


Abstract
The Society of Nuclear Medicine (SNM) published procedure guidelines for thyroid imaging in 1999. We wished to determine how many clinics performing thyroid imaging follow the guidelines and to what extent. Of particular interest to us was the choice of collimator. Methods: We developed a 10-question survey to obtain information on how hospitals perform thyroid imaging. The questions were designed to cover the procedure recommendations of the SNM guidelines. The survey was sent to 350 hospitals randomly selected from 11 states in the northeastern United States. Results: One hundred sixty-five surveys (47%) were returned. Most of the clinics that responded obtain a history, hyperextend the neck, and obtain anterior and anterior oblique views. Twenty-five percent of the respondents obtain all their images with a parallel-hole collimator. Seventy-five percent use a pinhole collimator or a combination of parallel-hole and pinhole collimators. The number of counts and time used for acquiring the images vary greatly. Less than half the respondents palpate the neck for correlation with the scan. Conclusion: The survey results indicated that many clinics do not follow the recommendations of the SNM guidelines. The major deviations from the guidelines were in the choice of collimator, the number of counts or amount of time used to acquire images, and the lack of neck palpation for correlation with the scan.
The thyroid gland is located in the neck, superior to the trachea and between the thyroid cartilage and sternal notch. The gland is relatively small, consisting of 2 lobes, each of which is approximately 2–3 cm wide by 5 cm high. The 2 lobes are connected in the middle by the isthmus. The primary function of the thyroid gland is to synthesize, store, and secrete the thyroid hormones thyroxine and triiodothyronine. These hormones stimulate many metabolic processes, which are reflected by increased oxygen consumption and heat production. The synthesis and secretion of thyroid hormones is maintained by a feedback mechanism. Thyroid-stimulating hormone is secreted by the pituitary gland and is regulated by the thyroid-releasing hormone produced in the hypothalamus. Thyroid-releasing hormone acts on the pituitary to release thyroid-stimulating hormone, which acts on the thyroid to increase all aspects of thyroid function. When the level of triiodothyronine and thyroxine in the blood rises, the level of thyroid-stimulating hormone falls because the hypothalamus produces less thyroid-releasing hormone, thus maintaining optimal thyroid function (1). Common thyroid disorders or problems include hyperthyroidism, hypothyroidism, inflammation of the thyroid, and thyroid cancer. Nuclear medicine plays a major role in the diagnosis and treatment of these conditions. Common indications for thyroid imaging include the evaluation of palpable nodules, evaluation of a gland abnormal to palpation but without nodules, evaluation of patients who had irradiation of the head and neck in childhood with or without palpable nodules, evaluation for ectopic thyroid tissue and lingual thyroid, and evaluation of congenital hypothyroidism.
The Society of Nuclear Medicine (SNM) published procedure guidelines for thyroid imaging in 1999 (2). The radiopharmaceuticals and doses for thyroid imaging recommended in the guidelines are listed in Table 1. The guidelines recommend that the patient be supine and that the neck be extended by placement of a pillow under the shoulders. No fasting is required. A patient history should be taken and should include the results of thyroid function tests, the results of prior thyroid uptake and imaging tests, and mention of whether the patient had recently been administered radionuclides, had recently ingested iodine-rich foods, had undergone any prior iodinated-contrast procedures, might be taking interfering medications, or is pregnant or lactating.
SNM Guidelines for Thyroid Imaging Radiopharmaceutical and Dose
The guidelines recommend that when 99mTc is used, the anterior image be acquired for 100,000–200,000 counts or for 5 min. When 123I is used, the guidelines recommend anterior imaging for 50,000–100,000 counts or 10 min. The thyroid should be palpated with the patient positioned for imaging. The views should include anterior and right and left anterior oblique. Radioactive markers should be used to identify anatomic landmarks and the location of palpable nodules. Duplicate views should be obtained without markers. For measuring the thyroid gland, sizing markers are useful but should be applied with caution since the pinhole collimator will cause geometric distortion with depth.
The purpose of the guidelines is to assist nuclear medicine practitioners in recommending, performing, interpreting, and reporting the results of thyroid scintigraphy. Regarding interpretation of the scans, the guidelines suggest that localized findings on palpation should be marked on the neck of the patient so they can be correlated with the scintigraphic image. Information from ultrasound or other diagnostic imaging procedures should be available for comparison with the images obtained by radionuclide studies.
