


Abstract
Neuroendocrine tumors (NETs) are rare neoplasms with an exceedingly low incidence of intracranial metastasis. We present a 79-y-old woman with a biopsy-proven pulmonary neuroendocrine tumor who presented with an intracranial mass in the posterior fossa that was avid on 68Ga-DOTATATE PET/CT, facilitating the rare diagnosis of intracranial NET metastasis. The case highlights the utility of advanced imaging techniques in differentiating intracranial NET metastasis from other etiologies.
Neuroendocrine tumors (NETs) typically present in an indolent clinical course, with an incidence of 6.98 per 100,000 (1). These lesions primarily, but not exclusively, originate from the gastrointestinal and bronchopulmonary systems (2). Intracranial metastases of NETs are rare, with an estimated incidence of 1.5%–5% (2,3). The sites of spread in intracranial metastasis are relatively uncharacteristic, with reported metastatic disease in the parenchyma, pineal gland, posterior fossa, dura, and even within an existing meningioma in the skull base (4,5).
Prognosis can vary depending on the NET stage and site of origin. Registry data on 10-y specific survival rates in 6,792 patients with small-intestine NETs found ranges of 77%–95% for locally advanced disease, 68%–77% for nodal disease, and 42% for distant metastatic disease. The median survival time after diagnosis of brain metastasis was 10.0 mo; however, this increased to 3.2 y in patients who underwent resection and whole-brain radiation therapy (3). Therefore, accurate diagnosis of intracranial metastases of NETs plays an important role in providing a reliable prognosis and clinical management.
