


Abstract
The purpose of this study was to determine the clinical accuracy of 82Rb PET/CT myocardial perfusion imaging (MPI) when performed with regadenoson stress in a U.S. Department of Veterans Affairs (VA) population of patients. Methods: The initial cohort of 480 patients undergoing vasodilator PET MPI with regadenoson stress at our institution from September 2009 through July 2010 was closely tracked for short-term outcomes based on correlation with invasive coronary catheterization. Long-term outcomes were determined by major adverse cardiac event rates based on data extraction from the electronic medical record and grouped by summed stress score (SSS) for a 3-y period. Results: At the 3-y follow-up, there had been 31 patient deaths, 5 of which were heart-related. Twenty-four patients had documented myocardial infarctions. Event rates and cardiac death rates were highly predicted by the results of PET MPI. Seventy patients underwent invasive cardiac catheterization within 60 d of the PET MPI. Patients were increasingly likely to undergo catheterization as their SSS increased. Catheterization correlation demonstrated a sensitivity of 95%, a positive predictive value of 88.4% for significant coronary artery disease, and an overall accuracy of 86% for PET MPI with regadenoson stress when compared with invasive catheterization. Conclusion: PET MPI with regadenoson stress demonstrates high accuracy when correlated with invasive catheterization and clinical outcomes. The SSS was highly predictive of cardiac events and patient survival in a VA population over a 3-y period of clinical follow-up.
Myocardial perfusion imaging (MPI) with SPECT and PET has earned a strong reputation for providing accurate clinical information to guide decision making for patients with known or suspected coronary artery disease (CAD). Its use continues to be endorsed by practice guidelines and refined by published appropriate use criteria (1–3). The clinical superiority of myocardial perfusion PET has also been recently recognized in a joint statement by the American Society of Nuclear Cardiology and the Society of Nuclear Medicine and Molecular Imaging to encourage its continued appropriate use (4). PET MPI has been increasingly used in recent years as the availability of a generator-produced radiotracer (82Rb) and the proliferation of hybrid PET/CT cameras has brought the technically superior PET modality within the realm of the wider clinical community lacking direct access to a cyclotron. These developments have also coincided with the availability of regadenoson, a new Food and Drug Administration–approved cardioselective vasodilator. Regadenoson stress has been found accurate when used with SPECT MPI, for which it produces results comparable to adenosine stress (5). However, questions have persisted about its accuracy for PET MPI because of its quick onset, short duration of action, and low degree of vasodilation compared with other vasodilators historically used for cardiac PET protocols (6). Although regadenoson is approved by the Food and Drug Administration for SPECT MPI applications, its use for PET MPI would technically be considered off-label. Early reports from single-center sites involving small numbers of patients have found that for PET MPI, pharmacologic stress with regadenoson is comparable to that with dipyridamole in regard to image quality and the size and severity of any stress-induced abnormality (7). Other investigators have performed similar quantitative comparisons of the two stressors, including the use of coronary flow reserve analysis, and found they were not significantly different with respect to the measurement of absolute myocardial blood flow and myocardial flow reserve (8). More recently, the accuracy of the modality—emphasizing the importance of systolic reserve—has also been reported (9). The purpose of the current paper is to report on the clinical outcomes of the initial cohort of 480 patients undergoing PET MPI with regadenoson stress at our institution. To our knowledge, this is the first study to document clinical outcomes for 36 mo after the reference regadenoson PET MPI study.
MATERIALS AND METHODS
All patients who underwent clinically indicated PET MPI from January 2009 through July 2010 were included in an institutional review board–approved retrospective database, and their clinical outcomes were carefully tracked. Short-term outcomes were based on correlation with invasive cardiac catheterization when performed within 60 d of the noninvasive study. Long-term outcomes were reported as major adverse cardiac events occurring after the date the patient was enrolled in the study, determined by extraction of the code for myocardial infarction (International Classification of Diseases, Ninth Revision) from the patient history. The outcomes of 3 subpopulations were evaluated and reported separately: patients unable to augment left ventricular ejection fraction from rest to stress, patients with an ischemic electrocardiogram response to regadenoson stress, and female patients. The study was approved by the Institutional Review Board, and the need for informed consent was waived.
Regadenoson PET Imaging Protocol
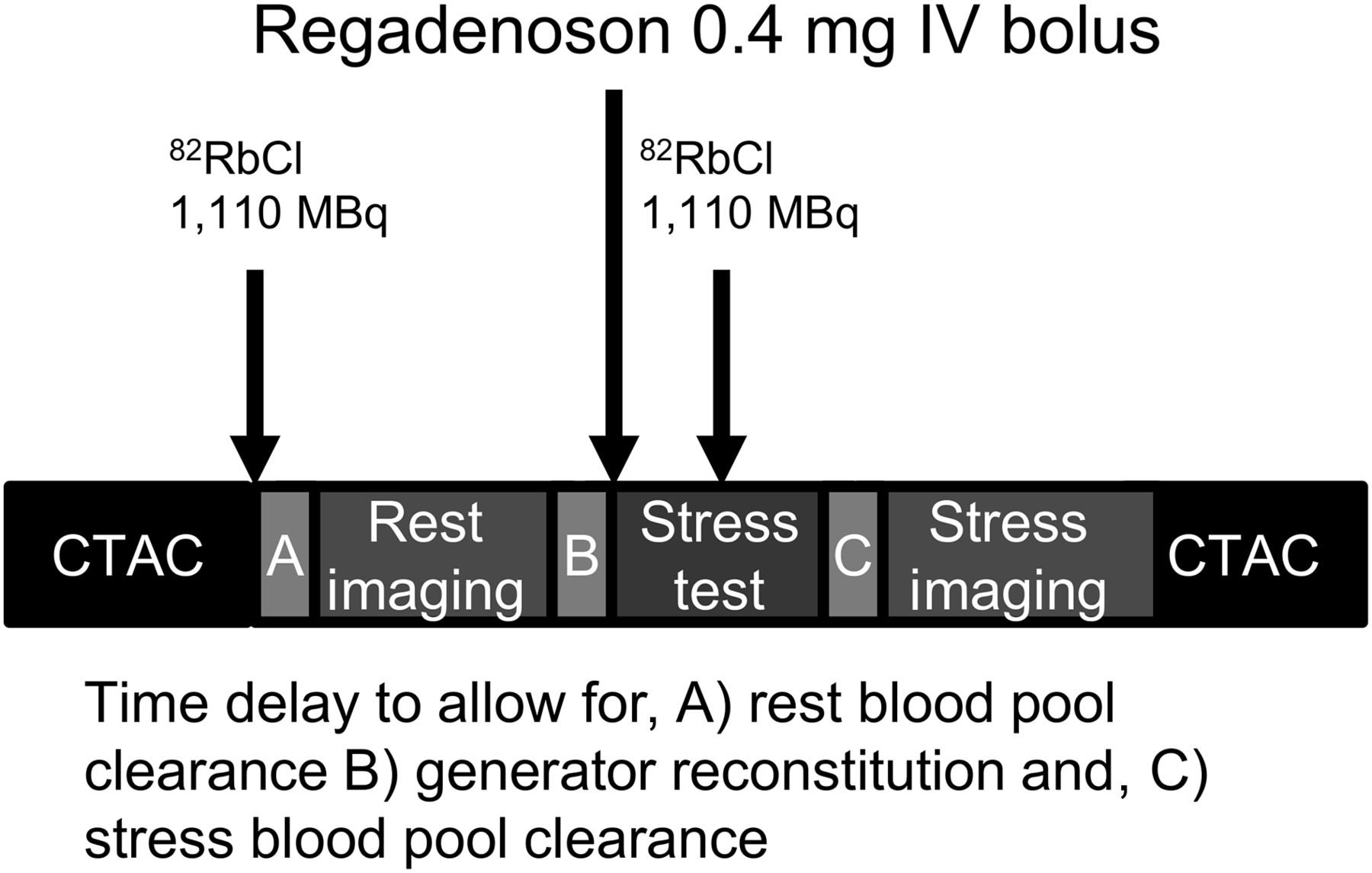
All subjects were imaged with a Gemini time-of-flight PET/CT scanner (Philips Medical) in 3-dimensional mode before and after induction of pharmacologic stress using a rapid intravenous bolus of regadenoson, 0.4 mg, followed immediately by a 10-mL saline flush and stress tracer administration. Rest and stress imaging were both performed with 1,110 MBq (30 mCi) of 82Rb Cl (1,480 MBq [40 mCi] if patient weight > 136 kg [300 lb]), and low-dose CT for attenuation correction was performed at rest and stress. The imaging protocol is illustrated in Figure 1. The patients were continuously monitored throughout the procedure for heart rate, blood pressure, and electrocardiogram changes until recovery and completion of stress imaging. Data were acquired from the initial time of injection in list mode, and perfusion data were processed after a 60- to 90-s delay, as appropriate, to allow for clearance of blood-pool activity.
