


Abstract
We present a case that caused a diagnostic dilemma on a bone scan. We also review the broad spectrum of nonmalignant findings that can impact the interpretation of a bone scan and the value of correlative imaging using SPECT/CT for exact localization and characterization of lesions. The imaging features of important benign pathologies—that is, metastatic mimics—are elaborated so that the reader can avoid misinterpretations when reporting them. We elucidate 4 uncommon benign findings on a bone scan. Rhabdomyolysis is a result of lysis of skeletal muscle with release of cell contents, such as myoglobin and muscle enzymes, and is diagnosed mostly through a combination of clinical appearance and laboratory values. Myositis ossificans is the most common form of heterotopic ossification, usually occurring within large muscles. Its importance stems largely from its ability to mimic more aggressive pathologic processes. Myositis ossificans is one of the skeletal “do not touch” lesions. Such bone lesions are defined by characteristic imaging features, the identification of which precludes the need for additional diagnostic tests or biopsies, thereby avoiding unnecessary interventions. Acute tubular necrosis is kidney injury caused by damage to the kidney tubule cells (kidney cells that reabsorb fluid and minerals from urine as it forms). Common causes are low blood flow to the kidneys, drugs that damage the kidneys, or a severe underlying infection.
Bone scanning continues to be the second most commonly used nuclear imaging procedure after nuclear cardiac scans, offering the advantage of total-body examination, low cost, and high sensitivity not only for metastatic lesions but also for benign conditions. Its power rests in the physiologic uptake and pathophysiologic behavior of 99mTc- diphosphonates (1). Radiotracers localize in damaged skeletal muscles because calcium builds up in them and, when combined with phosphate, provides a site for radiotracer deposition (1).
In a case of suspected rhabdomyolysis, not only is bone scintigraphy a sensitive indicator of muscle damage but also the amount of uptake is proportional to the extent of myonecrosis (2–5). Specifically, in sports medicine, bone scintigraphy could be a valuable tool in discriminating bone trauma from muscle trauma (6).
We present an unusual case of a 19-y-old woman who experienced heat stroke and whose bone scan presented several unusual findings; this case demonstrates important teaching points.
