


Abstract
Panitumumab is a new humanized antiepidermal growth factor receptor monoclonal antibody (mAb) approved for the treatment of advanced colorectal cancer. There is an increase in the use of this drug due to a good response rate and possible secondary resection in advanced colorectal cancer. Here, we present 18F-FDG PET/CT imaging findings of cardiac arrhythmia in a patient receiving panitumumab for the treatment of metastatic infiltrating rectal adenocarcinoma. Cardiotoxicity is a known adverse effect associated with panitumumab. So far, to our knowledge, no documented imaging findings for the same are available in the literature.
Panitumumab is used as a targeted immunotherapy for metastatic colorectal carcinoma as a first-line or second-line treatment (1). The adverse effects of this drug include skin-related toxicity as well as cardiotoxicity. The following case represents imaging features of newly diagnosed cardiac arrhythmia in a patient treated with panitumumab.
CASE REPORT
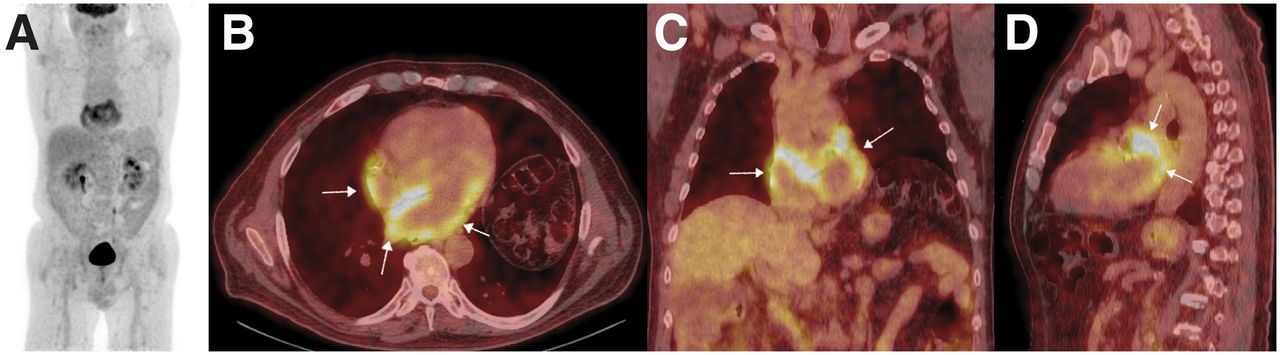
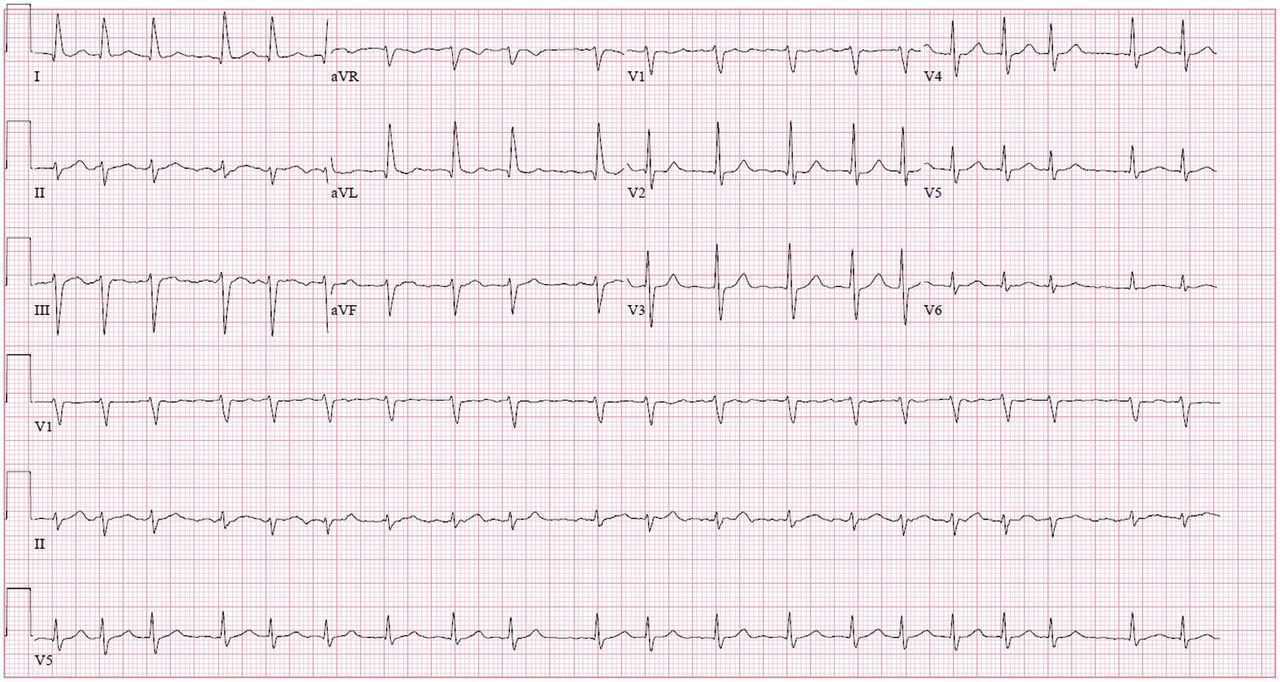
A 68-y-old nonsmoker man presented with intermittent hematochezia of 6-mo duration. He underwent colonoscopy, which showed a large fungating, ulcerated, and nonobstructing mass in the rectum. Biopsy from the lesion revealed infiltrating adenocarcinoma of the rectum. The carcinoembryonic antigen level was high and KRAS/NRAS/BRAF wild-type was positive. The patient underwent staging 18F-FDG PET/CT, which showed an 18F-FDG–avid hepatic lesion in the right lobe, in addition to an 18F-FDG–avid rectal wall thickening and perirectal lymph nodes. The myocardium demonstrated diffuse blood-pool tracer activity without any distinct abnormal focal tracer uptake (Fig. 1). Biopsy from the liver lesion was positive for adenocarcinoma metastasis. The patient was staged as advanced colorectal adenocarcinoma (stage IV) and was started on the FOLFOX regimen (folinic acid, fluorouracil, and oxaliplatin) with panitumumab. There was interim microwave thermal ablation of the hepatic lesion. After 8 cycles of combination chemotherapy, follow-up 18F-FDG PET/CT was performed 9 mo after the prior imaging. It demonstrated a reduction in the metabolic activity of primary rectal mass lesion and resolution of 18F-FDG avidity in the metastatic hepatic lesion. There was an incidental