A rare clinical scenario is a patient with multiple potential primary oncologic processes, making accurate diagnosis more critical for guiding clinical management. We present the case of a 79-y-old woman with biopsy-proven pulmonary NET and additional incidental renal and thyroid lesions who presented with a symptomatic posterior fossa mass with avidity on 68Ga-DOTATATE PET/CT, leading to a diagnosis of intracranial NET metastasis.
CASE PRESENTATION
The patient was a 79-y-old woman who presented because of progressive gait instability over the previous 5 mo. MRI demonstrated a 2.9-cm avidly enhancing mass in the cerebellum containing intralesional hemorrhage (Fig. 1). CT of the chest, abdomen, and pelvis showed a dominant 4.1-cm mass in the left upper lobe of the lung (Fig. 2C) and several lung nodules bilaterally throughout the lungs. CT-guided lung biopsy found an epithelial neoplasm with neuroendocrine differentiation, favoring carcinoid tumor.
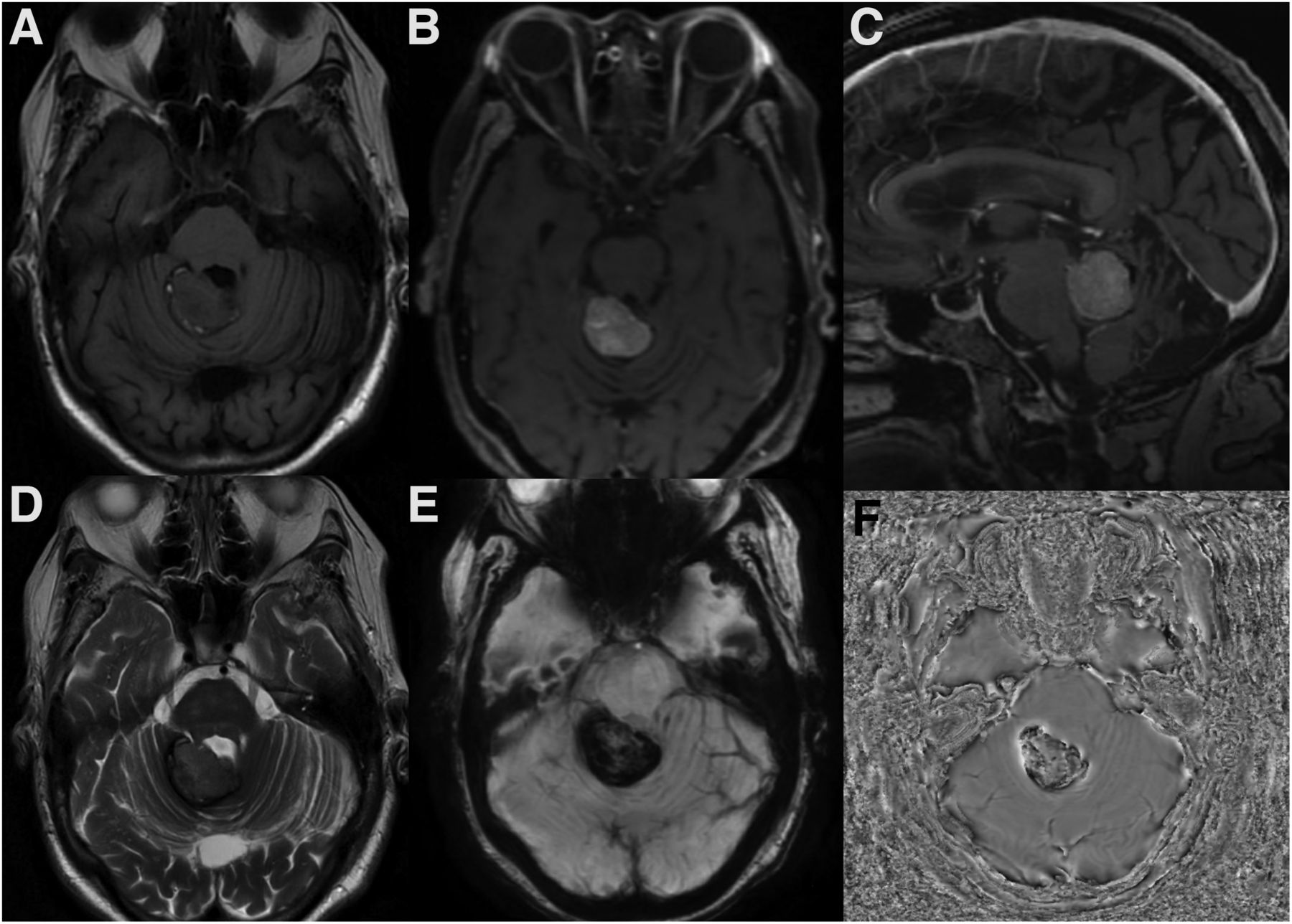
(A) Axial T1 unenhanced image demonstrates an extra-axial posterior fossa lesion in the right superior cerebellar region with predominantly intermediate T1 signal. (B) Axial and (C) sagittal T1 contrast-enhanced images show avid enhancement within this lesion. (D) Corresponding axial T2 image demonstrates intermediate signal intensity. (E) Susceptibility-weighted image and (F) phase image demonstrate signal loss within the lesion, suggesting intralesional hemorrhage.
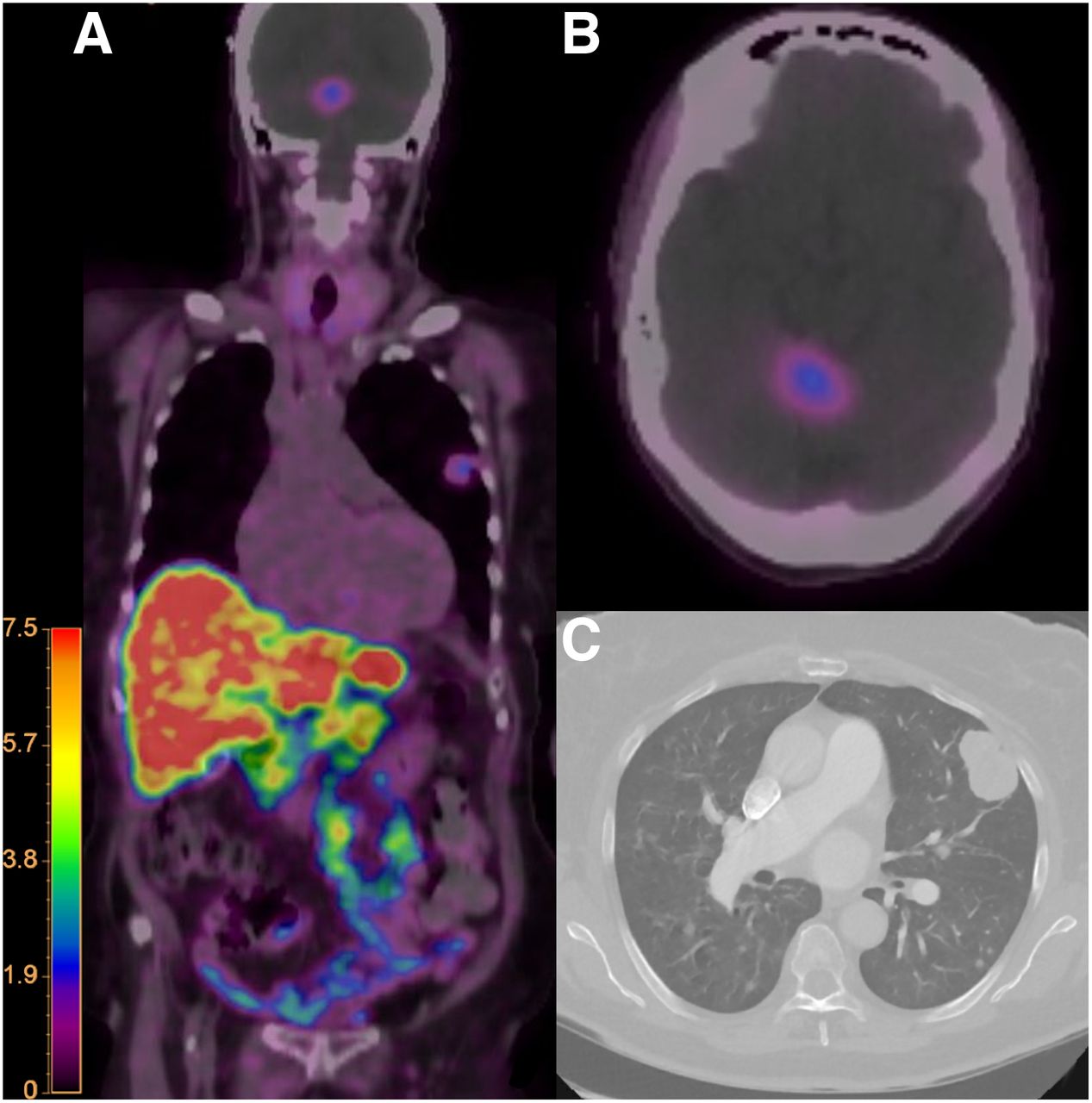
(A) Whole body coronal color fusion map and (B) axial color fusion map 68Ga-DOTATATE PET/CT demonstrate corresponding uptake within the posterior fossa lesion and left lung mass. (C) Chest CT demonstrates the mass in the left upper lob of the lung. Intensity scale bar in units of SUV.
