


Abstract
Modifications of the biodistribution of 99mTc-sestamibi seen during myocardial perfusion and parathyroid imaging may be secondary to benign or malignant processes in visualized anatomic structures not related to the target organs of these imaging procedures. This article presents a case of pancreatic adenocarcinoma indirectly depicted on parathyroid scintigraphy.
99mThe radiopharmaceutical 99mTc-sestamibi has physiologic biliary excretion during scintigraphic evaluation of the parathyroid and the myocardium. Biliary and gallbladder incidental findings have been reported during these 2 main imaging applications of this radiotracer. This article presents a case of an indirect incidental demonstration of pancreatic cancer with the presence of distended intra- and extrabiliary ducts on parathyroid scintigraphy.
CASE REPORT
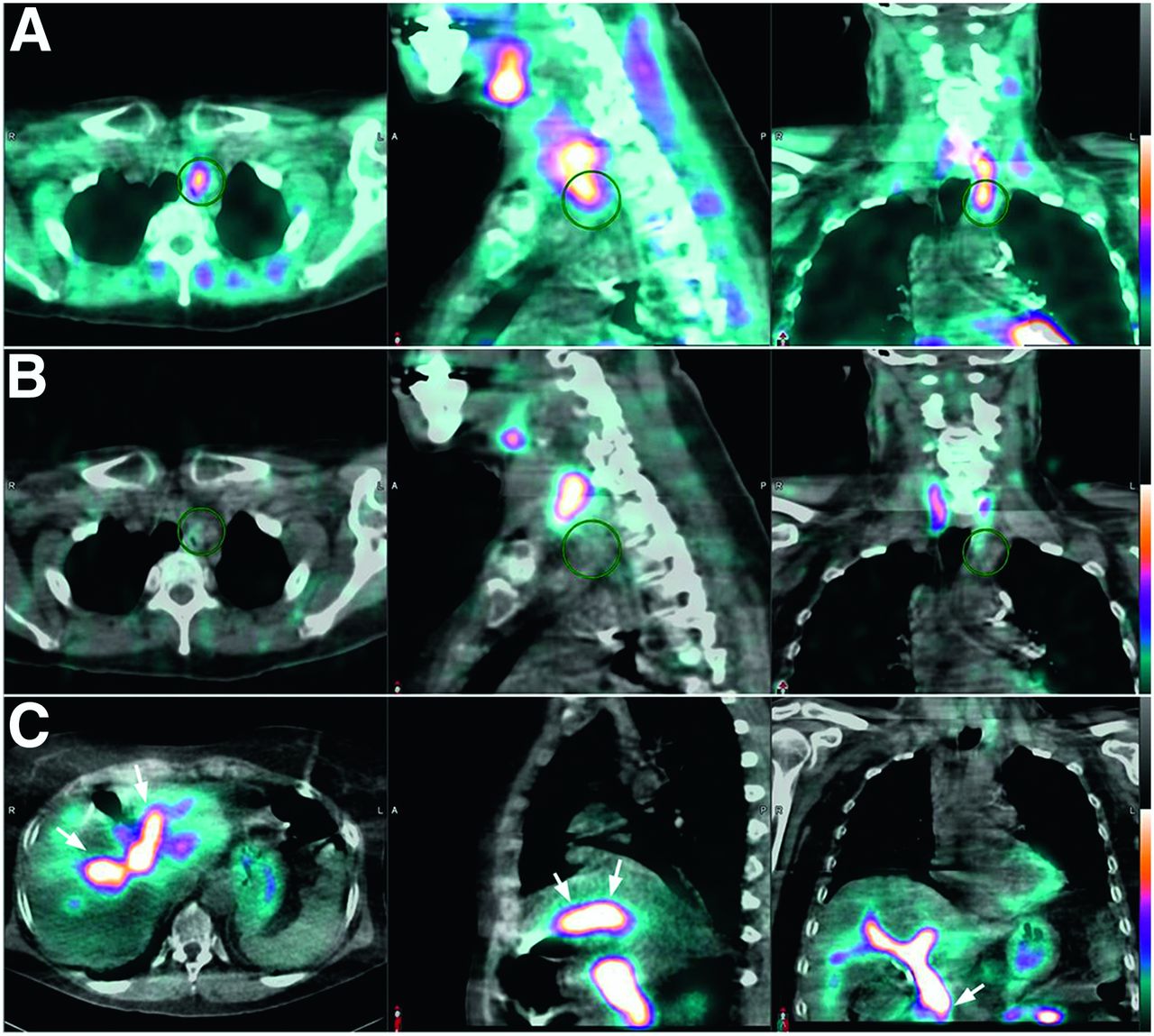
A 67-y-old woman consulted our institution because of primary hyperparathyroidism. Dual-radiotracer parathyroid scintigraphy was performed with 9.25 MBq (250 μCi) of 123I-sodium iodide, given orally as a capsule, and 925 MBq (25 mCi) of 99mTc-sestamibi intravenously. Double-isotope pinhole imaging with subtraction and SPECT/CT were performed. The SPECT/CT was done about 40–60 min after the tracer injection, using a Philips Brightview XCT camera with