


Abstract
Brown adipose tissue (BAT) has been widely reported to affect the efficacy of 18F-FDG PET in oncology. Several small studies have found that warming the patient both before 18F-FDG injection and during the uptake phase can reduce the frequency of BAT uptake. Pharmaceutical approaches such as propranolol and diazepam have also been used. Methods: We describe two case studies that demonstrated the impact of combined patient warming and diazepam administration on BAT uptake in pediatric 18F-FDG PET images. To support these findings, we performed a retrospective analysis of 139 patients: 71 who received warming only and 68 who received warming combined with diazepam. Results: BAT uptake was significantly less frequent in patients who received diazepam (16.2%) than in those who did not (33.8%) (P = 0.0167), particularly in female patients (7.4% vs. 26.7%) (P = 0.0486). Conclusion: Although patient warming alone reduces the frequency of BAT uptake, the addition of diazepam to patient warming significantly furthers the reduction in young patients, particularly female patients.
Brown adipose tissue (BAT) is responsible for nonshivering thermogenesis, which produces heat in the BAT cells to maintain body temperature (1). BAT is highly vascular and mitochondria-rich compared with white adipose tissue (1). Because BAT is metabolically stimulated by the sympathetic nervous system, both metaiodobenzylguanidine and sestamibi have been used to document the distribution of BAT (1). BAT utilizes glucose as a source of adenosine triphosphate to generate heat, providing a pathway by which 18F-FDG can localize within BAT (1).
BAT has been widely reported to affect the efficacy of 18F-FDG PET in oncology. The incidence of BAT uptake on 18F-FDG PET images varies, with one report indicating 2.5% in 638 patients (2), another indicating 3.6% in 1,495 patients (3), and a third, 3.7% in 863 patients (4). BAT is typically found in the supraclavicular area but can also be seen in the neck, paravertebral, paraaortic, and suprarenal areas (5). Combination imaging with PET and CT can help differentiate BAT on the basis of anatomic localization and measurement of tissue density (4,6). Nonetheless, BAT remains a confounder on oncologic 18F-FDG PET studies, with the potential for both false-positive and false-negative results.
Several important factors, particularly age and sex, predispose BAT accumulation of 18F-FDG. BAT plays an important role in maintaining the core body temperature of children (7), and consequently, one might expect to see a greater incidence of BAT uptake on pediatric 18F-FDG PET scans. Indeed, in two studies, categorization of patients with BAT uptake into pediatric and adult populations indicated the same: 13.6% in those under 18 y versus 2.8% in adults (3), and 23.8% in those under 18 y versus 5.9% in adults (8). Furthermore, several reports indicated that BAT uptake is more common in females (2,7,9). BAT is also, understandably, more common in colder seasons (e.g., winter vs. summer) (1,10).
Given the role of BAT in managing core body temperature, patients have been warmed to reduce the likelihood of BAT uptake on 18F-FDG PET images. Several small studies found that warming the patient both before 18F-FDG injection and during the uptake phase reduced the frequency of BAT uptake (11–13). In a large study of 300 consecutive patients, Skillen et al. (1) showed that warming the patient reduced the frequency of BAT uptake by 78%, from 15.3% without warming to 3.3% with warming. Although warming provides a noninvasive, inexpensive, and universal approach to BAT reduction, warming has several shortcomings that make it ineffective as a stand-alone solution. First, the approach assumes that core body temperature and BAT activation can be managed using a short-term strategy. O’Loughlin et al. (10) showed that the sympathetic activation associated with ambient thermal conditions reflects a 3-d window rather than the period contemporaneous with 18F-FDG injection. Thus, warming a patient for 90 min may not be effective if that patient was exposed to cooler ambient temperatures with no warming strategy over the preceding days. Second, the greater frequency of BAT activation in children may limit the success of warming strategies, leading to potential false-positive and false-negative findings.
Several pharmacologic approaches have been used to minimize the frequency of BAT uptake on 18F-FDG PET images. Propranolol (a nonselective β-blocker) has been the most widely reported (14–16). It blocks epinephrine and norepinephrine on β-receptors and, thus, prevents BAT stimulation to produce heat. In a study of 11 patients with BAT uptake seen on baseline images, the uptake was eliminated in all cases by 80 mg of oral propranolol before the administration of 18F-FDG (14); in a study of 40 patients with baseline BAT uptake on 18F-FDG PET images, 40 mg of oral propranolol resolved the uptake in 90% of cases (15); and in a study of 26 patients with baseline BAT uptake, 20 mg of oral propranolol eliminated the uptake in 92.3% of cases (16).
