


Visual Abstract

Abstract
Our aim was to explore whether the 360° γ-camera design of the Veriton-CT scanner adversely affects the rate of scan noncompletion due to claustrophobia or other patient experience factors, when compared with a standard dual-head Discovery NM/CT 670 γ-camera. Methods: This was a single-center prospective study of all nuclear medicine studies on either of the 2 γ-cameras. It was recorded whether the patient completed the scan as protocoled or, because of claustrophobia, had a shortened scan or no scan. The patients were also offered a patient experience questionnaire, with domains of comfort, scan time, scan noise, and claustrophobia assessed using a 5-point Likert scale. Results: Over a 4-mo period, 296 patients were scanned on the Discovery and 274 patients on the Veriton-CT. There was a scan noncompletion rate, due to claustrophobia, of 1.35% for the Discovery and 1.46% for the Veriton-CT. Of the 570 patients involved, 354 (62%) returned their questionnaires. There was no statistical difference between the responses for comfort, scan time, scan noise, or feelings of claustrophobia. Conclusion: The study provides evidence that the 360° γ-camera design of the Veriton-CT does not lead to a significantly increased scan failure rate due to claustrophobia and that there is no change in the subjective experience for patients.
SPECT imaging and hybrid SPECT/CT imaging have undergone multiple developments since the first commercial SPECT/CT scanner became available over 20 years ago (1). Identifying the clinical indication of optimized localization and quantification of tracer uptake was essential to the increasing clinical utility (1). Moreover, the continued advances in detectors and the emergence of digital cadmium-zinc-telluride cameras have allowed for improved extrinsic resolution (2), increased count sensitivity, and reduced scan times (3). These advantages allow for superior image quality and presentation using maximum-intensity projections but should be balanced against a patient’s ability to tolerate the scan. Although there are limited published data on whether patients experience claustrophobia during γ-camera examinations, claustrophobia is a shared theme with other high-technology medical imaging modalities such as MRI, for which potential negative experiences of discomfort and claustrophobia need to be considered (4–9). One study showed that 10% of children undergoing 3-T MRI report feelings of claustrophobia (4), and in another study, up to 40% of adults undergoing MRI experience feelings of unpleasantness due to a “confined space” (8). A focus on improving patients’ experience and using a patient-centered approach is paramount in the development and planning of radiology services (10).
In November 2020, a new SPECT/CT scanner with cadmium-zinc-telluride detectors (Veriton-CT; Spectrum Dynamics Medical) was installed in our local nuclear imaging department as a replacement for one of the older cameras. Unlike conventional dual-head Anger cameras, the Veriton-CT comprises a novel setup design, with 12 detectors in a 360° configuration that can be moved closer to the patient during image acquisition. During the scanner procurement process, we wanted to ensure that patients would tolerate this novel design. Acquiring the new scanner presented an opportunity for reflection and exploration of the patient experience of nuclear imaging within the department. The aim of this study was to assess claustrophobia in our patients by comparing the local scan-noncompletion rate, due to claustrophobia, between the new Veriton-CT and a conventional dual-head Discovery NM/CT 670 (GE Healthcare) γ-camera. Secondarily, we wanted to prospectively survey our patients about their subjective perception of several experience factors, including claustrophobia. Together, these investigations could provide both objective and subjective measures of scanner tolerability.
MATERIALS AND METHODS
The institutional review board approved this study, and the requirement to obtain informed consent was waived. This study was registered with the local clinical audit department. The patient experience team of the local hospital was involved from the start of the project and was invited to the nuclear imaging department, where they were able to view the available scanners and patient flow areas. Neither of the 2 scanner manufacturers was involved in the study design or manuscript review. On request, Spectrum Dynamics Medical supplied an image highlighting the different scanner designs.