finding of intense 18F-FDG uptake in bilateral atrial walls with relatively intense uptake in the left atrium, maximum metabolic activity (SUVmax) of 9.2 (Fig. 2). The patient underwent cardiac evaluation with electrocardiography, which showed an irregular rhythm, with changes of left-axis deviation, atrial fibrillation, and a rapid ventricular response (Fig. 3). Echocardiography showed normal systolic function, with an ejection fraction of 55% and no evidence of thrombus. Comprehensive metabolic panel, including electrolytes, was within the reference range. A clinical diagnosis of cardiac arrhythmia secondary to cardiotoxicity from the antiepidermal growth factor receptor (EGFR) inhibitor panitumumab was postulated. The panitumumab was discontinued, and the patient was treated with diltiazem, with consideration of future abdominoperineal resection of the rectal tumor mass.
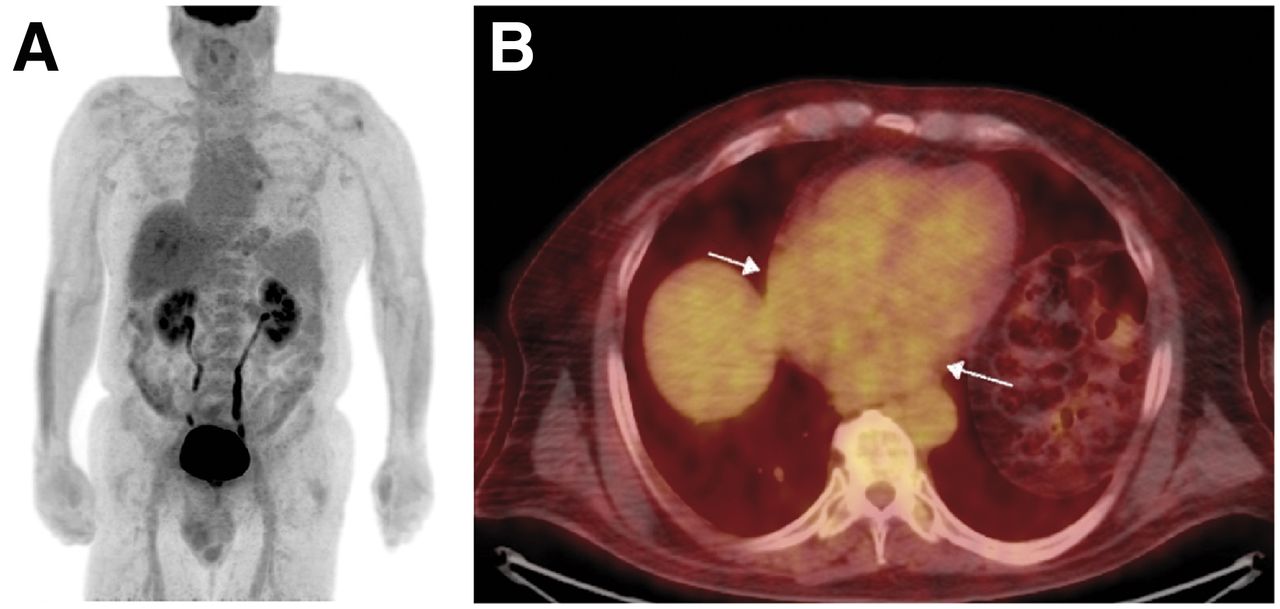
(A) Maximum-intensity projection of whole-body 18F-FDG PET/CT pretherapy staging scan in patient with colorectal cancer. Imaging was performed 62 min after intravenous injection of 362.6 MBq (9.8 mCi) of 18F-FDG. (B) Transaxial 18F-FDG PET/CT image demonstrating diffuse blood-pool 18F-FDG activity in myocardium (arrows), with SUVmax of 3.3 and SUVmin of 1.8.

(A) Maximum-intensity projection of whole-body 18F-FDG PET/CT scan in patient who had received combination therapy (FOLFOX regimen plus panitumumab) for colorectal cancer. Imaging was performed 66 min after intravenous injection of 436.6 MBq (11.8 mCi) of 18F-FDG. (B–D) Transaxial (B), coronal (C), and sagittal (D) 18F-FDG PET/CT images demonstrating intense 18F-FDG uptake in bilateral atrial walls (white arrows). Uptake is more intense in left atrium, with SUVmax of 9.2 and SUVmin of 5.9.

Electrocardiography demonstrating irregular rhythm, with changes consisting of left axis deviation, atrial fibrillation, and rapid ventricular response.
DISCUSSION
Colorectal cancer is one of the most common cancers worldwide. Median survival in metastatic colorectal cancer has improved because of combined use of chemotherapy and targeted agents (1) such as antivascular endothelial growth factor and anti-EGFR therapies. Panitumumab is a human immunoglobulin G2 monoclonal antibody against EGFR. It binds with the EGFR, reduces cell proliferation, and induces