CASE REPORT
As per our institute protocol, the patient was injected with 925 MBq of 99mTc-methyldiphosphonate, and after 2.5 h whole-body anterior and posterior images of the entire skeleton were obtained using a γ-camera with gantry motion of 10 cm/min, a matrix size of 256 × 1024, and no magnification. Subsequently, for better visualization of related pathologies, SPECT images of the chest and upper abdomen were obtained using a 360° rotation, noncircular step-and-shoot mode, 128 steps, 20 s per step, a matrix size of 128 × 128, and no magnification.
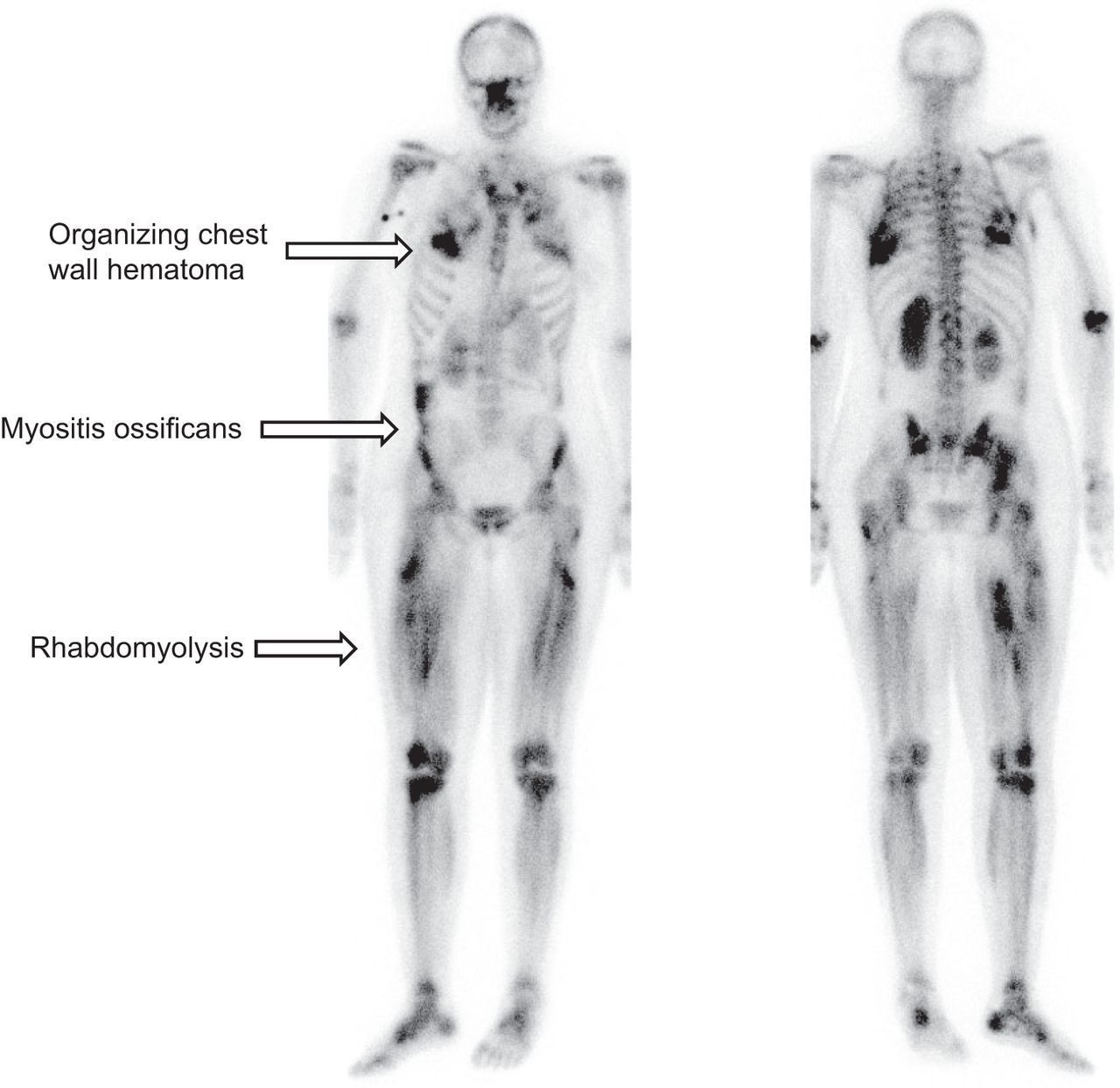
The whole-body planar and SPECT/CT images demonstrated abnormal radiotracer uptake suggestive of rhabdomyolysis in the muscles of the lower extremity, abnormal bilateral cortical uptake suggestive of acute tubular necrosis within the kidneys, greater abnormal uptake in the right than the left pleural space suggestive of organizing hematoma, and abnormal uptake within the abdominal musculature suggestive of myositis ossificans.
DISCUSSION
Rhabdomyolysis is a complex medical condition leading to disruption of skeletal muscle integrity. This disruption can lead to the direct release of intracellular muscle components such as myoglobin, creatine kinase, aldolase, and lactate dehydrogenase into the bloodstream and extracellular space (2–4).
Bone scans are a sensitive way to visualize muscle injury and have been used with 99mTc-diphosphonate and several similar agents in a wide variety of conditions, including exercise injuries (6), seizures, crush injuries, and polymyositis, and are a good indicator of acute rhabdomyolysis. Myositis ossificans is essentially metaplasia of the intramuscular connective tissue resulting in extraosseous bone formation. Examination of the soft-tissue lesion using 99mTc-diphosphonate bone scans has been helpful in establishing the diagnosis and in determining the full extent of the process early in its evolution (6).
Another important utility of 99mTc-diphosphonate bone scans lies in evaluation of acute renal failure after exercise with flank pain and patchy renal vasoconstriction due to acute tubular necrosis. These findings have been shown in multiple reports, with a prominent example being one written by Watanabe et al. (7). We also found an organizing pleural hematoma with radiotracer uptake. Localization of bone-imaging 99mTc-diphosphonate agents has previously been described in abdominal, chest wall, and pelvic hematomas (8,9).