Importantly, anxiety and stress have been reported to both increase muscle uptake of 18F-FDG (17) and activate BAT (15), suggesting a role for diazepam. In anxious patients, diazepam has been used to reduce muscle uptake, and the impact of diazepam on biodistribution initially caused BAT uptake to be interpreted as muscle (4). Although diazepam might be preferred in children, success has been limited and outcomes have been dose-dependent. A 0.10 mg/kg dose of oral diazepam was 100% successful in eliminating BAT uptake in a small population of children; however, lower doses of 0.06 mg/kg resolved the BAT uptake in only 29.4% of the children (18). Because diazepam is a lipid-soluble drug stored in adipose tissue, its success will be dose-dependent and subject to associated pharmacokinetic influences.
MATERIALS AND METHODS
Two case studies that demonstrated the impact of combined patient warming and diazepam administration on BAT uptake in pediatric 18F-FDG PET images are described. To support these findings, a retrospective analysis of 139 patients 9–21 y old was undertaken: 71 consecutive patients before the addition of diazepam to a warmed-blanket protocol and 68 after (0.27 mg of diazepam per kilogram, to a maximum of 10 mg). In the warmed-blanket protocol, the patients were covered with prewarmed blankets starting 30 min before the administration of 18F-FDG. For the patients additionally receiving diazepam, the dose was administered orally 30 min before the 18F-FDG. All patients fasted for 6 h before the study, and all studies were performed on a Discovery VCT (GE Healthcare).