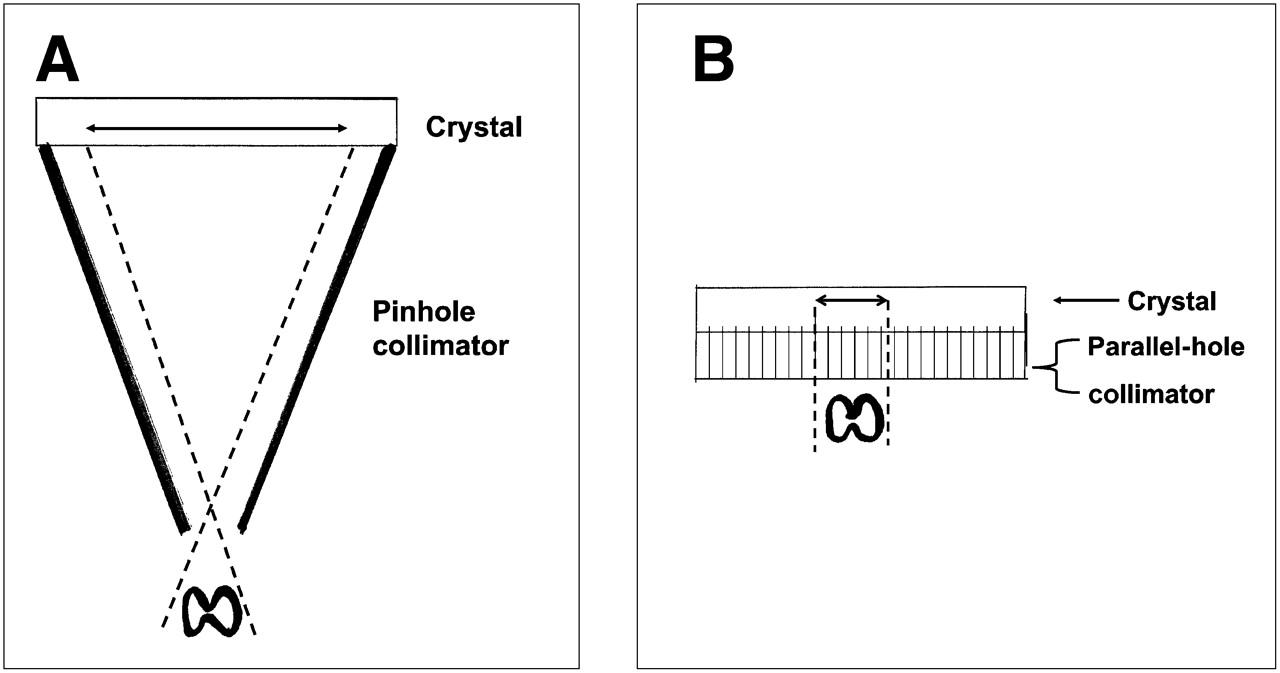
The SNM guidelines and most literature (2–4) recommend the pinhole collimator for routine thyroid imaging. Pinhole collimators, compared with parallel-hole collimators, offer improved spatial resolution for smaller organs such as the thyroid. The object is magnified and seen by a greater area of the detector, and the image is limited primarily by the intrinsic resolution of the γ-camera (Fig. 1). As the distance between the pinhole collimator and the source is increased, relative geometric efficiency drops rapidly (5). Therefore, a pinhole collimator can achieve superior system resolution and reasonable relative geometric efficiency at close distances (Fig. 2) (6). Thyroid imaging can be performed with a parallel-hole collimator, but the system resolution will not be as good as with a pinhole collimator at the same source-to-collimator distance. Zooming or magnifying parallel-hole images will not increase their resolution. As a result, small nodules in the thyroid may not be resolved (7).