Scanners and Patients
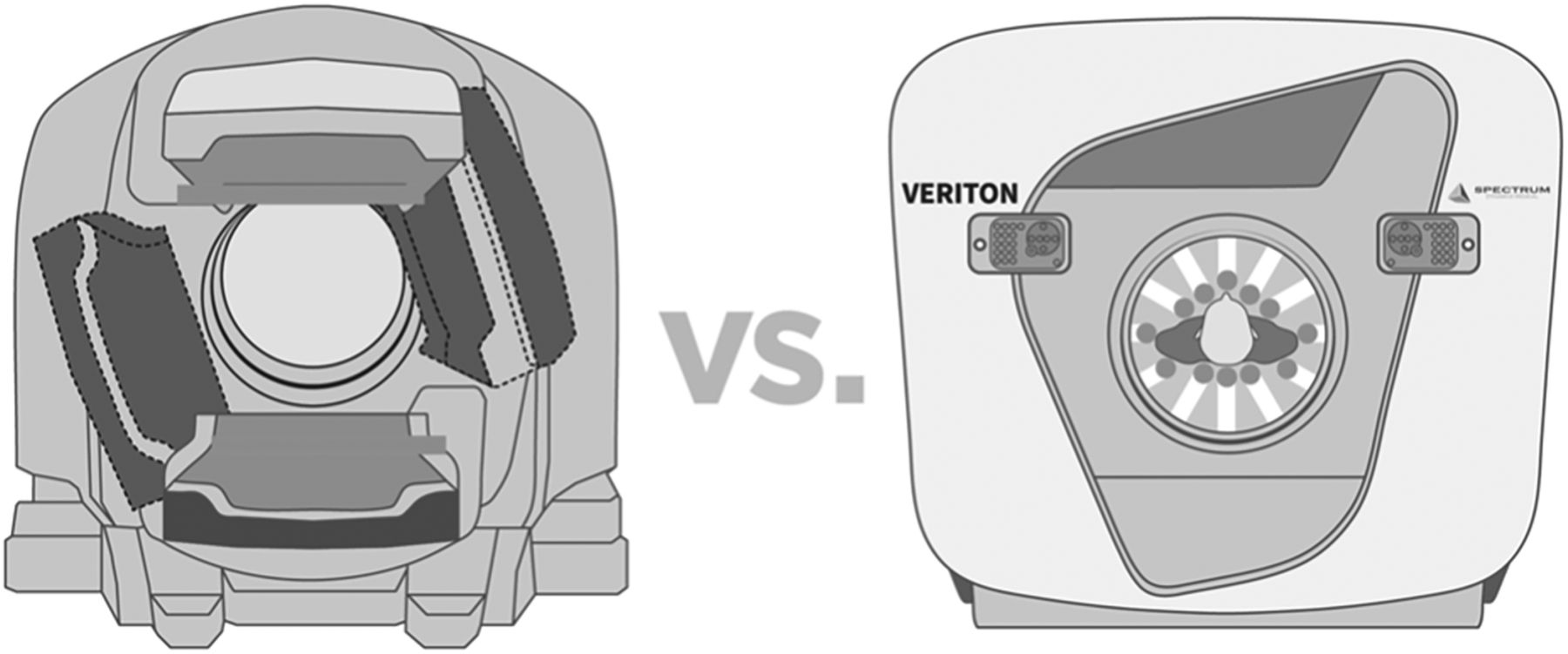
All patients presenting for nuclear imaging scans between October 28, 2020, and March 12, 2021, were included for analysis. Studies were performed on either of the 2 department scanners. The Discovery was installed in November 2012, and the Veriton-CT was installed in November 2020. The characteristics of each scanner are shown in Table 1, and a graphical representation of the difference between a conventional γ-camera and the Veriton-CT is shown in Figure 1. Patient positioning is similar between the 2 scanners. Of note, Veriton-CT protocols are generally shorter than corresponding protocols on the Discovery. For example, an oncology whole-body bone scan takes approximately 18 min on the Veriton-CT (3), whereas a bone scan and single-site SPECT take 40 min on the Discovery.
Characteristics of Nuclear Imaging Scanners in Our Department

Conventional Anger camera (left) vs. Veriton-CT scanner (right), with 360° detector design. (Courtesy of Spectrum Dynamics Medical.)
After consideration of the volumes and types of scans going through the department and the process of protocol development, initially it was decided that the Veriton-CT would be used for bone, parathyroid, and lung imaging, with a plan to gradually introduce other indications. During the study period, bone, parathyroid, and lung scans were protocoled for either of the 2 scanners, and the local radiology bookings team allocated the patients on the basis of efficient use of scanning slots. When patients expressed anxiety about the Veriton-CT, they were given the option of undergoing their scan on the Discovery instead.
