


Abstract
Lung cancer is the number 1 cause of cancer deaths in the United States. The prognosis is quite grim with the exception of stage 1. When faced with several failed therapeutic regimens and rapid progression of the disease, considering alternative therapies such as radiopharmaceutical therapies may be an option. We describe the case of a 36-y-old man with lung adenocarcinoma who had imaging molecular characterization of his disease with 18F-FDG, 68Ga-DOTATATE, and 18F-fluoride PET/CT scans that were able to shed some light on molecular characterization of his disease and serve as a guide to potential targeted or personalized radiopharmaceutical therapeutic options.
Lung cancer is the number 1 cause of cancer deaths in the United States. The overall 5-y survival is 12% (1). The adenocarcinoma subtype is the most common primary lung cancer. The prognosis is quite grim with the exception of stage 1 (1,2). Somatostatin receptor expression has been described in lung cancer in general and also specifically in lung adenocarcinomas (3–6). Today, β- and α-emitters are available for treatment clinically. The Food and Drug Administration and the European Medicines Agency have approved 177Lu-DOTATATE and 223Ra for the treatment of gastroenteropancreatic neuroendocrine tumors and metastatic castration-resistant prostate cancers, respectively. However, these agents have also been used off-label, such as in neuroblastoma, pheochromocytoma, paraganglioma, and thyroid cancer patients. When faced with several failed therapeutic regimens and rapid progression of the disease, exploring alternative therapies such as radiopharmaceutical therapies may be an option. In a theranostic approach, the choice of the radiopharmaceutical used for treatment is important and will depend on the distribution of the disease and on uptake of the specific companion diagnostic agent.
CASE REPORT
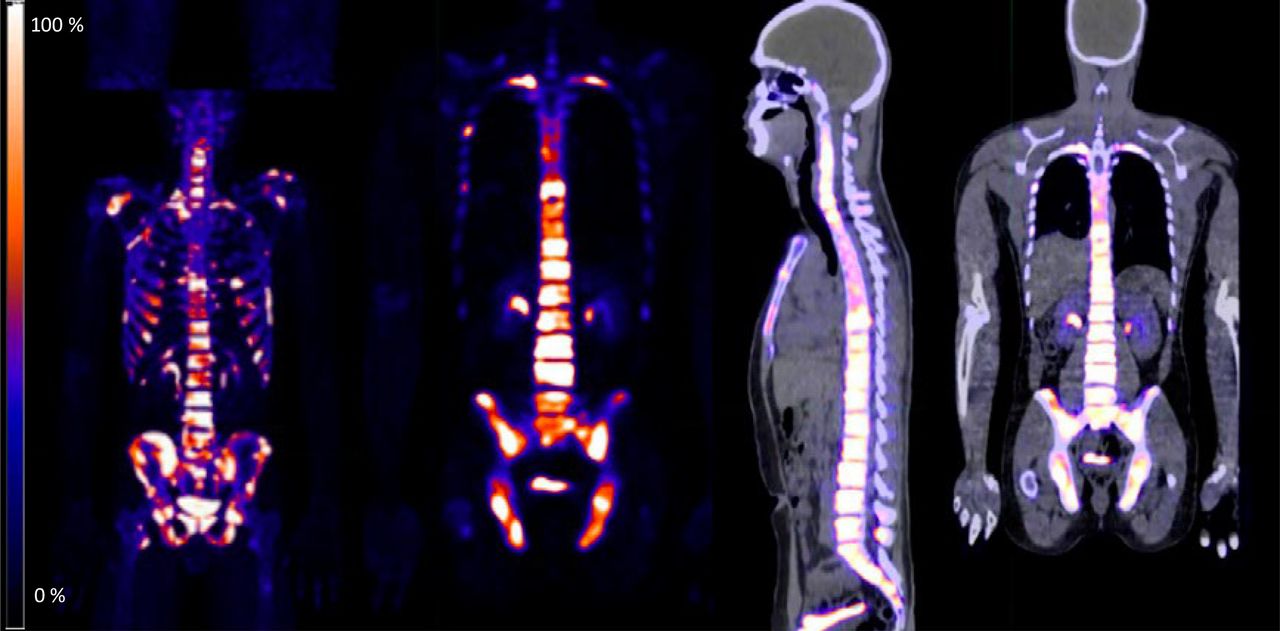
We present the case of a 36-y-old man who quickly progressed to advanced, stage IV, moderately differentiated lung adenocarcinoma with metastasis to the liver and bone. Initial staging CT scans on May 12, 2019, showed an irregular right-upper-lobe mass and a few small subcentimeter mediastinal lymph nodes. Biopsy revealed a moderately differentiated lung adenocarcinoma that was anaplastic large cell lymphoma–negative, had PD-L1 expression in 35% of the tumor, and had a next-generation sequencing EGFR mutation in exon 20 and a JAK mutation