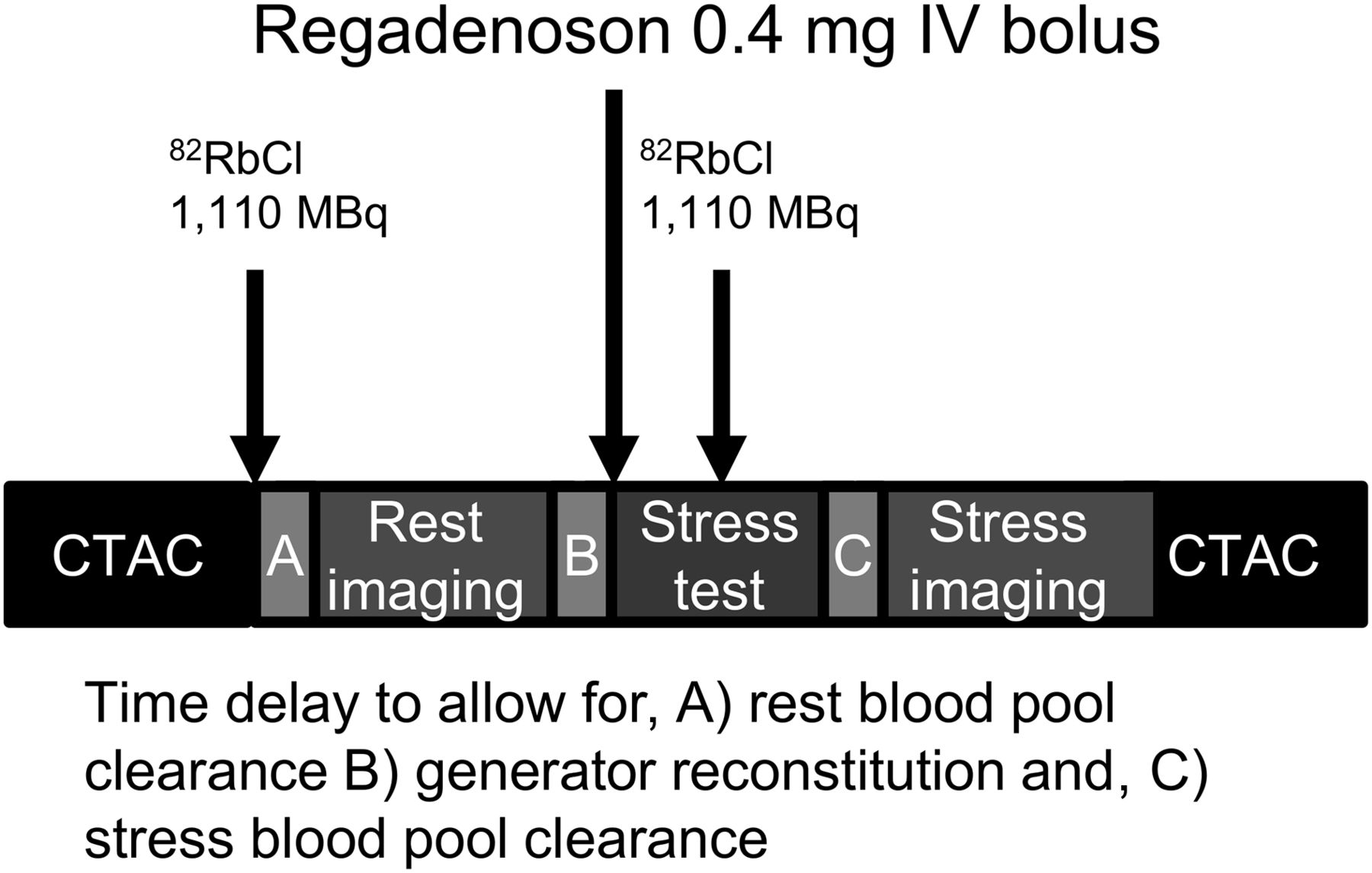
Rest–stress 82Rb PET/CT protocol. CT attenuation correction imaging (120 kVp, 10 mA, 0.704 pitch) was performed slowly over 1 min to simulate volume-averaged emission data from 7-min rest and stress perfusion data. Pharmacologic stress was induced by 0.4 mg of regadenoson followed by 10-mL saline flush and then immediately by second 1,110-MBq (30 mCi) infusion of rubidium. A final CT attenuation correction to apply to stress emission data concludes the protocol, which can be completed in approximately 30 min. CTAC = attenuation correction CT; IV = intravenous.
Image Processing and Reconstruction
Perfusion images were iteratively processed (maximum-likelihood expectation maximization, Butterworth 0.6, cutoff 10, 12 iterations) on an Extended Brilliance Workspace workstation (Philips Healthcare) and exported to a separate workstation for semiquantitative review using the Emory Cardiac Toolbox (version 3.0). Emission and transmission images were manually aligned by the technologist staff, and the interpreting physician confirmed the alignment by viewing fused images in the axial, coronal, and sagittal planes for both rest and stress datasets. Misregistration was corrected by manually shifting the fused datasets, with special attention to excluding cardiac activity from the lung field to avoid artifacts. Attenuation correction CT images were carefully reviewed for any clinically relevant incidental findings. Non–attenuation correction images were also carefully inspected for concordance with the attenuation correction imaging findings. Any discrepancies were again scrutinized for correct alignment of the transmission and emission datasets.
Interpretation of Perfusion and Gated Images
Perfusion images were independently interpreted by 4 experienced observers board-certified in nuclear medicine, who used a standard 17-segment cardiac model without knowledge of the catheterization results. The images were semiquantitatively analyzed using a 5-point scoring system (0 = normal, 1 = equivocal reduction of counts, 2 = mild reduction of counts, 3 = moderate reduction of counts, and 4 = absence of counts or background equivalence). Studies were evaluated for transient dilation based on concordance of the visual qualitative assessment and a quantitative threshold of greater than 1.19 as indicative of clinically significant transient dilation and possible critical or multivessel CAD. A summed stress score (SSS) of less than 4 was considered normal; 4–8 was considered mildly abnormal; 9–13, moderately abnormal, and more than 13, severely abnormal. Eight-frame gating was performed for assessment of global and regional systolic function. Image review and semiquantitative analysis were performed with the Emory Cardiac Toolbox (version 3.0).
Coronary Angiography
Cineangiograms were obtained in multiple projections using an Integris FD20 angiographic system (Philips Healthcare). Coronary cine angiograms were considered positive for significant CAD if the visually determined stenosis of the left main coronary artery was more than 50% or if the left anterior descending, circumflex, or right coronary arteries or their major branches had more than 70% stenosis.