CONCLUSION
It is extremely important for all 4 benign conditions described above to be recognized on a bone scan. We hope this report educates the reader about the types of uncommon conditions that can be seen on bone scans.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.

Whole-body 99mTc-methyldiphosphonate SPECT/CT image demonstrating abnormally increased uptake in organizing chest hematoma, myositis ossificans, and rhabdomyolysis. Increased bilateral uptake in several locations in lower extremities along length of muscle corresponds to pattern of rhabdomyolysis.

SPECT/CT images demonstrating abnormally increased radiotracer uptake in organizing chest wall hematoma. (Top left) CT image of chest demonstrating chest wall hematoma. (Top right) SPECT image demonstrating abnormally increased uptake within hematoma. (Bottom left) SPECT/CT image demonstrating abnormally increased radiotracer uptake (arrow) corresponding to underlying chest wall hematoma. (Bottom right) Rotating maximum-intensity projection SPECT image demonstrating focal region of uptake in right chest. Also seen is faint focus of uptake in left chest (additional site of hematoma).

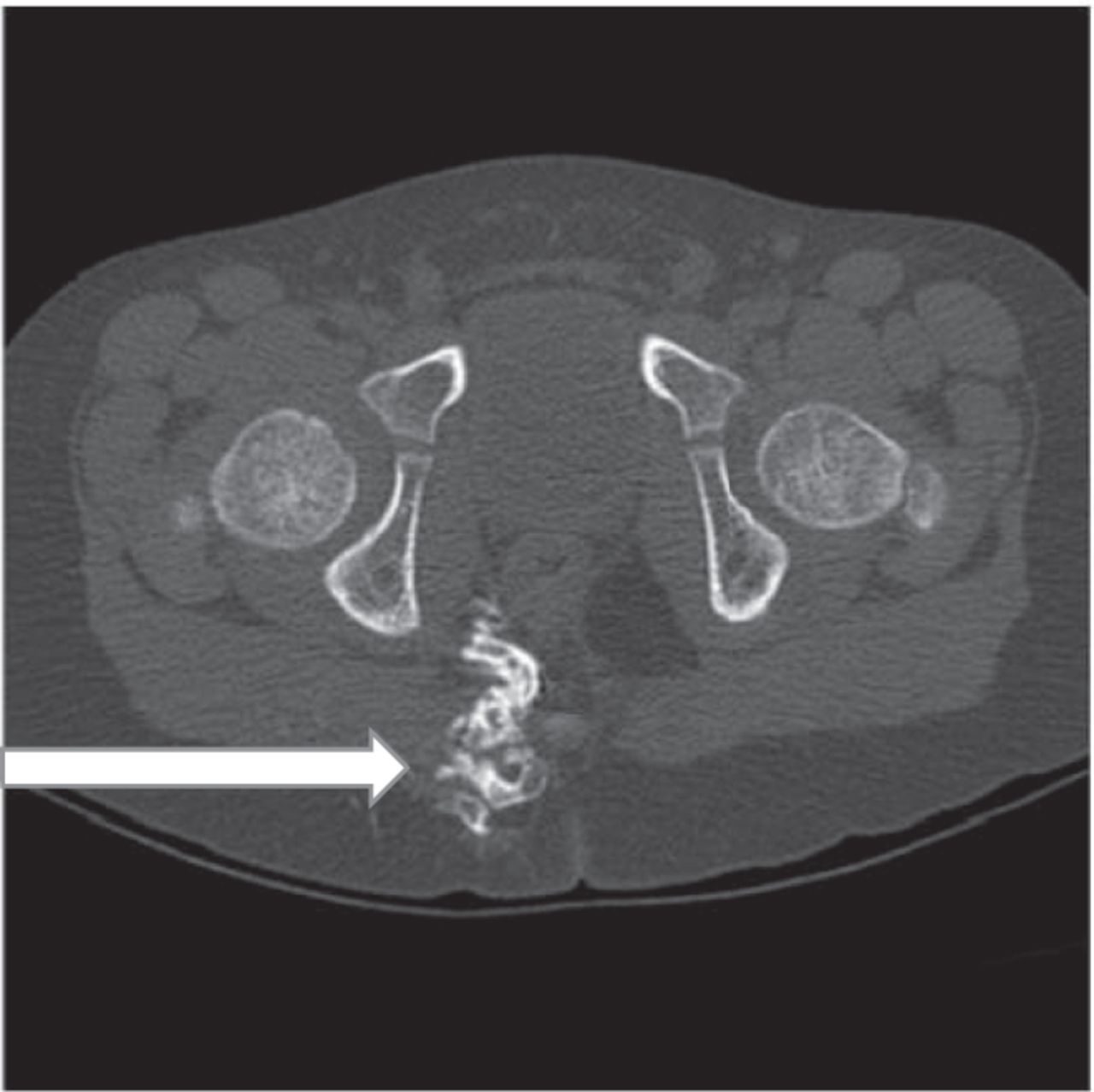
CT images in bone window demonstrating focus of myositis ossificans (new bone formation, arrow) in pelvis.