Questionnaire Development
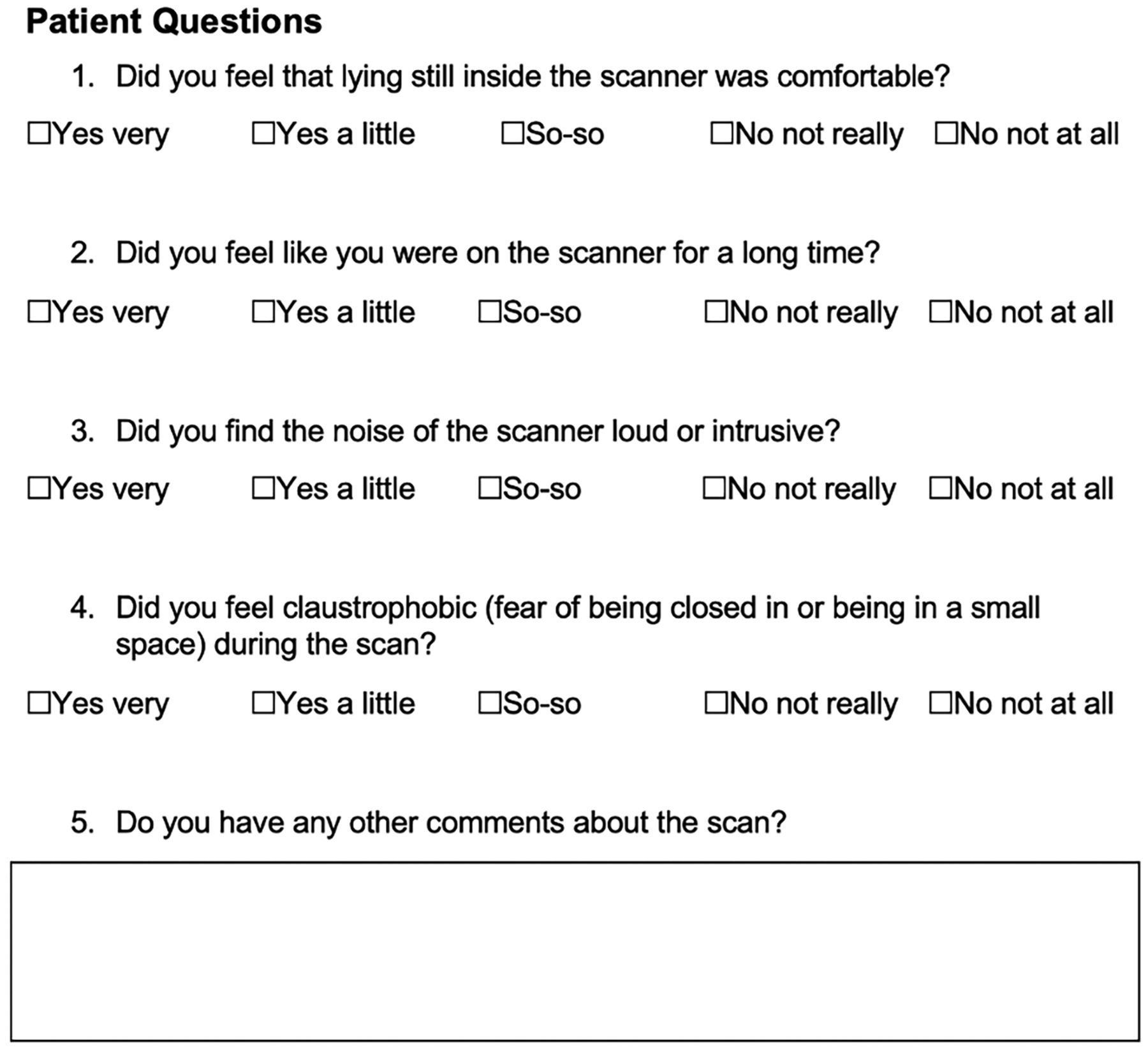
A review of current literature regarding the patient experience of medical imaging revealed similar studies of patient experience and tolerability of MRI and nuclear imaging (4–8). Informed by one of these studies (4), a cross-sectional patient experience questionnaire was drafted, which contained 4 measures of scan experience (comfort, scan time, scan noise, and claustrophobia). The draft was reviewed by the hospital patient experience team. The final questions are shown in Figure 2. During the prospective data-collection phase, demographic data for all patients undergoing nuclear imaging were recorded in a spreadsheet along with information about whether they completed their scan as protocoled. After the scan, patients were offered a paper questionnaire to fill out before leaving the department. The reception staff then collected the questionnaire from the patient and recorded the responses in the spreadsheet.