Demographics
This study includes 480 patients presenting for a clinically indicated cardiac PET examination between January 2009 through July 2010. Ninety-seven percent were male, the average age was 61 y, and 38.9% had an established diagnosis of CAD at the time of the cardiac PET examination. Most patients were evaluated for chest pain, dyspnea, or atypical clinical symptoms suggestive of angina or an anginal equivalent. Additional patient characteristics are listed in Table 1.
Patient Characteristics (n = 480)
RESULTS
The patients generally tolerated regadenoson well. Use of the agent to induce pharmacologic stress was safe in this population. Minimal side effects were reported by 38% of patients. The most frequent side effects listed in the package insert are dyspnea, headache, flushing, and chest pain. Only 6 patients (1.2%) experienced side effects severe enough to require aminophylline reversal. The cardiac PET stress results, which were based on SSS, transient dilation, and systolic function evaluation, were normal (SSS < 4) in 223 patients (46.5%), mildly abnormal (SSS 4–8) in 134 (27.9%), moderately abnormal (SSS 9–13) in 55 (11.5%), and severely abnormal (SSS > 13, transient dilation, drop in left ventricular systolic function) in 68 (14.2%).
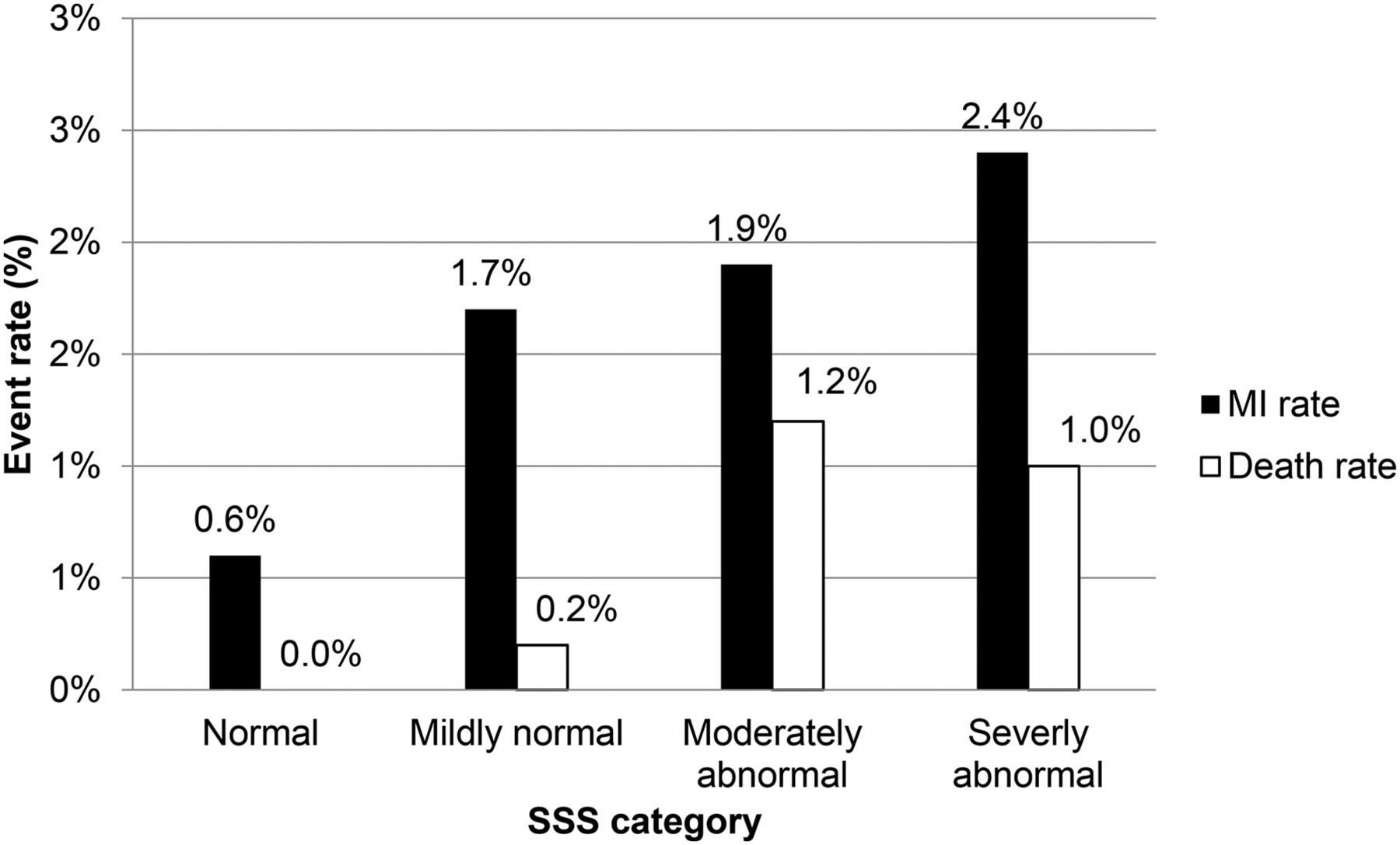
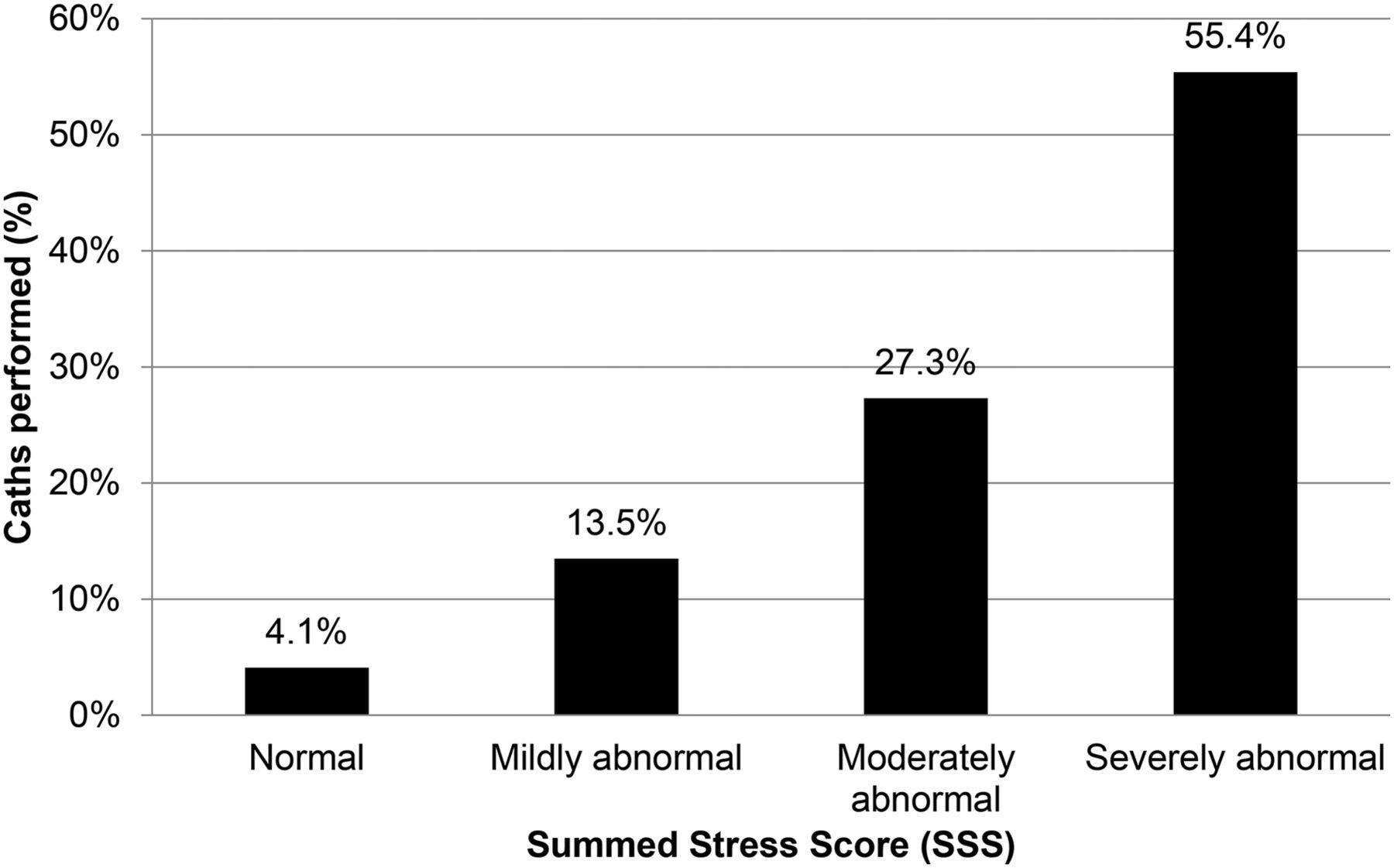
At the 3-y follow-up, there had been 31 deaths, 5 of which were heart-related. Myocardial infarction during the follow-up period had been documented for 24 patients. Event rates and cardiac death rates were highly predicted by the results of PET MPI (Fig. 2). Fifty patients without prior coronary artery bypass grafting underwent invasive cardiac catheterization within 60 d of the PET MPI. Patients were increasingly likely to undergo catheterization as their SSS increased (Fig. 3). Compared with invasive catheterization, PET MPI with regadenoson had a sensitivity of 95%, a positive predictive value of 88.4%, and an overall accuracy of 86% (true-positive + true-negative/true-positive + true-negative + false-positive + false-negative).