18F-FDG PET CT demonstrated hypermetabolism of the left lung mass (Fig. 3A). The intracranial lesion had 18F-FDG uptake similar to that of the surrounding hypermetabolic brain (Fig. 3B). Additional metastatic workup revealed 2 more lesions: a small 1-cm enhancing right renal lesion and a heterogeneous hypodense left thyroid nodule, both of which have a known propensity for intracranial hemorrhagic metastasis. 68Ga-DOTATATE PET/CT demonstrated corresponding uptake within the focal lesion in the right cerebellum (Fig. 2A) and left lung mass, confirming somatostatin receptor expression in these lesions.

18F-FDG PET/CT. (A) Whole-body coronal fusion map maximal-intensity-projection and (C) axial image of the chest color fusion map demonstrate increased uptake in the left upper lobe lung mass. (B) Axial image of the brain demonstrates uptake in the posterior fossa lesion similarly to that in the hypermetabolic brain parenchyma.
In this case, intracranial metastasis from the thyroid gland and the kidney was essentially excluded as a feasible diagnosis given the 68Ga-DOTATATE uptake. Other intracranial lesions that exhibit 68Ga-DOTATATE uptake include meningiomas and hemangioblastomas. However, intratumoral hemorrhage in meningioma is rare, and hemangioblastomas demonstrate mural enhancing nodules with cystic components on structural brain MRI. Given the presumed recent onset, the 68Ga-DOTATATE avidity, and the hemorrhage, the lesion in this clinical context would likely be a neuroendocrine metastasis.
The patient received 4 d of stereotactic volumetric modulated arc therapy for a total of 3,000 cGy in 5 fractions. On follow-up MRI 3 mo after treatment, the lesion had decreased in size and enhancement. Only monitoring was used for the pulmonary lesions, because of lack of associated symptoms.
DISCUSSION
NETs are a rare and diverse group of neoplasms that generally follow an indolent course and have a high propensity to metastasize. Intracranial NET metastasis is extremely rare, with variable imaging characteristics and distributions on imaging when described in the literature. Functional data from 68Ga-DOTATATE PET/CT provide additional valuable information for lesion characterization, increasing the diagnostic accuracy for NET intracranial metastasis. 68Ga-radiopharmaceuticals have been used for the diagnosis and staging of NETs for multiple reasons. The somatostatin receptor type 2 expression of NETs allows for somatostatin analog radiopharmaceuticals to be used to identify tumors. The gold standard for detection and staging of most NETs is 111In-diethylenetriaminepentaacetic acid-octreotide, with a sensitivity of between 50% and 95%, depending on the subtype of NET (6). However, 68Ga, when linked to a DOTA peptide, demonstrates an increased affinity for somatostatin receptor subtype 2, with the highest affinity being seen for 68Ga-DOTATATE (7). 68Ga-DOTATATE has been shown to be useful in identifying primary and metastatic NETs that express the somatostatin receptor (6). Recent European guidelines on imaging in search of a primary NET include cross-sectional imaging with CT or MRI, followed by 68Ga-DOTATATE PET in combination with native or triple-phase enhanced CT (8).
Although 68Ga-DOTATATE PET/CT helps to distinguish intracranial metastases from NETs versus other primary neoplasms, other intracranial lesions expressing somatostatin receptors, particularly meningiomas and hemangioblastomas, can also demonstrate 68Ga-DOTATATE uptake. Oh et al. reported the case of a 36-y-old woman with von Hippel–Lindau disease in which 68Ga-DOTATATE PET/CT for pancreatic tumor restaging found new avid cerebellar and spinal hemangioblastomas (9). In cases for which distinguishing between meningioma/hemangioblastoma and NET is necessary, structural brain MRI and the clinical context remain crucial to reaching an accurate diagnosis.
CONCLUSION
Intracranial metastases from NETs are extremely rare and can have an uncharacteristic and variable imaging appearance on conventional imaging. Accurate diagnosis of these lesions is important to provide a reliable prognosis and to guide appropriate treatment. This case report demonstrates the utility of 68Ga-DOTATATE PET CT in combination with conventional imaging, providing more robust lesion characterization and an accurate diagnosis in this patient with NET intracranial metastasis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 4, 2023.
REFERENCES
- Received for publication August 26, 2022.
- Revision received November 7, 2022.





{kind=link}
{kind=link}
{kind=link}