in exon 14. The initial staging 18F-FDG scan showed uptake in the primary right-upper-lobe lesion and mediastinal lymph nodes, with no distant metastases (Fig. 1). Brain MRI findings were unremarkable. Right upper lobectomy and mediastinal lymph node dissection were performed, revealing invasive adenocarcinoma, mainly of the acinar subtype, and micropapillary components; there was a grade 1, well-differentiated single tumor measuring 4.2 × 2.8 × 2.5 cm (R0). Spread of the tumor through air spaces was present. Visceral pleural invasion was also present, as well as extensive lymphovascular invasion. Twelve of 16 regional lymph nodes were involved, with extranodal extension. The patient at initial surgery had stage IIIA disease (T2b N2 M0). Surgery was followed by 4 cycles of adjuvant cisplatin/vinorelbine tartrate and adjuvant radiotherapy. About 1 mo after completion of adjuvant chemoradiation, the patient presented with generalized bone pain, and an 18F-fluoride PET scan showed widespread bony metastasis (Fig. 2). This rapid progression of disease required an inpatient hospital stay and several narcotics for pain control. These findings prompted consideration of palliation with radionuclide-based treatments and bone-seeking agents such as 153Sm, 89Sr, 186Re, 188Re, or even 223Ra. However, bearing in mind that the patient might also have additional soft-tissue disease, a 68Ga-DOTATATE scan was performed to assess whether the disease was predominantly in the bones or also in the soft tissues (Fig. 3). This scan showed mostly bony lesions, slightly less prominent than on the 18F-fluoride scan, and minimal uptake in the pleura, best appreciated retrospectively. Restaging 18F-FDG PET done within a few days showed not only bony disease but also right-sided pleural disease and fewer than 5 subcentimeter liver deposits, also not appreciated on the 68Ga-DOTATATE scan (Fig. 4). The progression of disease and molecular characterization are summarized in Figure 5.

18F-FDG PET/CT scan. Initial staging showing intensely 18F-FDG–avid right-upper-lobe mass with additional 18F-FDG–avid mediastinal lymph nodes. From right to left maximum-intensity-projection PET, coronal PET, coronal PET/CT, and axial PET/CT images.
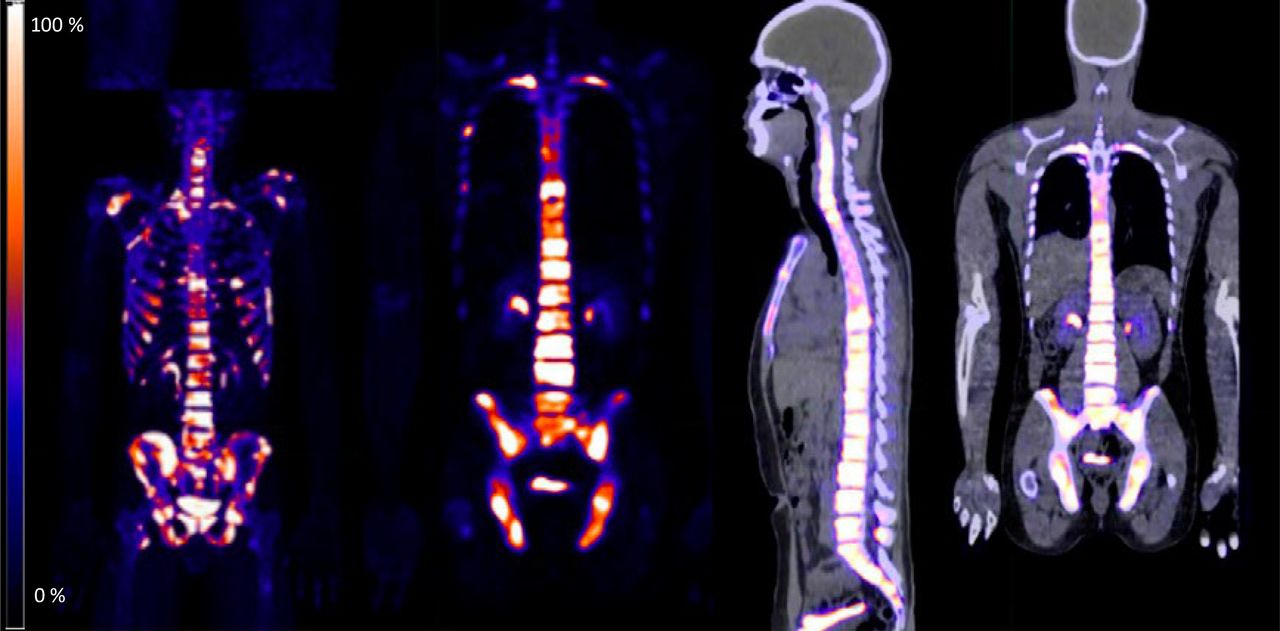
18F-fluoride PET/CT scan. Diffuse bony metastasis with intense 18F-fluoride uptake is seen. From right to left maximum-intensity-projection PET, coronal PET, sagittal PET/CT, and coronal PET/CT images.