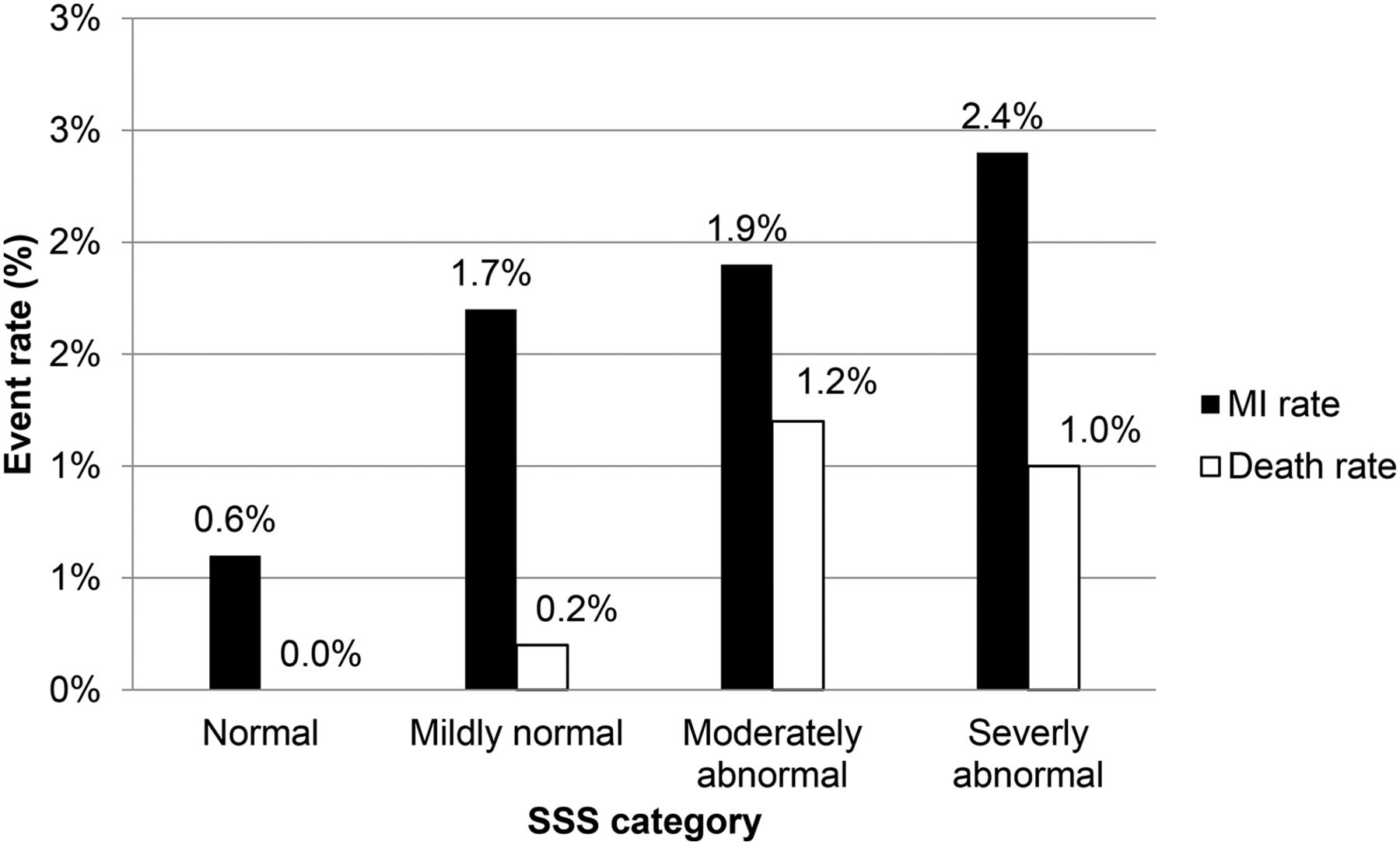
Myocardial infarction and death rates by SSS.
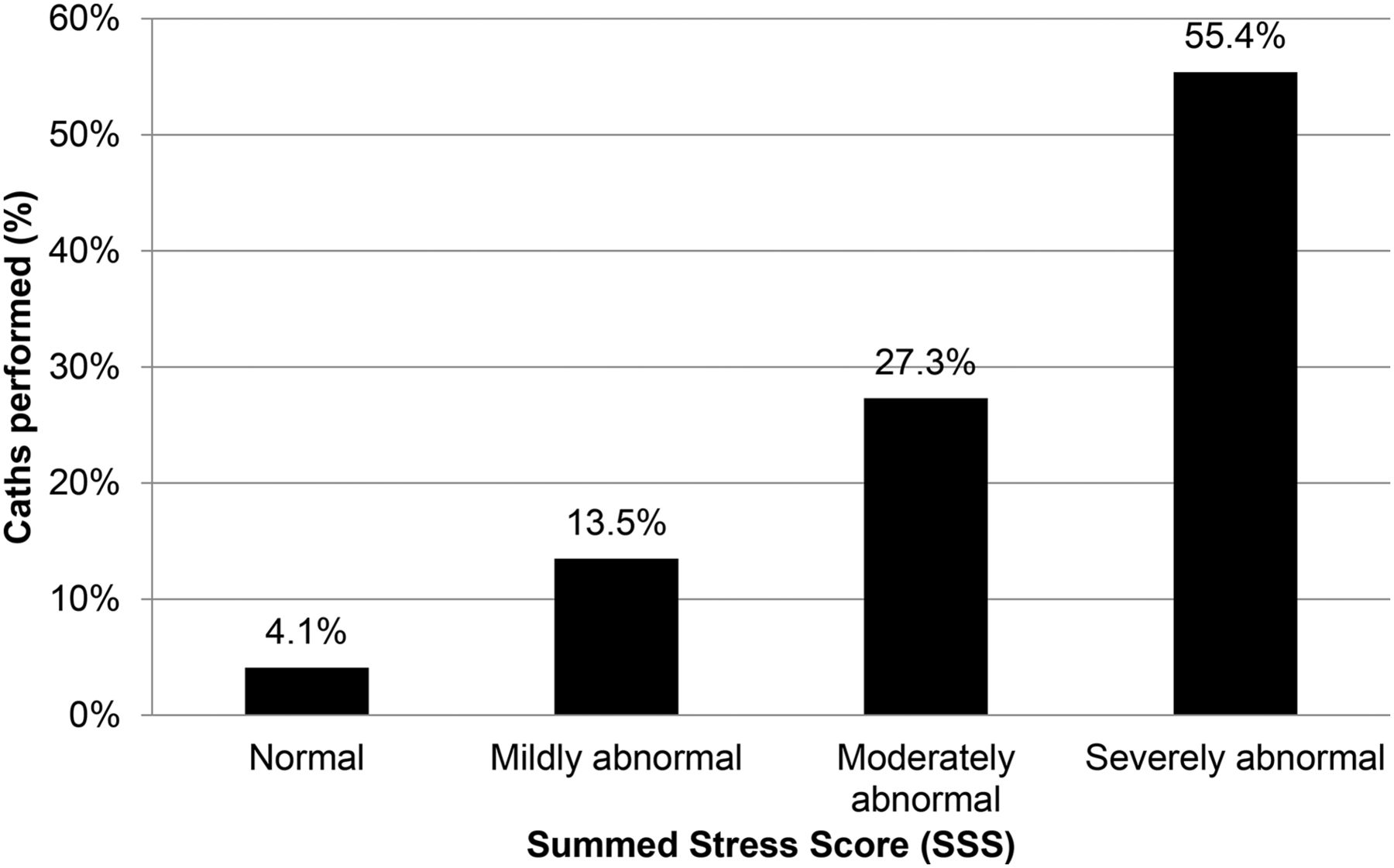
Rate of cardiac catheterization (Caths) increased as SSS increased.