Statistical significance was calculated using χ2 analysis for nominal data and the Student t test for continuous data. F test ANOVA was used to determine statistically significant differences within grouped data. A P value of less than 0.05 was considered significant.
RESULTS
Case 1
A 16-y-old boy with Hodgkin lymphoma was given an injection of 18F-FDG (399.6 MBq [10.8 mCi]) and scanned 1 h later. He had been covered with warmed blankets in a warm room before receiving the injection and throughout the uptake phase. Significant uptake in the neck, supraclavicular, mediastinal, and paravertebral regions raised suspicion of BAT uptake, with its potential to confound disease detection (Fig. 1). The study was repeated after chemotherapy. This time, in addition to the warmed blankets and warm room, 10 mg of diazepam was given orally 1 h before the 18F-FDG injection (270.1 [7.3 mCi]). The scan demonstrated a largely clear neck-and-chest field, with some mild uptake in the right lateral chest and right axilla. In this case, it was difficult to discern how much of the uptake at baseline was disease versus BAT and whether the uptake after chemotherapy was residual or new. Nonetheless, the combination of warming and diazepam effectively eliminated the BAT uptake.
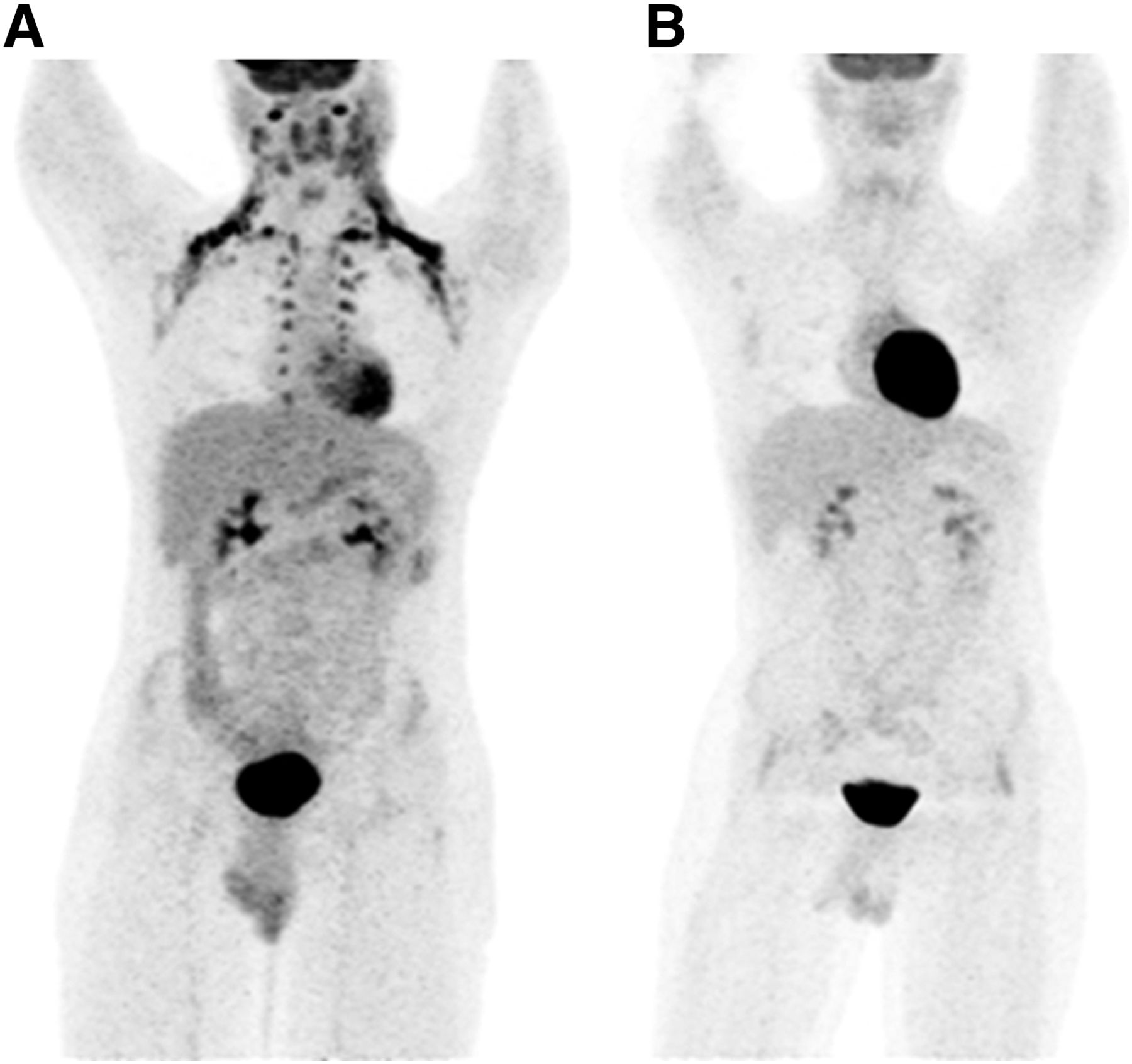