Questionnaire on experience of nuclear imaging patient.
Quality Checking and Statistical Analysis
The prospectively collected data were cross-referenced against a retrospectively generated patient list from the radiology information system, to ensure no patients were missed. Whether scans were completed as protocoled was assessed. Variations in the survey responses were assessed using the χ2 test. Differences in scan noncompletion numbers between the Discovery and the Veriton-CT were assessed using the Mann–Whitney U test. Two-tailed tests were used, and a P value of less than 0.05 was considered statistically significant. All statistical analysis was performed on GraphPad Prism, version 9, for the Mac operating system (Apple).
RESULTS
Study Group
Between October 28, 2020, and March 12, 2021, 296 patients were scanned on the Discovery and 274 were scanned on the Veriton-CT. There was a 62% (354/570) overall questionnaire-response rate. The spread of nuclear imaging scan indications across the 2 scanners is shown in Table 2.
Spread of Nuclear Imaging Scan Indications Across Discovery and Veriton-CT over 4-Month Period
Rate of Scan Noncompletion as Protocoled
All patients presenting for nuclear imaging had some form of imaging during their visit. Overall, 6 of 570 (1.05%) patients failed to complete their scan as initially protocoled, because of claustrophobia (Table 3). Four of these patients were booked on the Veriton-CT; of these, one was able to have a partial scan on the Veriton-CT (patient 1), 2 were able to have a partial scan on the Discovery (patients 2 and 3), and one was able to have a complete scan on the Discovery (patient 4). Two further patients were initially booked on the Discovery (patients 5 and 6) and were able to have only partial scans because of claustrophobia. This gives a composite rate of scan noncompletion as protocoled of 4 of 274 (1.46%) for the Veriton-CT and 4 of 296 (1.35%) for the Discovery (P = 0.33, Mann–Whitney U test), because of claustrophobia.
Patient Characteristics of Noncompleted Scans Due to Claustrophobia
Survey Responses
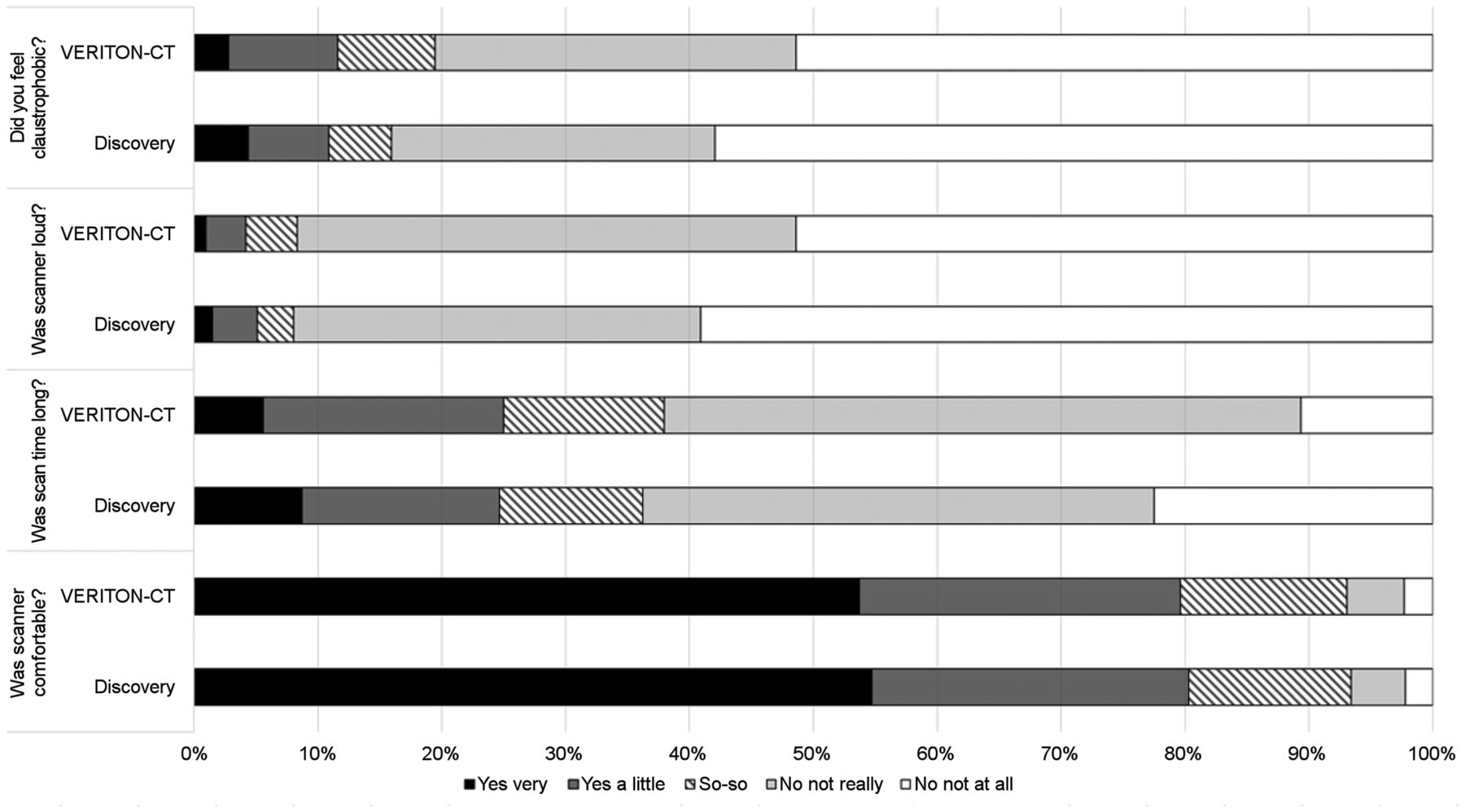