Patients with Decreased Left Ventricular Ejection Fraction Reserve
Left ventricular ejection fraction reserve, the ability of the heart to increase its systolic function in response to stress, has been reported to be an important factor in predicting future events (9). In 65 patients (13.5%) who completed PET MPI with regadenoson stress, systolic function decreased after stress testing. The fall in ejection fraction ranged from 1% to 25% (mean, −5.5%). None of these patients experienced cardiac death during the 3-y follow-up. Six experienced myocardial infarction; none had a change of less than 2% in ejection fraction. The average fall in ejection fraction among patients with a documented hard event after stress testing was 9.5% (range of ejection fraction decrease, 2%–25%). Of the 65 patients with a fall in ejection fraction after stress testing, 5 concurrently manifested an ischemic electrocardiogram response (≥1 mm of ST depression) to vasodilator stress. Their SSS ranged from 0 to 36 (average, 9.4).
Patients with Abnormal Electrocardiogram Response
Ten patients (2.1%) had an ischemic electrocardiogram response (≥1 mm ST depression) to pharmacologic stress with regadenoson. Their average SSS was 12.5 (range, 0–29), and they were 2.7 times more likely to undergo invasive cardiac catheterization than patients without an ischemic response. Three patients with discordant electrocardiogram and imaging findings (abnormal electrocardiogram response to pharmacologic stress but SSS < 4) did not undergo invasive catheterization. No hard event had been documented during the follow-up period in any of these patients. All patients with an ischemic response concordant with imaging results underwent invasive cardiac catheterization and were found to have significant, multivessel CAD. Five (83%) of these 7 patients underwent revascularization (3 with coronary artery bypass grafting and 2 with percutaneous coronary intervention), and one—despite having multivessel CAD—did not undergo revascularization during the follow-up period because there was a comorbidity, pancreatic carcinoma, from which the patient died.
Female Patients
Fourteen patients (2.9%) were female. The PET MPI results were normal in all except one, who had a mildly abnormal result with an SSS of 8, indicating inferior ischemia. This patient was treated medically and had a good clinical outcome, with no hard event documented during the follow-up period. No female patient underwent cardiac catheterization, experienced myocardial infarction or cardiac death during the 3 y after testing, had an ischemic response to vasodilator stress, or developed stress-induced systolic dysfunction.
DISCUSSION
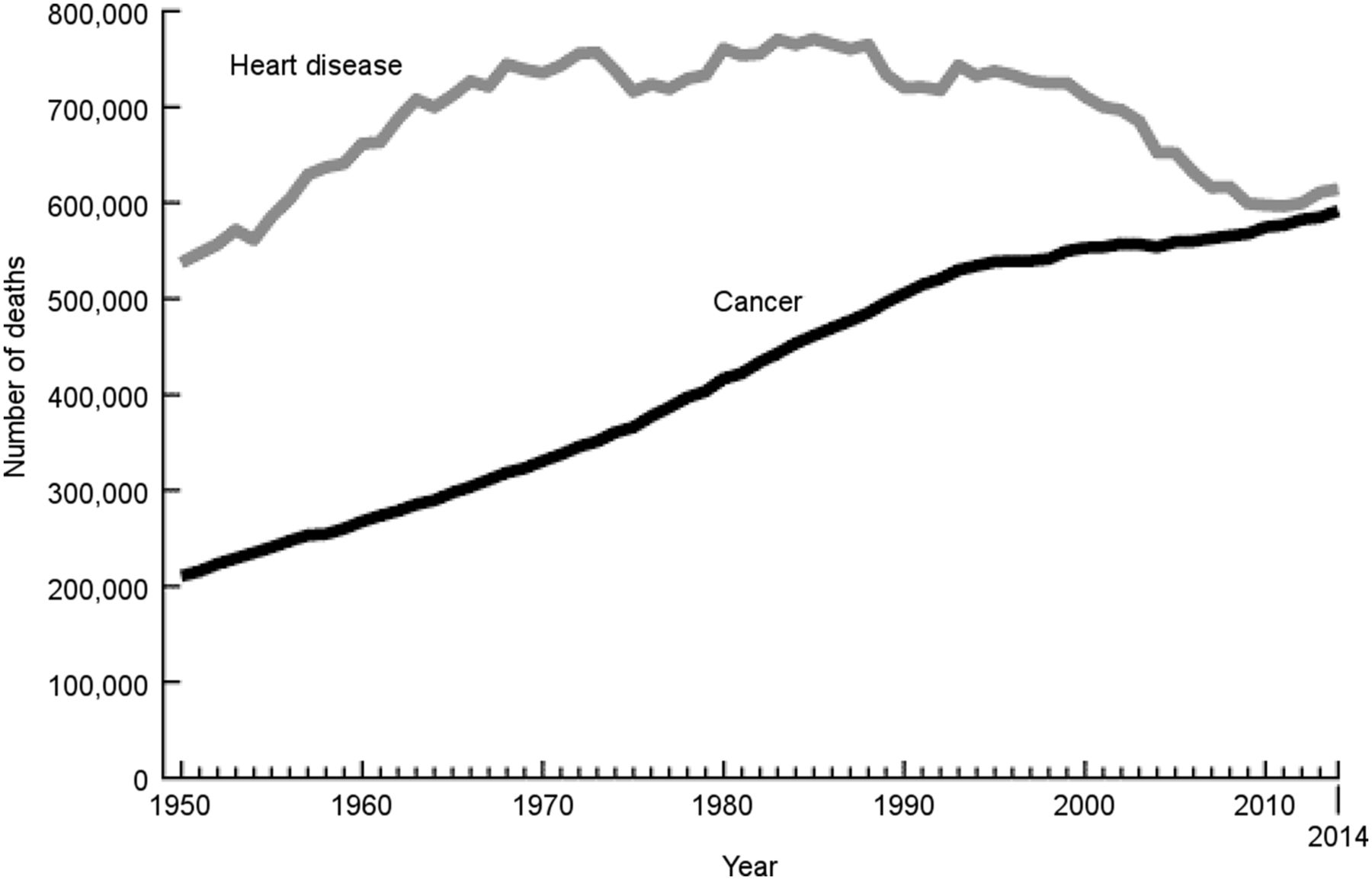
CAD continues to be the leading killer of Americans, both men and women. The Centers for Disease Control and Prevention reported that recent changes in mortality trends related to heart disease and cancer suggest that cancer is poised to become the leading cause of death in the United States in this decade if those trends are sustained (Fig. 4). In several states, this is already the case (10). The noninvasive assessment of CAD has relied heavily on gated SPECT MPI in the past because of its powerful ability to risk-stratify patients, predict prognosis, and direct patient management decisions to allocate health-care resources appropriately while improving patient outcomes. In recent years, use of cardiac PET/CT has led to an even better sensitivity and specificity as a result of its greater spatial resolution, inherent high quality, attenuation correction, and flow quantification.