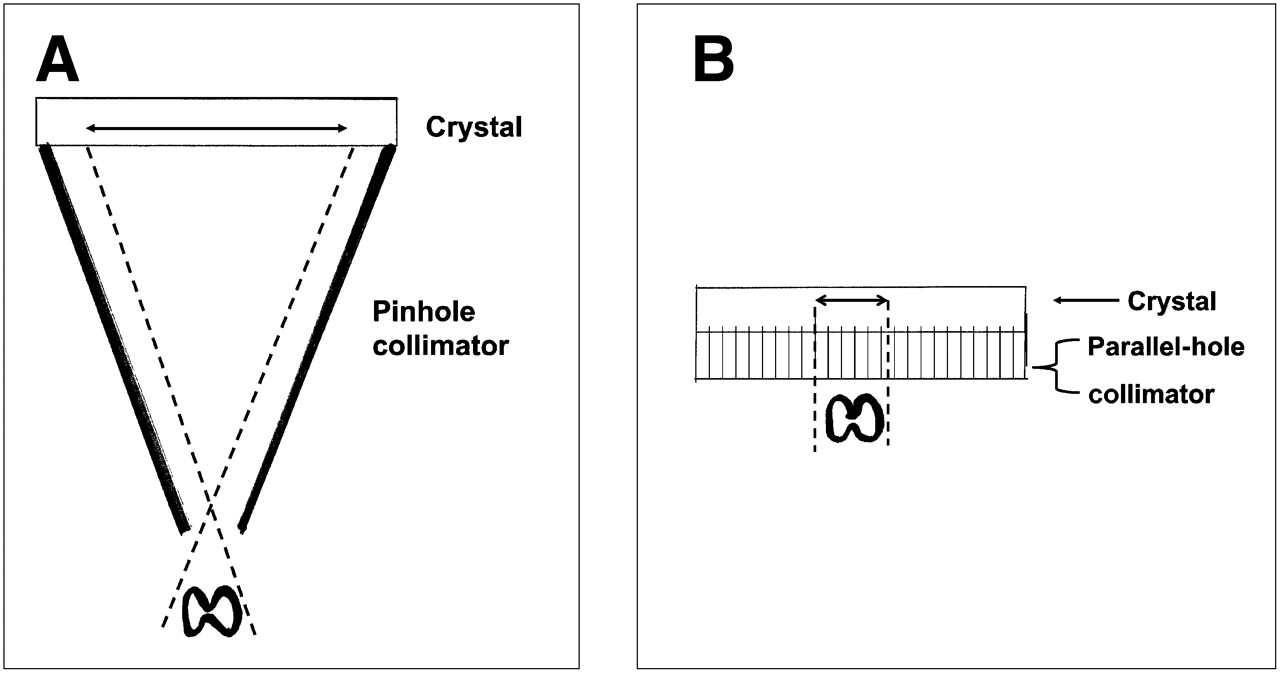
A larger area of the detector “sees” object when object is close to pinhole collimator (A) than when object is close to parallel-hole collimator (B).

Performance characteristics of various collimators (5).
Most clinics in western New York use a pinhole collimator for thyroid imaging. However, several use the parallel-hole collimator exclusively. This fact prompted us to conduct this study. The purpose of our study was to determine how many clinics perform thyroid imaging following the SNM guidelines and to what extent. Although inquiring about the choice of collimator was the main objective of the study, we designed a survey to inquire about other aspects of thyroid scintigraphy as well.
MATERIALS AND METHODS
A 10-question survey was designed to obtain information on thyroid imaging procedures. The questions were designed to cover the procedure recommendations of the SNM guidelines. The specific survey questions are listed in the Appendix.
The survey was sent to 350 hospitals with nuclear medicine departments, throughout the Northeast. The hospitals were randomly selected from the American Hospital Directory (www.ahd.com). The hospitals were located in 11 states, including New York, Pennsylvania, Michigan, Ohio, Connecticut, Vermont, Massachusetts, New Jersey, Virginia, North Carolina, and Maryland.
RESULTS
One hundred sixty-five surveys (47%) were returned from hospitals in 10 different states whose number of beds ranged from 35 to 501, with an average of approximately 200. The survey results are listed in Table 2.
Survey Results
Radionuclide
One hundred seventeen of the 165 surveys returned (70.9%) stated that 123I is used for thyroid imaging. Forty-one of the 165 (24.8%) use 99mTc-pertechnetate for routine imaging.