(A) Baseline 18F-FDG PET study with warmed blankets and increased room temperature demonstrated marked BAT uptake. (B) Postchemotherapy follow-up 18F-FDG PET study in same patient with warmed blankets, increased room temperature, and 10 mg of diazepam demonstrated elimination of BAT uptake.
Case 2
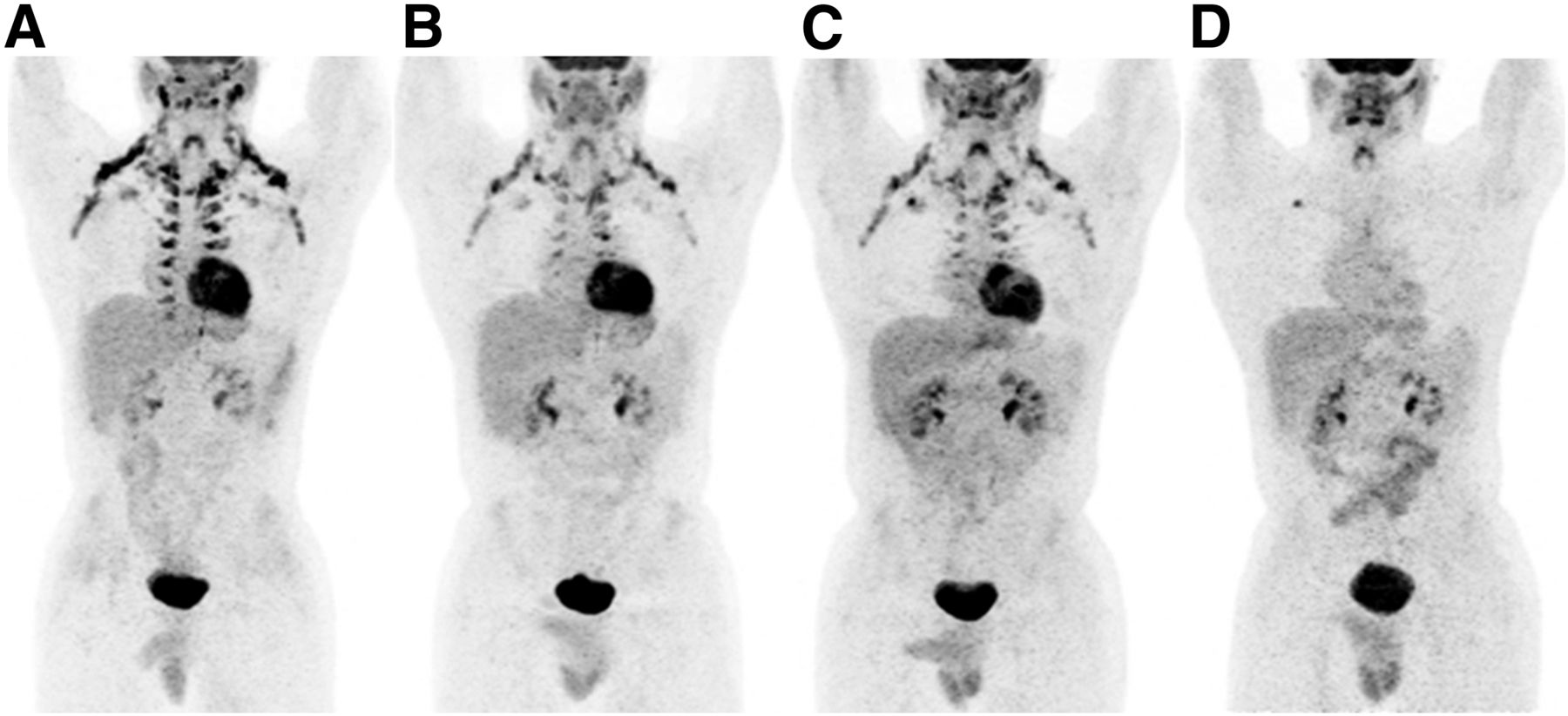
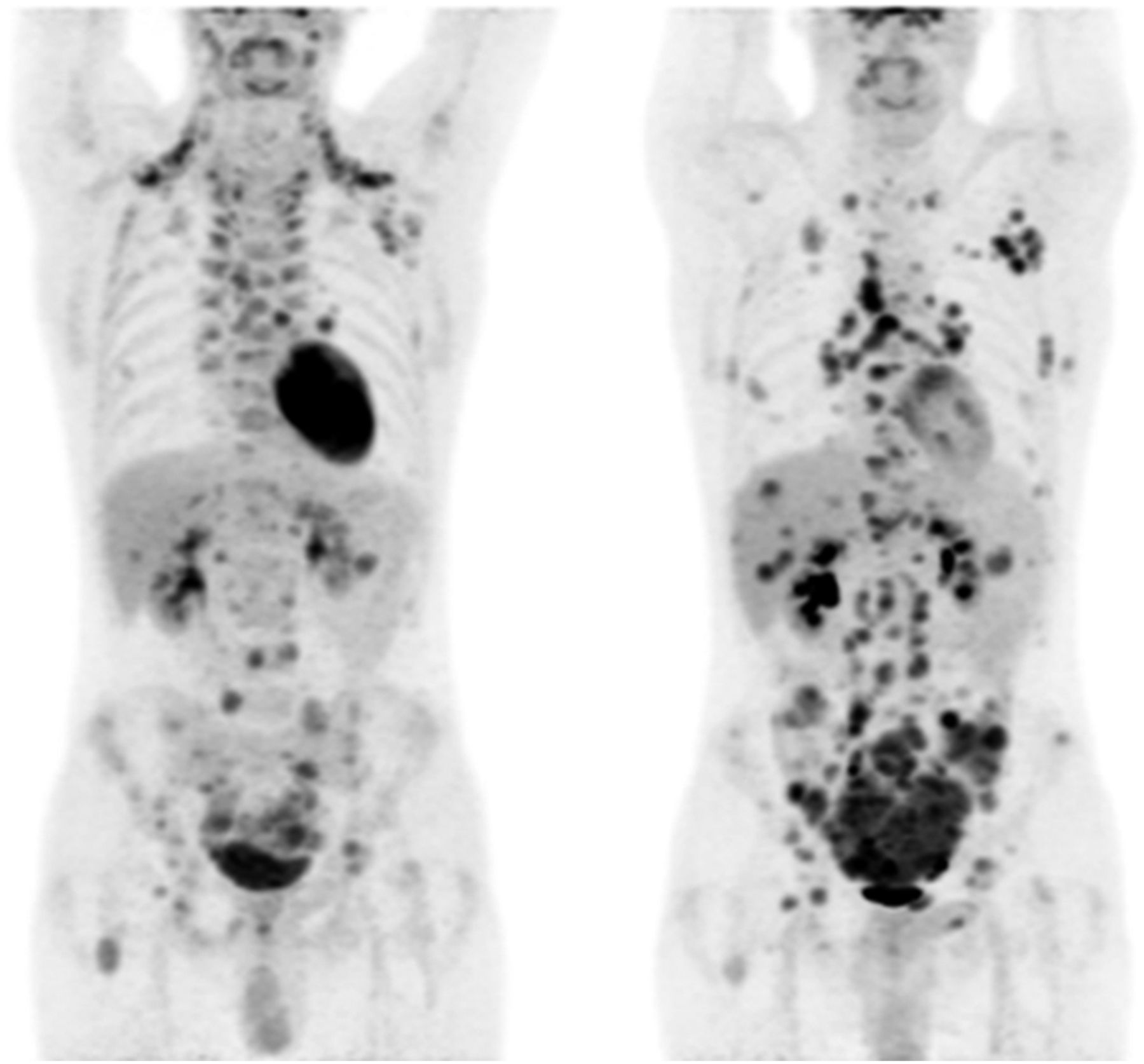
A 17-y-old boy with non-Hodgkin lymphoma underwent 4 18F-FDG PET scans over 9 mo. The first 3 scans used 455.1 MBq (12.3 mCi), 503.2 MBq (13.6 mCi), and 492.1 MBq (13.3 mCi) of 18F-FDG at baseline, 3 mo, and 6 mo, respectively; the patient was covered with warmed blankets before administration of the 18F-FDG and during the uptake phase. On the images, marked uptake in the neck, supraclavicular, mediastinal, and paravertebral regions suggested extensive BAT uptake of 18F-FDG (Fig. 2). At 9 mo, the patient was scanned with 388.5 MBq (10.5 mCi) of 18F-FDG using the same warmed-blanket protocol plus 10 mg of diazepam. The images showed suppression of BAT uptake, washout of cardiac uptake, and a focal area of uptake in the right upper chest representing new disease. On the baseline and 3-mo scans, this area had shown a mild, diffuse accumulation of 18F-FDG likely to represent BAT uptake. On the 6-mo scan, however, this area had a superimposing focus of uptake representing new disease, but the finding was noted only retrospectively after BAT uptake had been suppressed with diazepam on the 9-mo scan.