68Ga-DOTATATE PET/CT scan. Diffuse bony metastasis is noted; uptake of 68Ga-DOTATATE is less prominent than that of 18F-fluoride in Figure 2. Liver and pleural involvement seen on subsequent 18F-FDG scan 1 wk later is not clearly appreciated with 68Ga-DOTATATE. From right to left maximum-intensity-projection PET, coronal PET, sagittal PET/CT, and coronal PET/CT images.
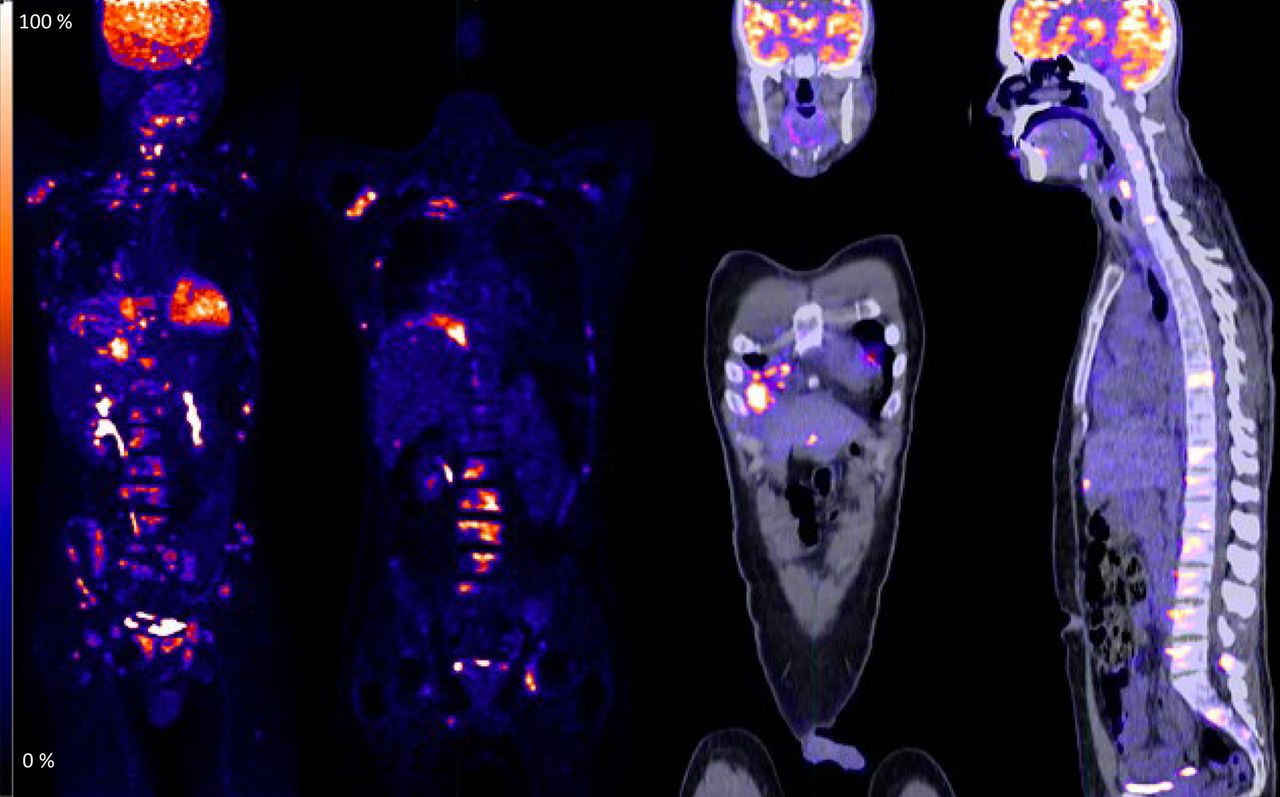
18F-FDG PET scan showing diffuse bony lesions but also detecting pleural and very minimal subtle liver disease not visualized on 68Ga-DOTATATE scan. From right to left maximum-intensity-projection PET, coronal PET, coronal PET/CT, and sagittal PET/CT images.