Dose
Most clinics (85/165, or 51.5%) performing thyroid imaging use a dose of between 200 and 299 μCi (1 Ci = 37 GBq) of 123I for thyroid imaging. The other 80 of 165 (48.5%) used doses ranging from 100 to 599 μCi per patient. The 41 responders that use 99mTc-pertechnetate for patient dosing use a range from 400 μCi to 20 mCi, with the majority predominately using a 10-mCi dose.
Neck Positioning
One hundred fifty-five, or 93.9%, of respondents stated they hyperextended the neck during thyroid imaging. The other 10 did not answer this question on the survey.
Fasting
Sixty-seven of the 165 (40.6%) reported having the patient fast before the examination. The number of hours of fasting ranged from 1 to 12 before patient dosing. Ninety-eight respondents (59.4%) do not require the patient to fast.
Patient History
Nearly all respondents (163/165, or 98.8%) reported taking a patient history. Two (1.2%) did not report that a patient history was taken.
Views
All respondents who answered the survey question on views reported taking an anterior view. The number of clinics that acquire oblique views was 151 of 165 (91.5%). There were 149 clinics that reported using right and left anterior oblique views without markers and 2 clinics that reported taking oblique views with markers. Most respondents reported taking 2 anterior views—one with and one without markers. Thirty-seven, or approximately 23%, reported taking only 1 anterior view with no markers. A smaller number (13, or 8%) reported acquiring only 1 anterior view with markers.
Counts Versus Time
One hundred seventeen, or 70.9%, of the clinics reported using 123I. Of those, 84 use only counts or time whereas 33 use both and end the acquisition by whichever is reached first. The counts that were reported ranged from 20,000 to more than 300,000. Time termination ranged from 5 to 20 min. Of the clinics who responded, 41 of 165, or 24.8%, reported using 99mTc-pertechnetate. Thirty of the 41 reported using only counts or time, whereas 10 reported using both counts and time. The reported counts ranged from 50,000 to more than 300,000, and the reported time ranged from 5 to 10 min.
Measurement
Only 72 of the 165 clinics reported using some type of method to size the gland. The reported methods include grid pictures, radioactive rulers, computer software, a 57Co marker, ultrasound, and lead markers. Ninety-three of 165, or 56.4%, reported not using a method to size the gland.
Collimator
Regarding the type of collimator used, 107 of 165 (64.8%) clinics reported using a pinhole collimator for imaging the thyroid, 42 of 165 (25.5%) reported using a parallel-hole collimator, and 16 of 165 (9.7%) use both pinhole and parallel-hole collimators.
Neck Palpation
Less than half the respondents, 67 of 165 (40.6%), palpate the neck for correlation with the scan. Ninety-eight (59.4%) reported that no palpation is performed.
DISCUSSION
Twenty-eight percent of the survey respondents use 99mTc-pertechnetate exclusively for thyroid imaging. The SNM guidelines list the advantages and disadvantages of 99mTc-pertechnetate and 123I-iodide for thyroid imaging (Table 3) (2). In addition to those items (Table 3), many publications have reported discordant results for thyroid nodules when imaged with these 2 different agents (8–11). Cold thyroid nodules seen on a 123I scan sometimes appear to accumulate 99mTc-pertechnetate. A cold nodule could be a thyroid carcinoma. Therefore, some thyroid cancers might be missed if thyroid imaging is done exclusively with 99mTc-pertechnetate. Some publications recommend that if a 99mTc pertechnetate thyroid scan shows warm or hot palpable nodules and the clinical indication is to rule out thyroid cancer, the scan should be repeated with 123I (11).
Comparison of Radiopharmaceuticals for Thyroid Scintigraphy
Although the SNM guidelines for thyroid imaging do not recommend that patients fast before receiving the radiopharmaceutical, 41% of the respondents ask the patient to fast before receiving the 123I capsule. Fasting would have no effect on the absorption of 99mTc-pertechnetate since it is administered intravenously. However, the oral route of administration may cause 123I absorption to vary from patient to patient. Pharmacokinetically, drugs that are administered orally are dependent on several factors for absorption. They include stomach contents, pH of stomach, and gastrointestinal motility. All 3 are patient-specific and could change if the stomach contains food or medications that affect one of the above factors (12). Therefore, the 41% of the respondents that recommend fasting to patients may be trying to minimize these variables to ensure sufficient uptake of the radiopharmaceutical.