(A) Baseline 18F-FDG PET study with warmed blankets showed marked uptake in the neck, supraclavicular, mediastinal, and paravertebral regions suggestive of extensive BAT uptake. (B) Three-month study with warmed blankets showed no change from baseline. (C) Six-month study with warmed blankets prospectively showed no significant change from baseline but retrospectively showed apparent increase in focal uptake in right upper chest. (D) Nine-month study with warmed blankets and diazepam showed suppression of BAT uptake and clear demarcation of focal disease in upper right chest.
Retrospective Analysis of 139 Patients
In the retrospective analysis of 139 patients, the sex distribution was statistically significant, with females representing 41% of the population and males 59% (P = 0.034). Overall, 25.2% of patients showed BAT uptake on 18F-FDG PET images, and although not statistically significant, there was a greater frequency of BAT uptake in males (30.5%) than in females (17.5%) (P = 0.0838).
As expected, a statistically significant positive correlation was noted between age and 18F-FDG dose (P < 0.001), but there was no significant relationship between the use of diazepam and 18F-FDG dose (P = 0.886) or between the presence of BAT uptake and 18F-FDG dose (P = 0.554). In addition, there were no significant differences in the distribution of age across sex, season of study, use of diazepam, or presence of BAT uptake (all P > 0.321) (Table 1); in the distribution of sex across season of study (P = 0.865) or diazepam use (P = 0.760); or in the distribution of seasons across use of diazepam (P = 0.289), presence of BAT uptake (P = 0.448), or patient dose (P = 0.619).