The modal responses in the different experience parameters for each of the scanners was as follows: comfort was “yes very,” long scan time was “no not really,” loud scan noise was “no not at all,” and claustrophobia was “no not at all.” There was no statistical significance in the spread of the 5-point scale responses across the 2 scanners, when compared using the χ2 test: comfort (P = 0.84), long scan time (P = 0.39), loud scan noise (P = 0.46), and claustrophobia (P = 0.44). In particular, the overall subjective reporting of claustrophobia (patients who answered, “yes very” and “yes a little”) was 15 of 138 (10.9%) for the Discovery and 25 of 216 (11.6%) for the Veriton-CT (P = 0.87). A graphical representation of the spread of responses from all surveyed patients, comparing the Veriton-CT and the Discovery, is shown in Figure 3.

Spread of survey responses across 4 experience factors.
DISCUSSION
It is recognized that high-technology imaging presents a potential source of patient anxiety, which can limit adequate scan completion (4–9). We sought to assess the claustrophobia rate in 2 ways. First, we recorded the rate of scan noncompletion due to claustrophobia and found that few patients were unable to complete their scan fully on the Veriton-CT or Discovery (1.46% and 1.35%, respectively). All patients were able to complete at least part of their scan, which is the most important outcome. Second, a survey of subjective perception of several experience factors was conducted. The modal responses support the finding that overall patient experience is positive across the 2 scanners. Moreover, there was no statistical significance across the responses from the 2 scanners. This shows that the 360° configuration of the Veriton-CT does not significantly affect the subjective patient experience.
There is strong heterogeneity in patient groups for bone imaging, as there was no dynamic bone imaging protocol established for the Veriton-CT. Hence, bone scans for indications such as postarthroplasty imaging, which involved a 3-phase acquisition, were protocoled for the Discovery. This makes subgroup analysis difficult.