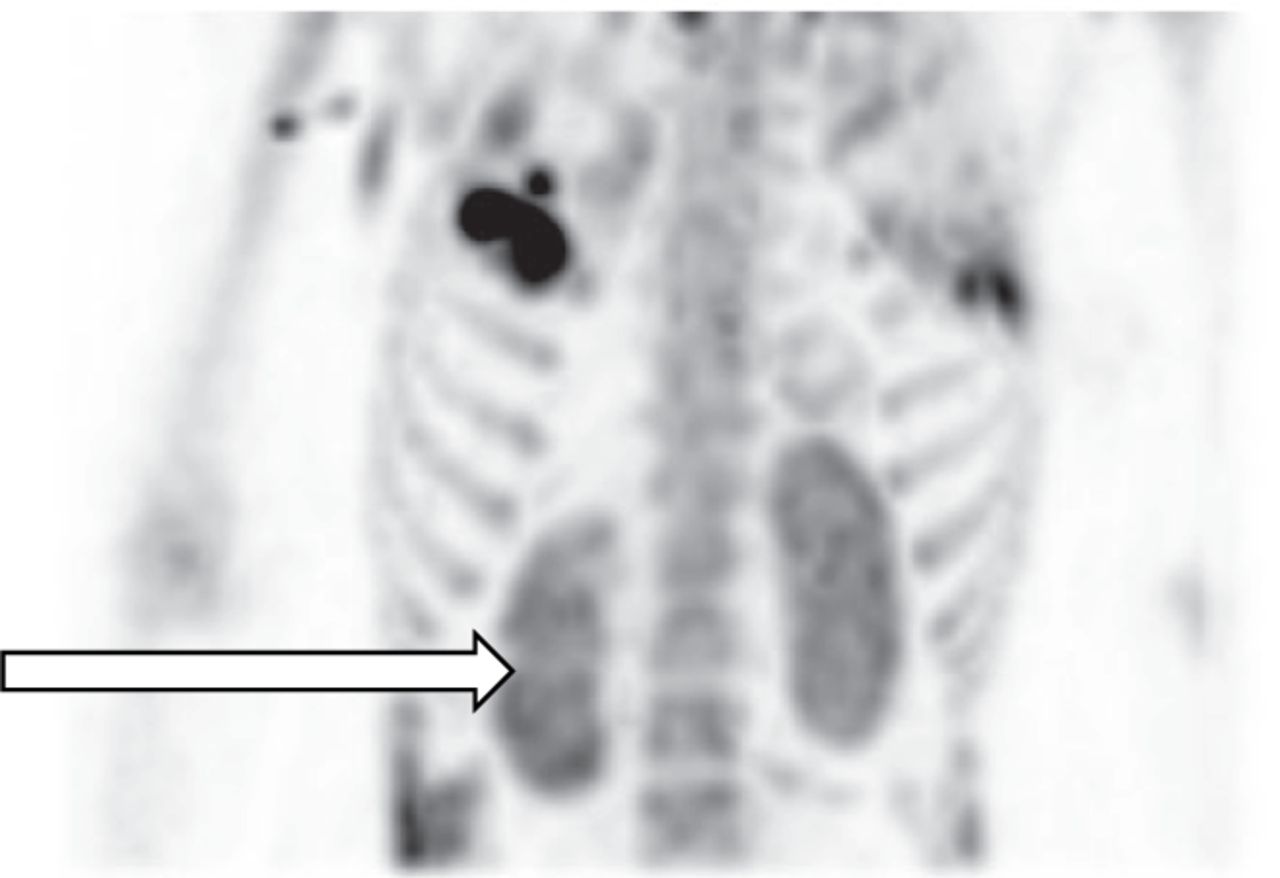
Planar image demonstrating abnormally increased bilateral cortical retention of radiotracer in kidneys in pattern of acute tubular necrosis.