Demographic Comparison of Groups
The frequency of BAT uptake was significantly lower in patients who received diazepam (16.2%) than in those who did not (33.8%) (P = 0.0167). In men, the difference was not statistically significant (22% vs. 39%) (P = 0.0931), but in women it was (7.4% vs. 26.7%) (P = 0.0486).
DISCUSSION
BAT is sympathetically activated in response to exposure to cold (1). The impact of cold on 18F-FDG PET studies is the result of prolonged exposure over the days or weeks leading into the 18F-FDG PET study (8); consequently, short-term warming temporally close to the 18F-FDG injection may have limited usefulness in some patients, as the impact on core body temperature will not be sufficient to deactivate BAT uptake. Nonetheless, BAT has also been linked to short-term exposure to cold, and in these cases warming may be an effective strategy to reduce BAT.
Tatsumi (17) used rats to demonstrate that BAT uptake of 18F-FDG was reduced to 16% of the control value by propranolol and to 36% by diazepam. This finding suggests that the medications do not eliminate BAT uptake but simply reduce it. The drug concentrations were much higher (per kg) in that study than would be used in human studies. Effectiveness might best be achieved, therefore, with a combination of medication (propranolol in adults and diazepam in children) and warming.
Although 18F-FDG PET is commonly used for the detection and staging of disease in oncology, it is also widely used to assess myocardial viability (10). Our second case provides an interesting paradox. Although BAT uptake was reduced with warming and diazepam, cardiac uptake was also reduced. A negative impact on cardiac 18F-FDG PET imaging might be expected, as was reported for a study that found patient warming to reduce uptake in both BAT and the heart (Fig. 3) (1). Cardiac glucose metabolism depends on numerous factors, but increased sympathetic activity drives an increased metabolic demand for glucose (10), and cooler ambient conditions may be associated with increased cardiac sympathetic activity.
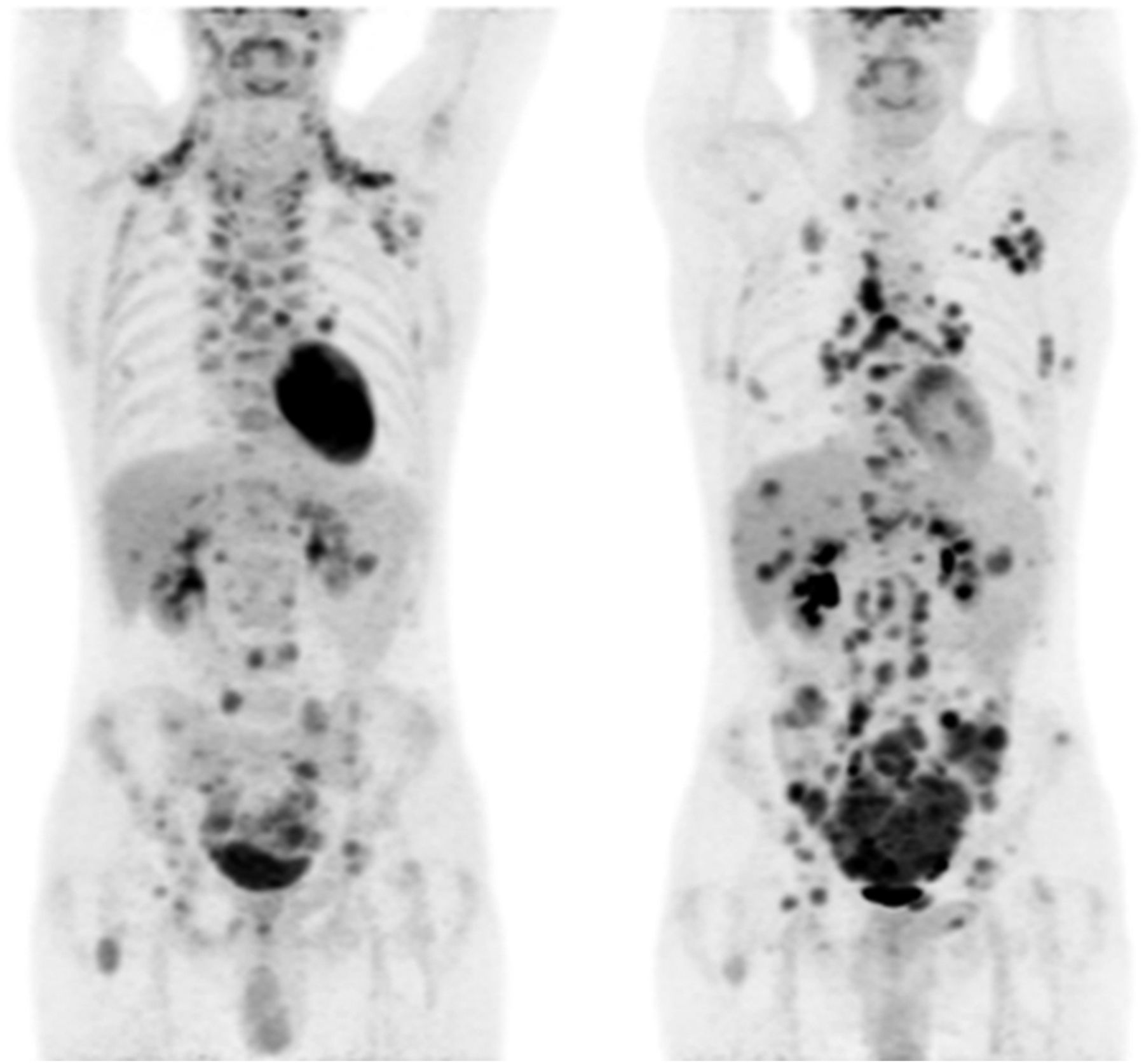
A 28-y-old man with desmoplastic small-round-cell tumor presented in October 2009 for initial 18F-FDG PET study (left) and subsequently in January 2010 (right). Both studies used approximately 270 MBq of 18F-FDG and were obtained after 60-min uptake phase. Initial image was obtained without warming techniques. Follow-up image was obtained with warming intervention. Apart from disease progression, presence and absence of significant BAT accumulation is noted. (Reprinted with permission of (1).)