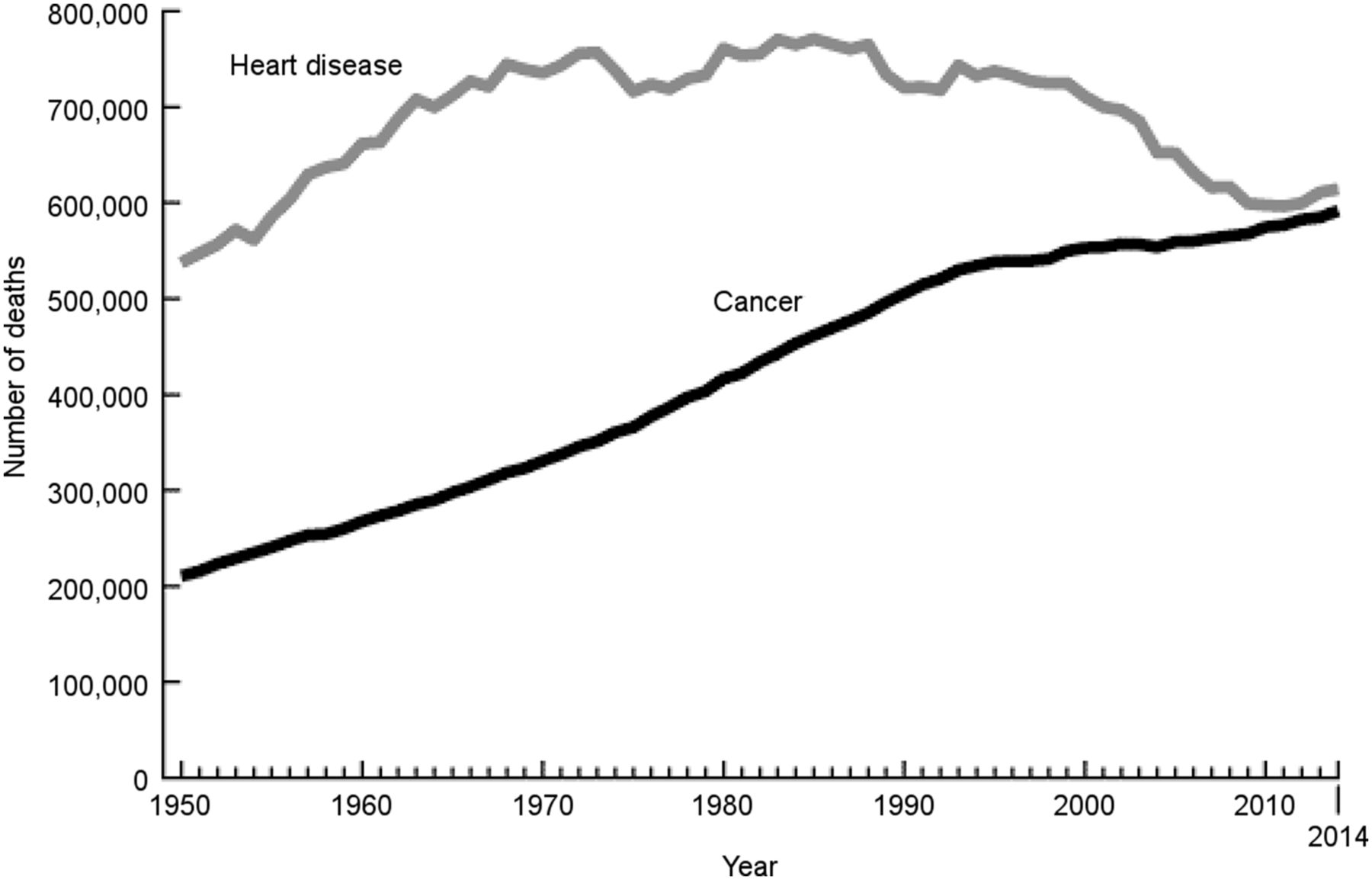
U.S. mortality trends for heart disease and cancer (10). Leading cause is based on number of deaths.
Compared with conventional SPECT MPI, PET/CT MPI offers technically superior, CT attenuation–corrected images for clinically challenging patients with known or suspected CAD. For patients unable to achieve adequate treadmill exercise or requiring pharmacologic stress for other reasons (such as a left bundle branch block), and who do not have severe, limiting claustrophobia, PET MPI offers a superior clinical protocol that can be completed in about 30 min. A recent joint statement by the American Society of Nuclear Cardiology and the Society of Nuclear Medicine and Molecular Imaging recognized the superiority of cardiac PET for these patients (4). This option also greatly improves the clinical efficiency of the department and lessens the patient’s time commitment compared with a standard 3-h conventional pharmacologic SPECT MPI protocol.
Regadenoson is more efficient than the other commercially available vasodilators, dipyridamole and adenosine, because it has fixed dosing (0.4 mg for all patients) and a simple intravenous bolus administration requiring no infusion system, but there has been concern about its lower and briefer maximal vasodilation. Previous reports have documented equivalent defect detectability and similar quantitative myocardial flow and flow reserve results between regadenoson and the other vasodilators, but to our knowledge, ours is the first report that extends follow-up on major adverse cardiac events to 3 y after the reference regadenoson PET MPI study.
The temporal efficiency of vasodilator PET MPI also allows global systolic function and regional wall motion to be assessed more contemporaneously with myocardial perfusion, increasing the ability to detect myocardial stunning in response to pharmacologic stress. Other authors have proposed that a poor prognosis may be predicted by failure of the stress ejection fraction to augment by at least 1% compared with rest (9). Although the threshold for changes in rest and stress ejection fraction may be debatable, the temporal proximity of wall motion assessment to stress testing should increase sensitivity for detection of this ischemic manifestation of CAD.