Most respondents take both anterior and oblique views. Markers on the images help to identify anatomic location. The SNM guidelines recommend that duplicate views be taken with and without markers. This recommendation ensures that markers, whether radioactive or nonradioactive, do not obstruct the view of any part of the thyroid. Some clinics use radioactive markers such as 57Co, and some clinics use nonradioactive markers. The recommended number of counts should be collected from the thyroid, not the thyroid plus markers. A substantial number of clinics, 22.8%, reported obtaining only views without markers. A smaller number of clinics (8%) reported that only 1 anterior view is taken and that it is done with markers.
A major variable affecting image resolution is the number of counts acquired. Of the 123I users that responded to question 7, 20% (11/54) acquire less than the minimum recommended 50,000 counts. The recommended acquisition time for 123I imaging is a minimum of 10 min. Again, a significant number of 123I users (29/90, or 32%) reported using an acquisition time of less than 10 min.
The size of the thyroid gland is often a factor used in the determination of a therapy dose for hyperthyroidism (3,4). Only 43.6% of the survey respondents reported a method to size the thyroid gland. We did not find this surprising as ultrasound can also be used to determine the size of thyroid lobes and nodules (13).
A large number of respondents (25.5%) use a parallel-hole collimator exclusively for imaging the thyroid. The exact reason was not identified but may be the cost of a pinhole collimator, the time required to change the collimator, or the lack of availability of a pinhole collimator for purchase with some camera models. During the data collection of this study, we discovered that a camera manufacturer had recommended to one clinic that a parallel-hole collimator be used for thyroid imaging.
CONCLUSION
The procedure used to obtain a thyroid scan varies from site to site. There is much deviation from the recommendations of the SNM guidelines. The greatest deviation from the guidelines occurs in the choice of collimation, the number of counts or amount of time used to acquire the images, and the lack of neck palpation for correlation with the scan.
The number of respondents exclusively using a parallel-hole collimator was surprising. If manufacturers are recommending the parallel-hole collimator for thyroid imaging, this finding warrants further investigation. Have equipment improvements over the years eliminated the need for pinhole images of the thyroid gland? This is the question we are currently investigating.
Continuing education programs offered by professional organizations and societies tend to focus on newer procedures or technology. For commonly performed studies such as thyroid imaging, perhaps there is a need for regular continuing education that may reduce the amount of procedure variability. Our survey did not ask if the nuclear medicine clinic was accredited by the Intersocietal Commission for the Accreditation of Nuclear Medicine Laboratories or by the American College of Radiology. We wondered whether there would be as much variability in the way these studies are performed if the responding clinics were accredited. Accreditation serves to standardize procedures and reporting for optimal patient care.
APPENDIX
Thyroid Imaging Method Survey
-
Which radionuclide do you routinely (most often) use for thyroid imaging?
123I
99mTc-pertechnetate
-
What is the routine dose administered?
-
Explain how the neck is positioned for imaging.
-
Are patients required to fast prior to the radiopharmaceutical administration?
Circle Yes or No
If Yes, for how long?
-
Do you take a history prior to administering the radiopharmaceutical?
Circle Yes or No
-
How many views are routinely taken? Circle all that apply:
anterior without markers
anterior with markers
right and left anterior oblique without marker
right and left anterior oblique with markers
other (please specify below)
-
Is the anterior view image taken for counts or time? Please specify how long or how many counts:
-
Is a method used to size the thyroid gland (such as comparison with a grid picture, radioactive ruler, computer software for sizing the image)?
Circle Yes or No
If Yes, please describe the method used in the space below.
-
Which collimator(s) is/are routinely used for imaging the thyroid?
Circle one of the following:
pinhole collimator only
parallel-hole collimator only
both pinhole and parallel-hole collimators (explain why)
-
Does someone in the imaging department palpate the patient's neck?
Circle Yes or No
If Yes
Is the patient sitting up or lying down?
Is palpating done before or after the images are taken?
Are nodules felt marked on the images or correlated with what is seen on the images?
Who palpates the neck?
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 24, 2008.
- Accepted for publication April 8, 2009.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.