In the study by Tatsumi (17), diazepam produced a small increase in 18F-FDG uptake, and this finding is concordant with that of Israel et al. (19). This important observation provides crucial insight. In our first case, despite having been warmed, the patient showed prominent uptake in both BAT and the heart, suggesting that raising the ambient temperature is insufficient to overcome sympathetic stimulation of either (in a patient who perhaps has experienced longer-term exposure to cold). After the addition of diazepam to warming, BAT uptake was suppressed but cardiac uptake increased, as was also reported by Tatsumi (17) and Israel (19). Again, this finding suggests that warming alone cannot overcome the sympathetic stimulation caused by exposure to cold. In our second case, on the other hand, the patient showed a marked decrease in cardiac uptake and suppression of BAT uptake in the 9-mo study. This finding suggests that warming was inadequate in the first 3 studies, because there was no decrease in cardiac uptake. It also suggests that warming played a significant role (combined with diazepam) in reducing both BAT uptake and cardiac uptake in the 9-mo study because if the effects were due to diazepam alone, one might expect increased cardiac uptake. Note also that the 9-mo study was performed at the end of winter.
Our current study found a statistically significant reduction in the presence of BAT uptake from 34% with warming alone to 16% with warming plus diazepam (P = 0.012), highlighting both the limitations of warming alone and the marginal benefit of diazepam in children. Interestingly, our study demonstrated a lower than expected incidence of BAT uptake in control groups and in females, whereas the literature generally suggests an increased incidence of BAT uptake in children (3,7,8) and females (2,7,9). However, our study found almost twice the rate of BAT uptake in males as in females—a finding that likely reflects the confounding influence of standard care. The control population was warmed. It is likely that female patients are more responsive to warming than male patients, because in the warmed blanket–only group, the highest proportion of BAT uptake occurred in spring for females and in winter for males. This possibility is also reflected by the greater response of females than males to use of diazepam to reduce BAT uptake.
CONCLUSION
BAT uptake is a common confounder on 18F-FDG PET imaging. Although warming the patient reduces the frequency of BAT uptake, the addition of diazepam has a significant impact on reducing BAT uptake in young patients, particularly female patients. Both warming and diazepam may confound interpretation of cardiac 18F-FDG studies.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 9, 2017.
REFERENCES
- Received for publication November 17, 2016.
- Accepted for publication January 31, 2017.





{kind=link}
{kind=link}
{kind=link}