Comfort is essential for nuclear imaging as scan times vary greatly but can be up to 1 h long, and it is important for the patient to be able to lie relatively still. The patient tables for the 2 scanners are similar to each other, and it is understandable that there was no difference in perceived comfort. Although this question is likely to be answered mainly from a physical perspective, it seems probable that if patients were feeling psychologic discomfort from claustrophobia, this psychologic discomfort might also have affected the responses to this question. Many of the Veriton-CT scan protocols are shorter than corresponding protocols on the Discovery. For example, an oncology whole-body bone scan takes approximately 18 min on the Veriton-CT (3), whereas a bone scan and single-site SPECT take 40 min on the Discovery. However, there is no observed subjective difference in the patient appreciation of scan time. The results from this study give an overview of patient perceptions of scan time, but a separate study including actual time spent on the scanner would be required to draw further conclusions.
The subjective experience of scanner noise also did not reveal any statistical difference between the 2 scanners. Of note, the measured sound level during CT scanning in the Discovery was 74 dB, and that in the Veriton-CT was 72 dB.
For a minority of patients, claustrophobia is a deterring factor in medical imaging (4–9). The subjective experience of claustrophobia was relatively low: 10.9% for the Discovery and 11.6% for the Veriton-CT. The nuclear imaging technologists are experts in strategies to reassure patients and guide them comfortably through the scan as much as possible. With this expertise, all patients attending the department were able to complete at least part of their scan. Three patients declined to be scanned at all on the Veriton-CT, whereas all the patients completed at least part of their scan on the Discovery.
There is a potential for subconscious bias among the technologists, who are more familiar with the double-head camera setup of the Discovery. From an ethical standpoint in a 2-scanner department, it is understandable that patients who showed anxiety about the Veriton-CT were given the option to attempt their scan on the Discovery instead. Conversely, patients who were booked for the Discovery were encouraged to complete as much of the scan as they could but were not offered the Veriton-CT scanner as an alternative, because the technologists have years of experience in getting patients through their scans on the Discovery. It is therefore not possible from our study design to say what the rate of scan noncompletion would be for the Veriton-CT if it were the only scanner available. It is possible that some, if not all, of the patients (patients 2–4) would have partially completed their scans on the Veriton-CT.
We have not sought to assess what an individual patient’s experience of both scanners would be as a head-to-head comparison, as this would involve scanning the patient twice and potentially on different days. Such an assessment would be both impractical and unethical. However, we believe the relatively large numbers in our study allow us to draw reasonable conclusions without the need to scan patients on both scanners. Going forward, we aim to establish a protocol for brain 123I-ioflupane scans (DaTscans; GE Healthcare) on the Veriton-CT. This type of scanning brings the detector heads very close to the patient’s face, and it will be interesting to see whether there is a difference in the rate of scan noncompletion due to claustrophobia or the subjective perception of claustrophobia in this cohort of patients.
CONCLUSION
The 360° SPECT/CT scanner configuration brings the 12 detectors close to the patient, allowing the potential for improved image quality and resolution but raising a question as to whether this proximity can be tolerated by patients. This observational cohort study provides evidence that this scanner configuration does not significantly affect the rate of scan noncompletion due to claustrophobia or the subjective perception of claustrophobia, when compared with the conventional double-head scanner. This finding should reassure nuclear medicine departments regarding this novel design.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does the novel γ-camera design of the Veriton-CT adversely affect the rate of scan noncompletion due to claustrophobia, when compared with a standard dual-head γ-camera?
PERTINENT FINDINGS: This observational cohort study shows that the 360° SPECT/CT scanner configuration does not significantly affect the rate of scan noncompletion due to claustrophobia (1.46% compared with 1.35% with the conventional γ-camera) or the subjective perception of claustrophobia (10.9% compared with 11.6% with the conventional γ-camera).
IMPLICATIONS FOR PATIENT CARE: The 360° SPECT/CT scanner configuration of the Veriton-CT has the potential to improve image quality and resolution without having a negative impact on the patient experience. This finding should reassure nuclear medicine departments that are considering this novel design.
ACKNOWLEDGMENTS
We thank the nuclear medicine technologists for collecting the data and supporting patients during the study and throughout their careers.
Footnotes
Published online Nov. 8, 2021.
REFERENCES
- Received for publication May 25, 2021.
- Revision received September 25, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.