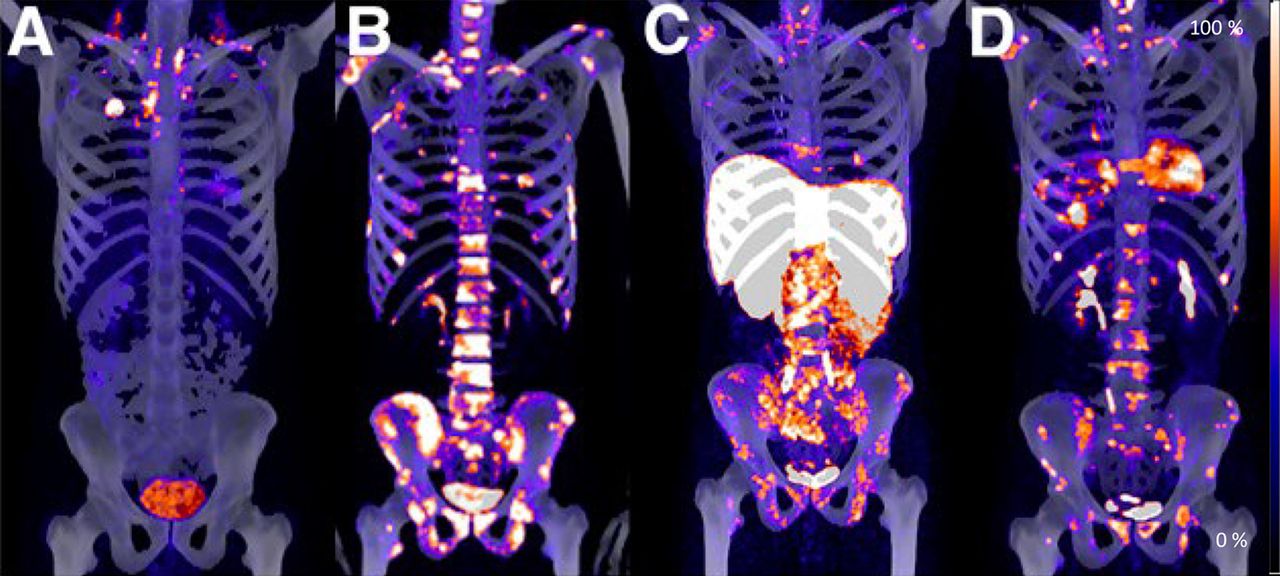
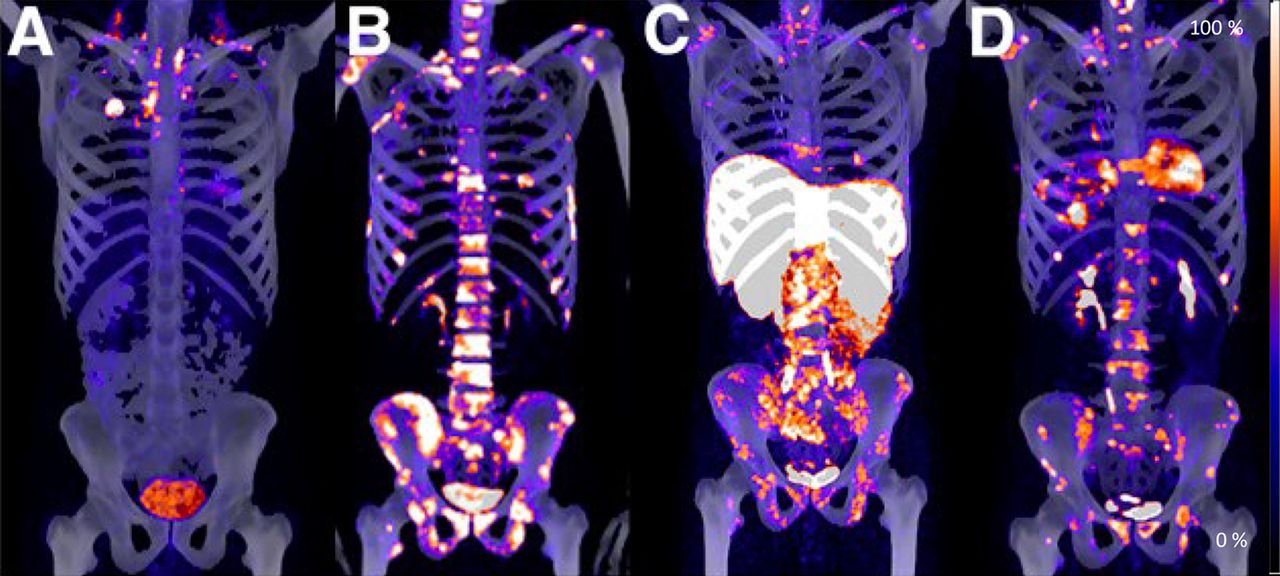
(A) Initial staging 18F-FDG PET/CT scan. (B) Seven months later, 18F-fluoride PET/CT scan shows diffuse bony metastasis. (C) Additional 68Ga-DOTATATE PET/CT scan 2 wk later shows bony lesions less prominently than on 18F-fluoride scan, somewhat similar to follow-up 18F-FDG PET/CT scan. (D) Follow-up 18F-FDG PET/CT scan 1 wk later shows bony lesions and pleural and liver disease.
DISCUSSION
223Ra, an α-emitter selectively targeting bone metastasis, improved overall survival in the ALSYMPCA trial in castration-resistant metastatic prostate cancer (7,8). 177Lu-DOTATATE, a β-emitter, also improved overall survival, progression-free survival, and quality of life in patients with midgut neuroendocrine tumors from the NETTER-1 study (9). Although radiopharmaceutical therapies are seldom used in lung cancer, there is a growing interest in use in a variety of cancers. 177Lu-DOTATATE–based radiopharmaceutical therapies were also shown to improve overall and progression-free survival in bronchopulmonary carcinoids (10–13). Reports have also discussed the 177Lu-DOTATATE treatment paradigm in small cell lung cancer (14–17). Additionally, some reports and clinical trials are evaluating the benefit of 223Ra in non–small cell lung cancer (18–20). One of the prerequisites for 177Lu treatment is somatostatin receptor expression demonstrated on a companion diagnostic 177Lu-DOTATATE PET scan such as in our case. Positive bone scan results are the companion diagnostic for 223Ra. 18F-fluoride and 