apoptosis (2). There are adverse effects associated with panitumumab, such as skin-related toxicities and cardiac arrhythmias. Preexisting cardiac disease and hypertension are assumed to increase the risk of developing cardiac arrhythmia (3). Qi et al. reported an overall 8.4% increase in the incidence of cardiac events with panitumumab combination therapy, as compared with 6.8% with chemotherapy alone (3). 18F-FDG PET/CT usually demonstrates variable tracer uptake in the myocardium, a finding that is presumed to be due to shifting of metabolism between glucose and fatty acids (4). In cases of cardiac arrhythmia, there may be distinct abnormal increase in myocardial 18F-FDG uptake (5). According to a study published by Sinigaglia et al. (6), diffuse increased 18F-FDG uptake in the atrium was seen in one third of patients with atrial fibrillation, and the intensity of 18F-FDG uptake was associated with underlying heart rhythm. The article also suggested an association between an increased risk of stroke and a detectable abnormality in atrial 18F-FDG uptake. Though 18F-FDG uptake in the myocardium is considered nonspecific on 18F-FDG PET scans performed for oncology purposes, for the above-mentioned reason the reading physician should be aware of certain patterns of tracer uptake indicative of the underlying disease process. As seen in this case, the patient treated with panitumumab had new atrial fibrillation with increased atrial wall 18F-FDG activity, findings that were attributed to possible cardiotoxicity, known to be associated with anti-EGFR immunotherapy.
CONCLUSION
Incidental findings on whole-body 18F-FDG PET/CT scans performed for oncological purpose may point toward underlying metabolic abnormalities. Although cardiac uptake on whole-body 18F-FDG PET scans is nonspecific, an abnormal myocardial 18F-FDG uptake pattern may occasionally warrant further investigation. Cardiotoxicity associated with panitumumab may present as an abnormal finding on 18F-FDG PET scans, as demonstrated in this case. Knowledge about such patterns of tracer uptake will improve diagnostic efficiency and contribute to holistic patient care.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online July 30, 2021.
- Received for publication March 1, 2021.
- Revision received May 20, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.