a low-energy high-resolution collimator, a 128 × 128 matrix, and 128 angles of rotation with 20 s per angle. The images showed a parathyroid adenoma at the left superior mediastinum near the thoracic inlet (Figs. 1A and 1B). In addition, the exam showed, at the right upper abdomen, prominent activity in the biliary ducts, with a cutoff sign at the distal common bile duct (Fig. 1C). The gallbladder was not seen because the patient had previously undergone cholecystectomy.

Axial, sagittal, and coronal SPECT/CT images of parathyroid scintigraphy showed parathyroid adenoma in left superior mediastinum positive for 99mTc-sestamibi uptake (A, circles) and negative for 123I-sodium iodide uptake (B, circles). SPECT/CT also showed prominent tracer activity in intra- and extrahepatic biliary ducts, with cutoff sign at distal common bile duct suggestive of obstruction (C, arrows).
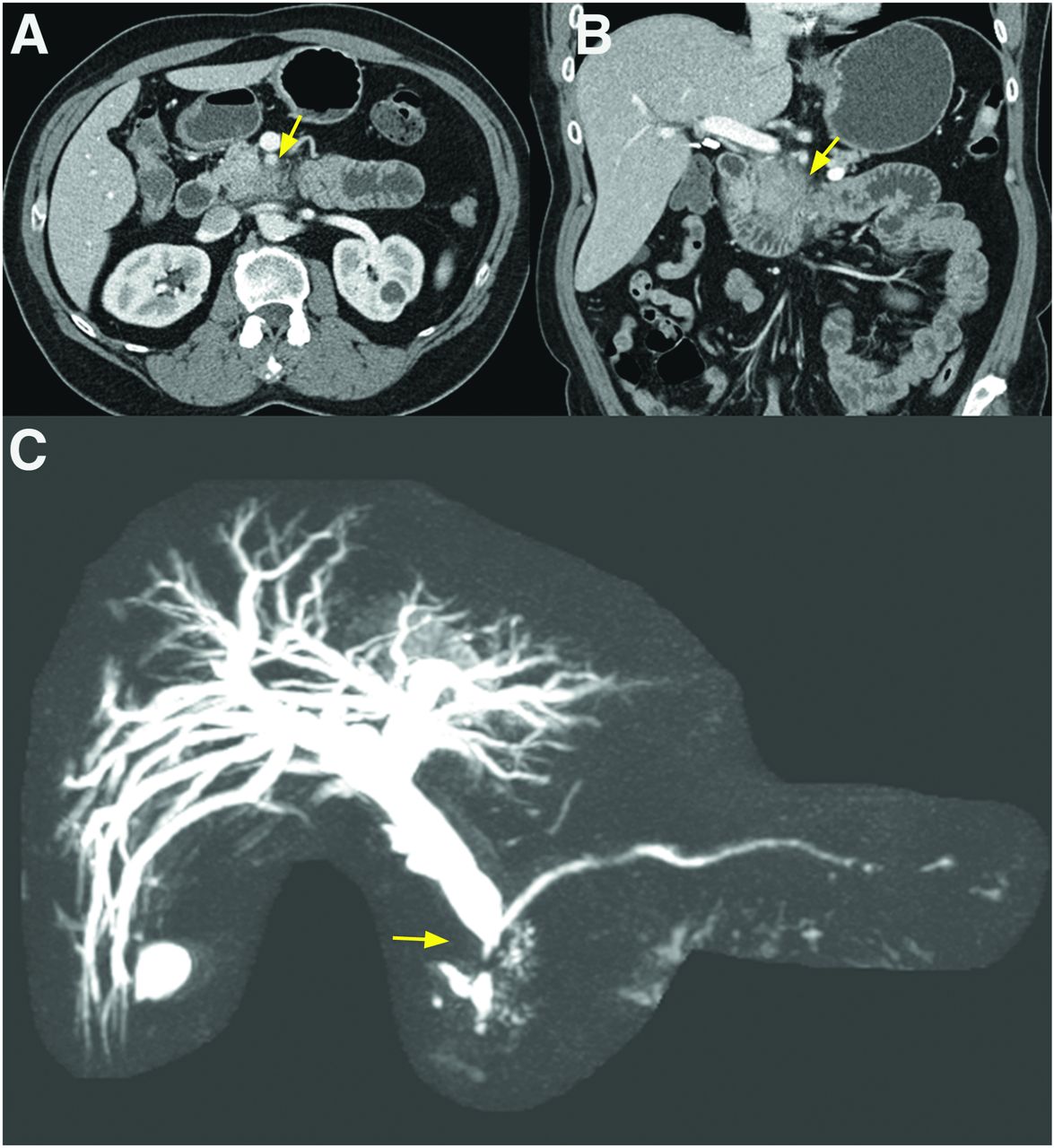
Review of the clinical notes revealed a recent history of progressively worsening pain in the back and abdomen, for which she had undergone abdominal CT, with normal findings, at an outside institution 2 mo before the present consultation. On the basis of the scintigraphic biliary findings, that previous CT scan was obtained, reviewed again, and found to show a soft-tissue mass in the region of the head and uncinate process of the pancreas (Figs. 2A and 2B). At the time of that CT exam, the patient had a vague abdominal pain but no laboratory or CT findings of biliary or pancreatic ductal obstruction.