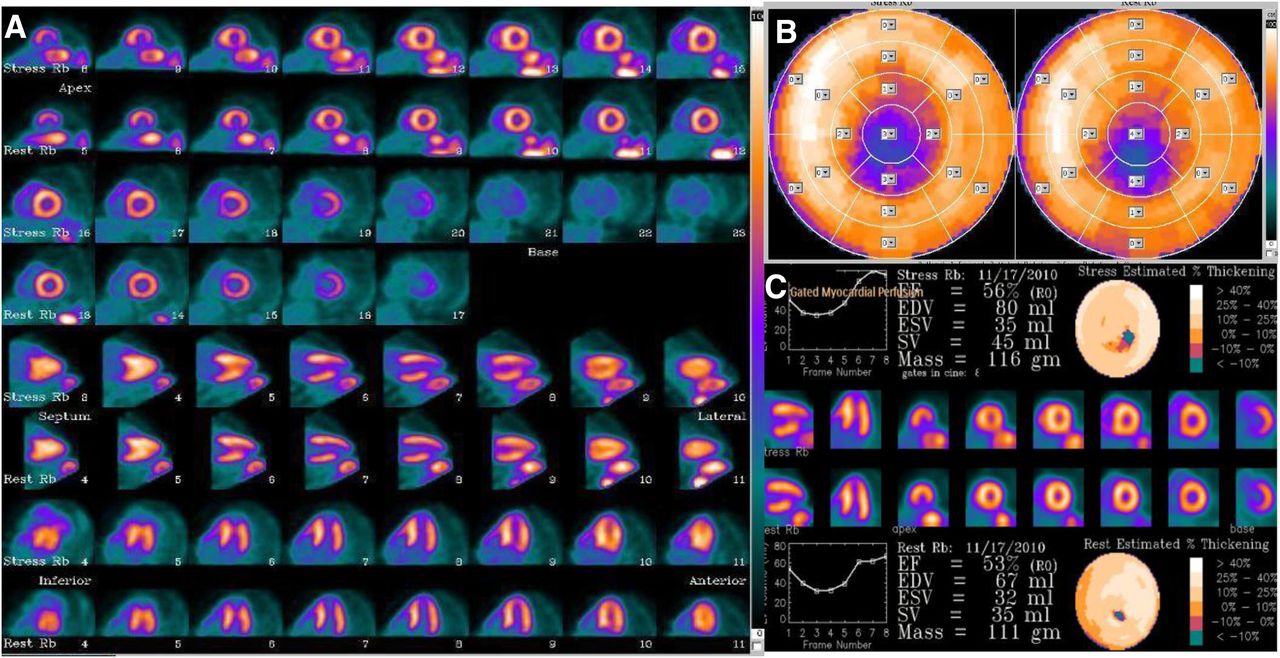
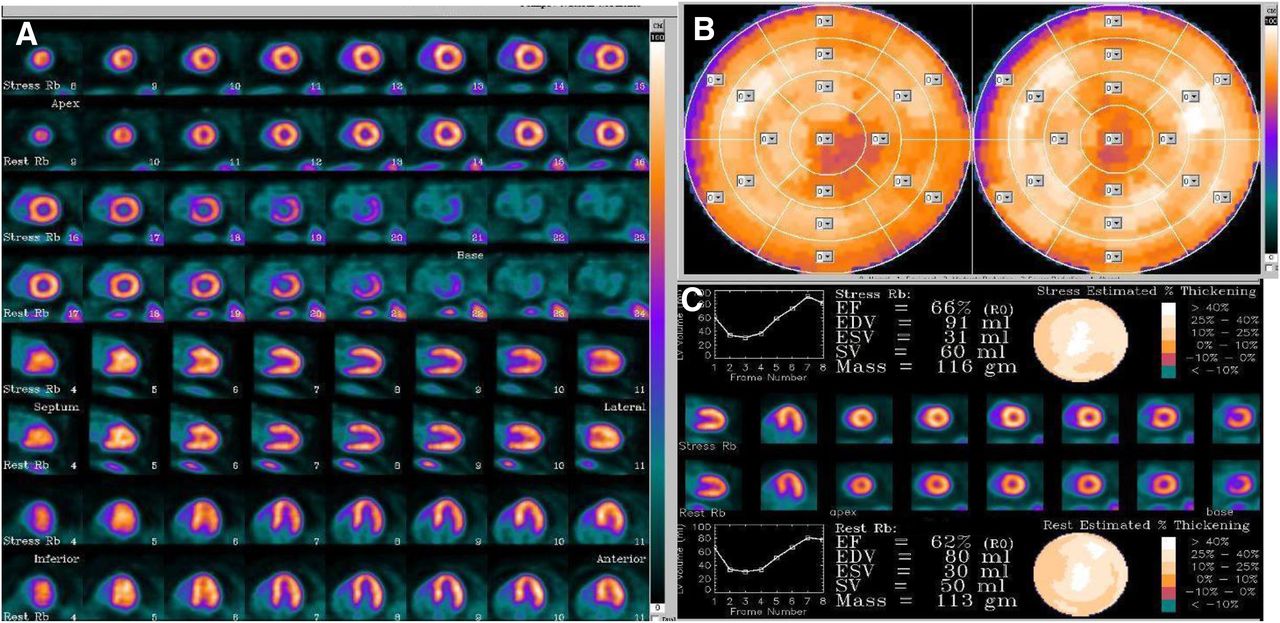
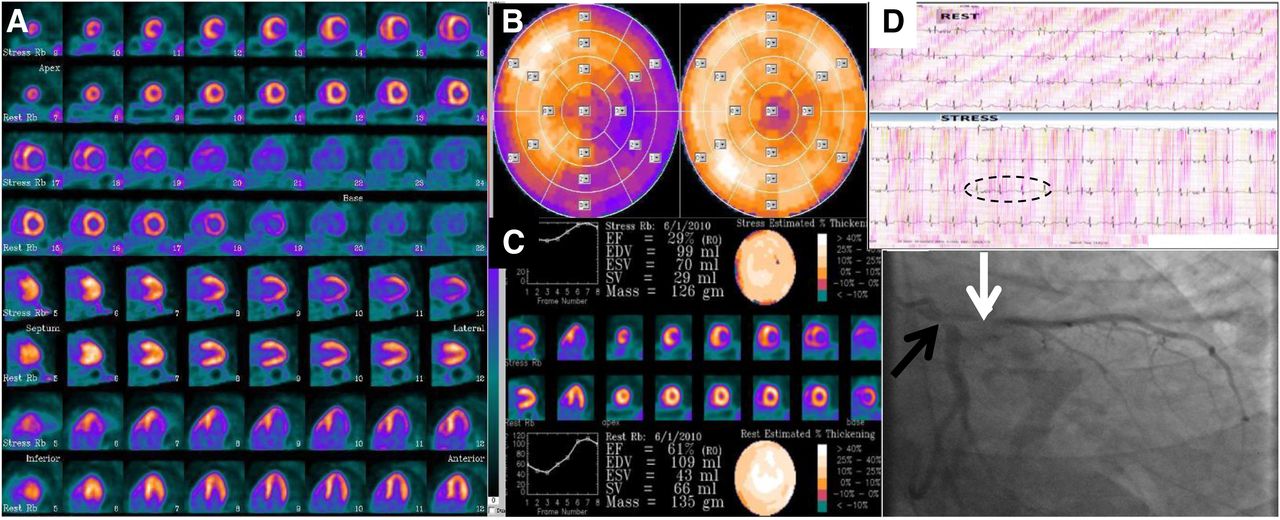
PET MPI performed well in our cohort of patients. The spectrum of findings in patients with known or suspected CAD can range from normal to severely abnormal. Figure 5 shows a representative patient with normal myocardial perfusion and function at stress and rest, denoting a low risk of myocardial infarction or cardiac death, and Figure 6 shows a representative patient with single-vessel disease involving the inferior wall. PET/CT is particularly helpful in the latter situation because of the likelihood of interference from diaphragmatic attenuation artifacts, especially in the large male patients commonly seen in our U.S. Department of Veterans Affairs (VA) population. Such a patient can be treated with maximal medical therapy, whereas revascularization would be reserved for refractory symptoms. Finally, Figure 7 shows a representative patient with extremely high-risk features: the triad of multiple-vascular-territory ischemia, transient dilation, and hemodynamic instability identified from rest and stress gating, coupled with acute electrocardiogram changes after vasodilator stress. This constellation of findings predicts that surgical revascularization will likely be the best option. Subsequent cardiac catheterization in this patient demonstrated critical disease of the proximal circumflex coronary artery and moderate disease of the left anterior descending coronary artery. Unfortunately, the patient had a comorbid malignancy that precluded revascularization, and he died of noncardiac causes 6 mo after the examination.