177Lu-DOTATATE PET scans offer a road map to assess the eligibility of a patient for a therapeutic option. This, of course, is currently limited to situations in which all conventional treatments have been exhausted. In our patient, we considered palliative treatment with radiopharmaceutical therapies with bone-seeking agents such as 153Sm, 89Sr, or even 223Ra. 177Lu-DOTATATE treatment was considered within a theranostic approach in the context of the patient’s also having some soft-tissue disease in the pleura and liver. Bone-seeking radiopharmaceuticals may be preferred in bone-predominant disease, and 177Lu-DOTATATE–based therapeutic radiopharmaceuticals may be preferred for non–bone-predominant disease. After declining any additional chemotherapy or immunotherapy and complete molecular characterization of the patient’s disease with PET, the patient then traveled to his home country and passed away shortly thereafter.
CONCLUSION
Considering that lung cancer patients frequently have a poor prognosis, radiopharmaceutical therapies should be kept in mind even if only for palliation of disease. In the era of theranostics, it becomes feasible to assess targets by pretherapy imaging such as, in our patient, with 18F-fluoride and 68Ga-DOTATATE. Further studies and clinical trials are needed for validation in lung cancer and other types of cancer.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online March 15, 2021.
REFERENCES
- Received for publication October 11, 2020.
- Accepted for publication January 27, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}