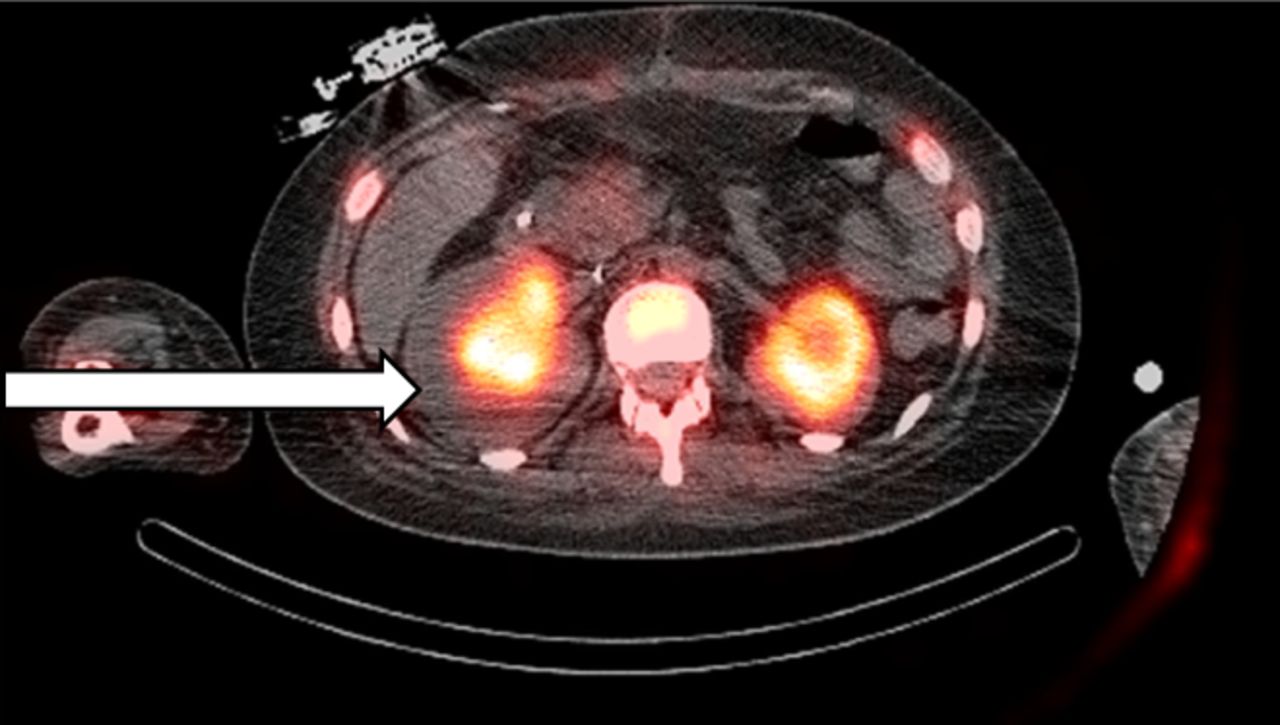
SPECT/CT image demonstrating abnormal bilateral cortical retention of radiotracer in kidneys, corresponding to acute tubular necrosis.
Footnotes
Published online July 30, 2021.
REFERENCES
- Received for publication April 27, 2021.
- Revision received June 10, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.