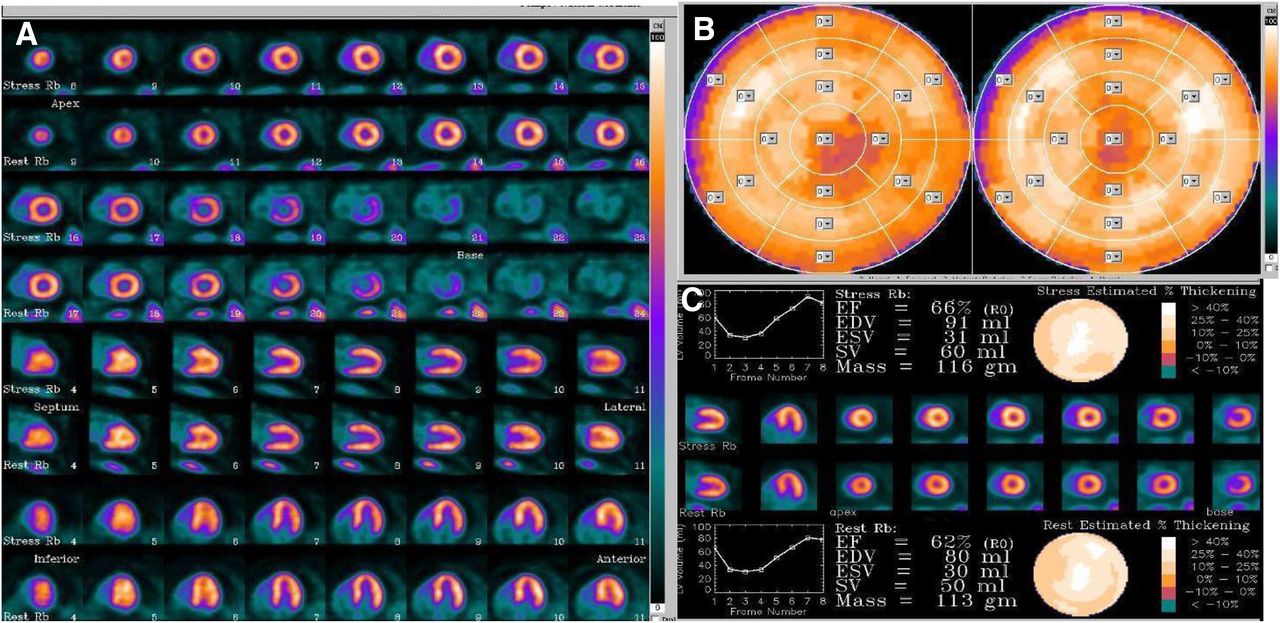
A 56-y-old man with history of diabetes mellitus, hypertension, and morbid obesity with complaints of exertional dyspnea and atypical chest pain. Normal findings were seen on 82Rb PET MPI at stress and rest (A), semiquantitative bull’s-eye images (B), and gated images (C). Presence of normal regional myocardial perfusion and left ventricular systolic function showed this patient to be at low risk for myocardial infarction or cardiac death. Patient has done well in the 36 mo since examination, with no heart-related events.
A 50-y-old man with history of chronic chest pain, risk factors for CAD, and abnormal baseline electrocardiogram results. (A) PET MPI showed severe, nonreversible perfusion defect in distal inferior wall and apex consistent with old myocardial infarction. (B and C) Semiquantitative bull’s-eye (B) and gated (C) images confirmed fixed defect and associated regional wall motion abnormality.

A 59-y-old man with known CAD and complaints of exertional arm and jaw pain after percutaneous coronary intervention of left anterior descending coronary artery. (A) 82Rb PET MPI showed large territory of severe inferolateral ischemia in expected circumflex distribution. (B) Semiquantitative bull’s-eye images showed that SSS was 15. (C) Gated images revealed normal left ventricular ejection fraction of 61% at rest, which fell to 29% under stress. Transient dilatation (1.3; normal, <1.19) was also present. Patient developed 1.5-mm ST depression in inferior leads II, III, and AVF (circled) during pharmacologic stress, which resolved after intravenous administration of aminophylline. (D) Subsequent left heart catheterization showed 60% stenosis of proximal left anterior descending coronary artery (white arrow) and 99% stenosis of proximal circumflex coronary artery (black arrow), confirming the 82Rb PET findings. Because of comorbid disease, patient was not a candidate for surgery, and he died of noncardiac causes 6 mo after examination.
Although conventional SPECT cameras are more available than PET/CT scanners in the community-hospital setting, availability of the hybrid devices is growing. PET/CT is being increasingly used to assess and risk-stratify patients with known or suspected CAD. Cardiac PET/CT, with its more efficient imaging protocols, results in higher-quality clinical results, lower exposure of patients to radiation, and a significantly shorter procedure. The attenuation correction inherent in all cardiac PET imaging makes it better suited for patients prone to attenuation artifacts. Although PET/CT requires a large capital investment and operational footprint, studies have shown that the decreased downstream costs stemming from its increased accuracy make the modality more than cost-effective (11). In particular, if a busy clinical environment such as the VA health-care system already deploys a PET/CT scanner for oncology imaging, applying it for cardiac imaging as well can maximize its use, benefit patient care, and improve workflow and efficiency. The availability of a generator-produced myocardial perfusion tracer, although costly, obviates a cyclotron. If a facility has access to a cyclotron, other agents (e.g., 13N) may be more cost-effective.
Although our results are limited by the retrospective, single-center design of the study, it was reassuring to find that—over both the short term and the long term—regadenoson PET MPI was highly predictive of obstructive CAD and subsequent cardiac events. This finding, viewed in context with other recent series documenting similar lesion detectability and absolute flow quantification, supports the continued clinical use of regadenoson stress for PET MPI. The sensitivity and specificity of PET MPI studies can be increased by adding software tools that provide absolute quantification of myocardial blood flow and coronary flow reserve. Validated software was available only for 13NH3 when our initial patient cohort was studied, and hardware limitations at our center also precluded its use. Computer modeling is now available for 82Rb and needs to be validated for use of regadenoson, rather than dipyridamole, as the vasodilator. The addition of this assessment would further strengthen the ability of PET to identify CAD patients at risk for adverse events.
The population of our study was almost exclusively male, as reflected by the demographics of patients served by the VA health-care system. The number of women being cared for at VA hospitals is increasing, but women were underrepresented in our study cohort. PET MPI performed well in our limited number of women; the rate of normal findings successfully predicted a low rate of cardiac events. Continued verification of the modality’s accuracy in women is important.
Interesting areas of future research include evaluating the quantitation of regadenoson 82Rb PET MPI with regard to coronary flow reserve. In addition, the conventional SPECT-derived breakpoints for SSS—transient dilation and change in ejection fraction—bear reexamination in the PET era, and it is also important to establish the ability of regadenoson PET MPI to detect and risk-stratify female patients for CAD. These investigations will require larger patient populations and are currently under way at our facility.
CONCLUSION
PET MPI with regadenoson stress demonstrated high sensitivity, high positive and negative predictive values, and high overall accuracy when compared with invasive catheterization. The SSS was highly predictive of cardiac events and survival in the initial cohort of 480 patients undergoing the procedure at our facility. The combination of a reversible perfusion abnormality and an ischemic electrocardiogram response to regadenoson stress was highly predictive of severe CAD and the need for subsequent revascularization. The results of regadenoson stress were accurate and clinically relevant and were not inferior to those of conventional SPECT MPI at our facility, based on comparisons with historic active catheterization correlations, which have been documented since 2008.
DISCLOSURE
This work was supported by the Dallas VA Research Corporation and used the resources and facilities of the Dallas VA Medical Center, which is a part of the VA North Texas Health Care System. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank all the patients who contributed to this study; Edwin Tajalle and Stephen Faith, the CNMTs who cared for them while performing the examination; and Monique Shuler, who provided excellent technical, data analysis, and statistical support.
Footnotes
Published online Apr. 13, 2017.
REFERENCES
- Received for publication December 28, 2016.
- Accepted for publication March 6, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}