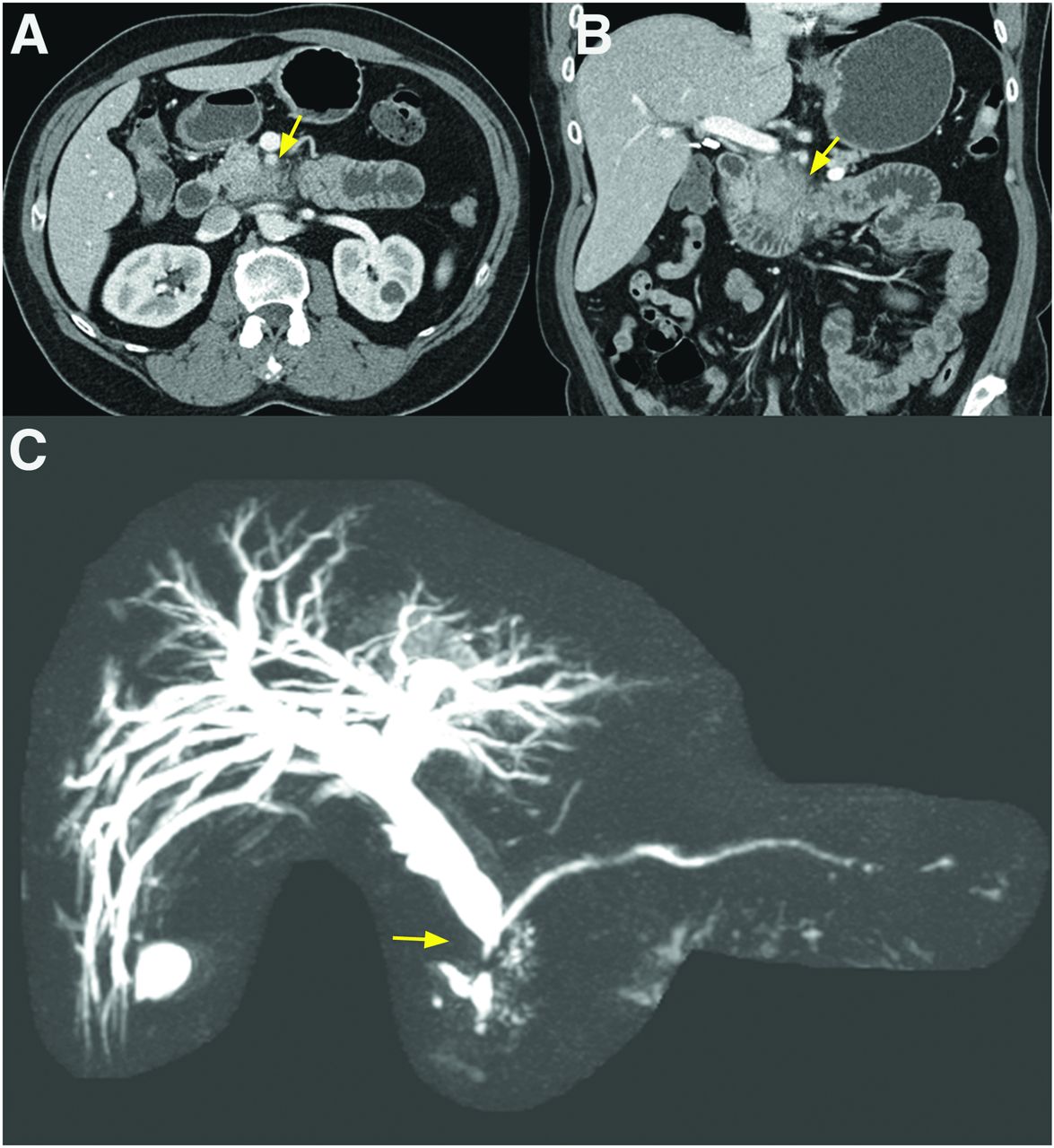
Review of prior CT exam, performed 2 mo before parathyroid scan, showed soft-tissue fullness of head and uncinate process of pancreas suggestive of malignancy (A and B, arrows). MR cholangiography, after parathyroid scan, confirmed dilated biliary ducts from progressing unresectable adenocarcinoma at head of pancreas, with cutoff sign at distal common bile duct (C, arrow).
Subsequent MRI and MR cholangiography showed an unresectable pancreatic mass with compression of the distal common bile duct and tumor encasement of the superior mesenteric artery, the replaced right hepatic artery, and the superior mesenteric vein (Fig. 2C). An MRI exam followed by an endosonographic evaluation staged the pancreatic cancer as T4 Nx Mx. Endoscopic tissue sampling confirmed the diagnosis to be pancreatic adenocarcinoma.
Because of the aggressiveness of the pancreatic adenocarcinoma and the patient’s rapid clinical deterioration, parathyroidectomy was postponed. Twenty-two months after the initial CT exam, the patient died from complicated biliary and gastrointestinal tract obstruction along with widespread bilateral pulmonary metastasis.
DISCUSSION
99mTc-sestamibi is the workhorse radiopharmaceutical for myocardial perfusion imaging and for scintigraphic evaluation of hyperparathyroidism. These 2 procedures include planar, SPECT, or SPECT/CT imaging with a field of view that includes part of the chest and upper abdomen. The radiotracer biodistribution in thoracic and abdominal organs visualized during these procedures may provide important information about coexisting diseases potentially impacting patient care (1–3). 99mTc-sestamibi physiologic uptake is usually homogeneously diffuse in the hepatic parenchyma, often with prominent activity in the gallbladder (4). In our case, the unusually conspicuous intra- and extrabiliary ducts on scintigraphy, with distal common bile duct interruption, led to retrospective detection of an overlooked pancreatic lesion and subsequent diagnosis of an unresectable pancreatic adenocarcinoma.
CONCLUSION
Thorough evaluation of planar, SPECT, and SPECT/CT images of myocardial perfusion and the parathyroid is useful in detecting extracardiac and extracervical pathologic processes.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 24, 2020.
- Received for publication May 1, 2020.
- Accepted for publication September 18, 2020.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.