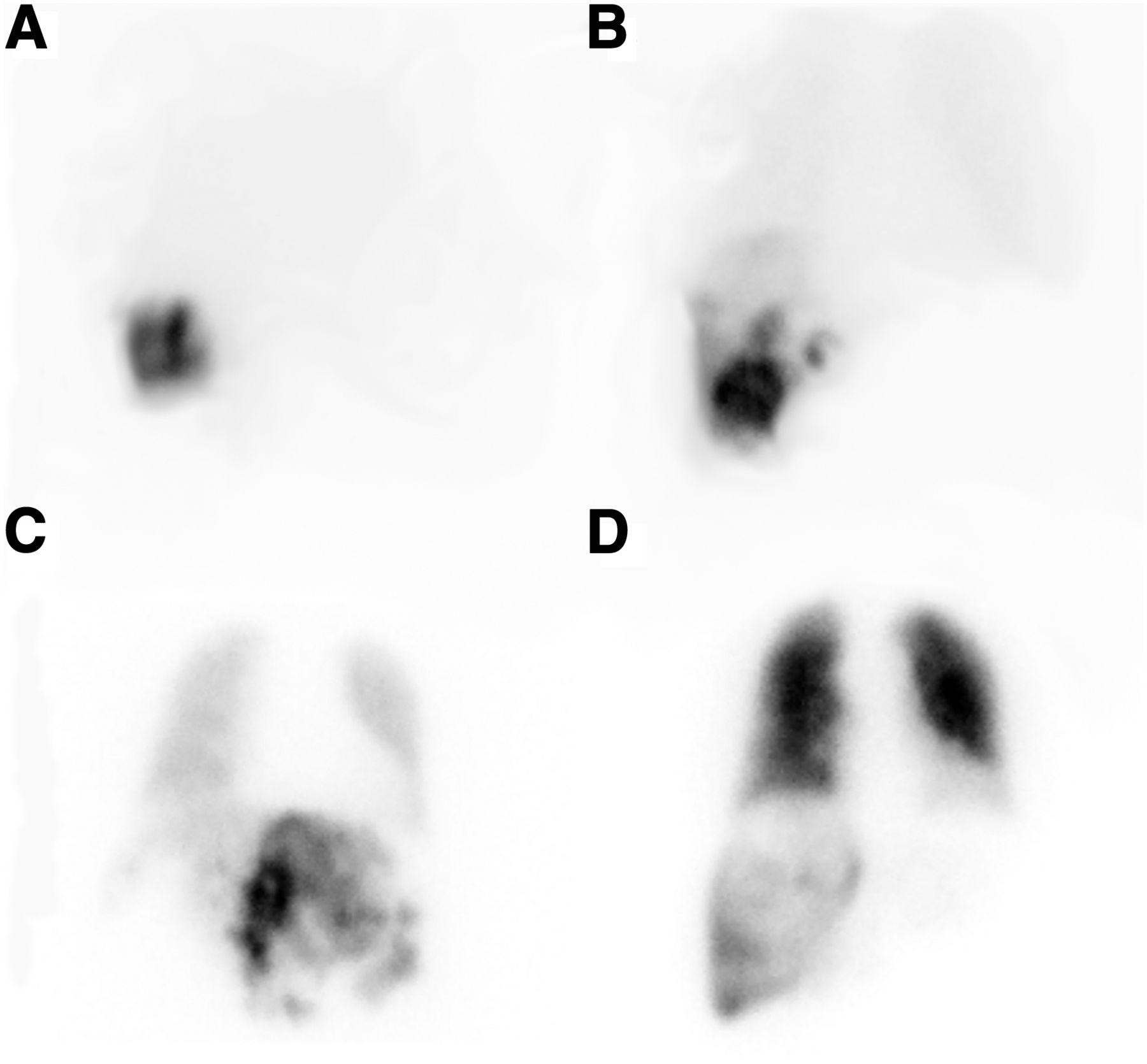
Lung shunt fraction visual reference for LSFs of 3% (A), 15% (B), 37% (C), and 79% (D).
CONCLUSION
99mTc-MAA imaging and LSF calculations are important steps in pretreatment assessment for patients before 90Y radioembolization for hepatocellular carcinoma. Confirming that the visual assessment and calculated LSF are concordant ensures that the LSF has been calculated appropriately from the geometric mean image during processing.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 6, 2019.
REFERENCES
- Received for publication July 29, 2019.
- Accepted for publication October 7, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}