


Abstract
Pelvic lymphatic leakage and lower extremity lymphedema are well-known complications of pelvic surgery or radiation therapy. We report a cervical carcinoma patient who, after hysterectomy and lymphadenectomy, developed concomitant lymphedema of the left lower extremity and a pelvic lymphatic leak identified on lymphoscintigraphy and SPECT/CT.
Lower extremity lymphedema and pelvic lymphatic ascites are well-recognized complications of pelvic surgical procedures, commonly secondary to lymphadenectomy in the treatment of gynecologic malignancies (1,2). Noninvasive lymphoscintigraphy is an established imaging modality for characterization of extremity lymphedema. We report a patient with cervical carcinoma who, after radical hysterectomy, pelvic lymphadenectomy, and radiation therapy, presented with bilateral lower extremity swelling. 99mTc-labeled filtered sulfur colloid lymphoscintigraphy and SPECT/CT confirmed lower extremity lymphedema and concomitant pelvic lymphatic ascites.
CASE REPORT
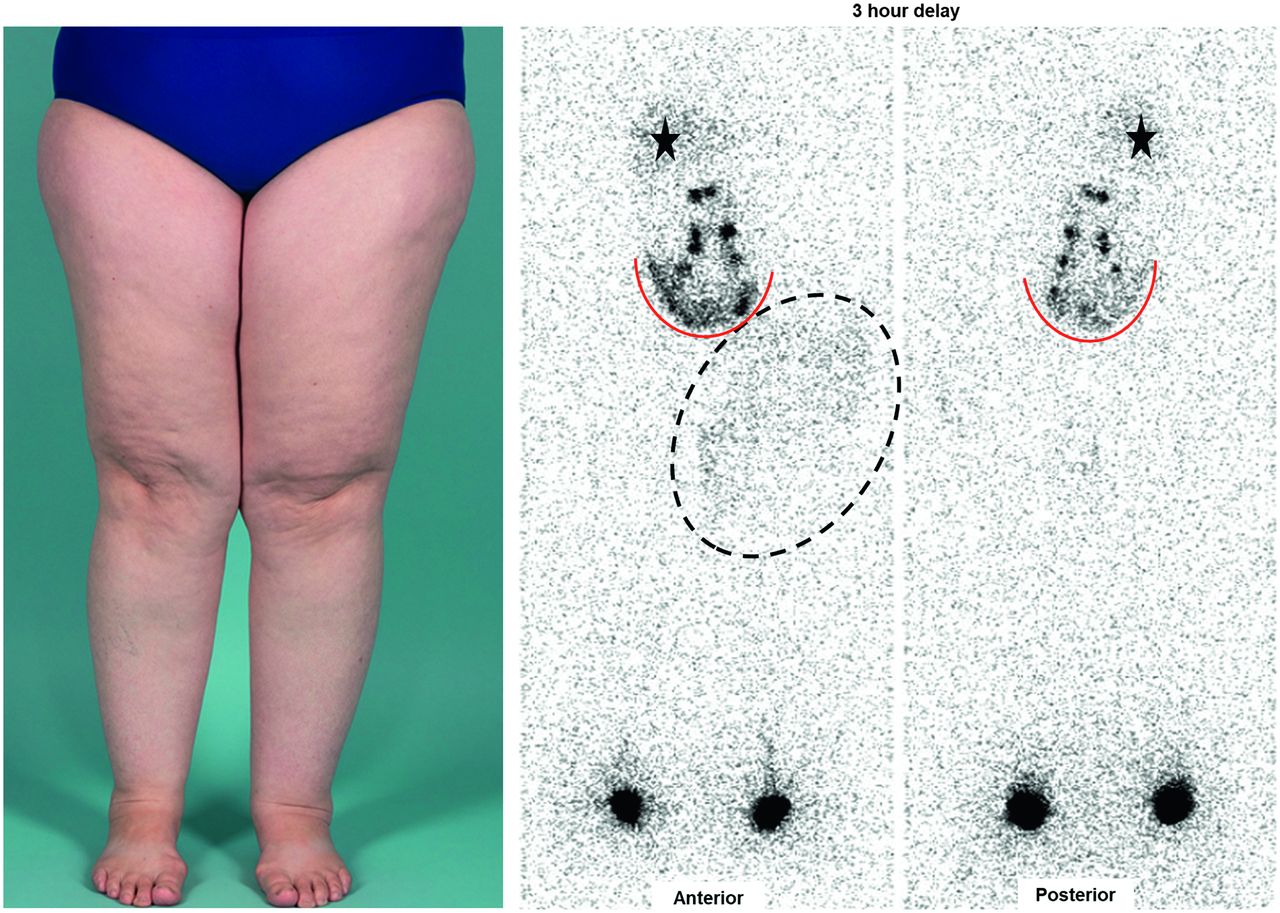
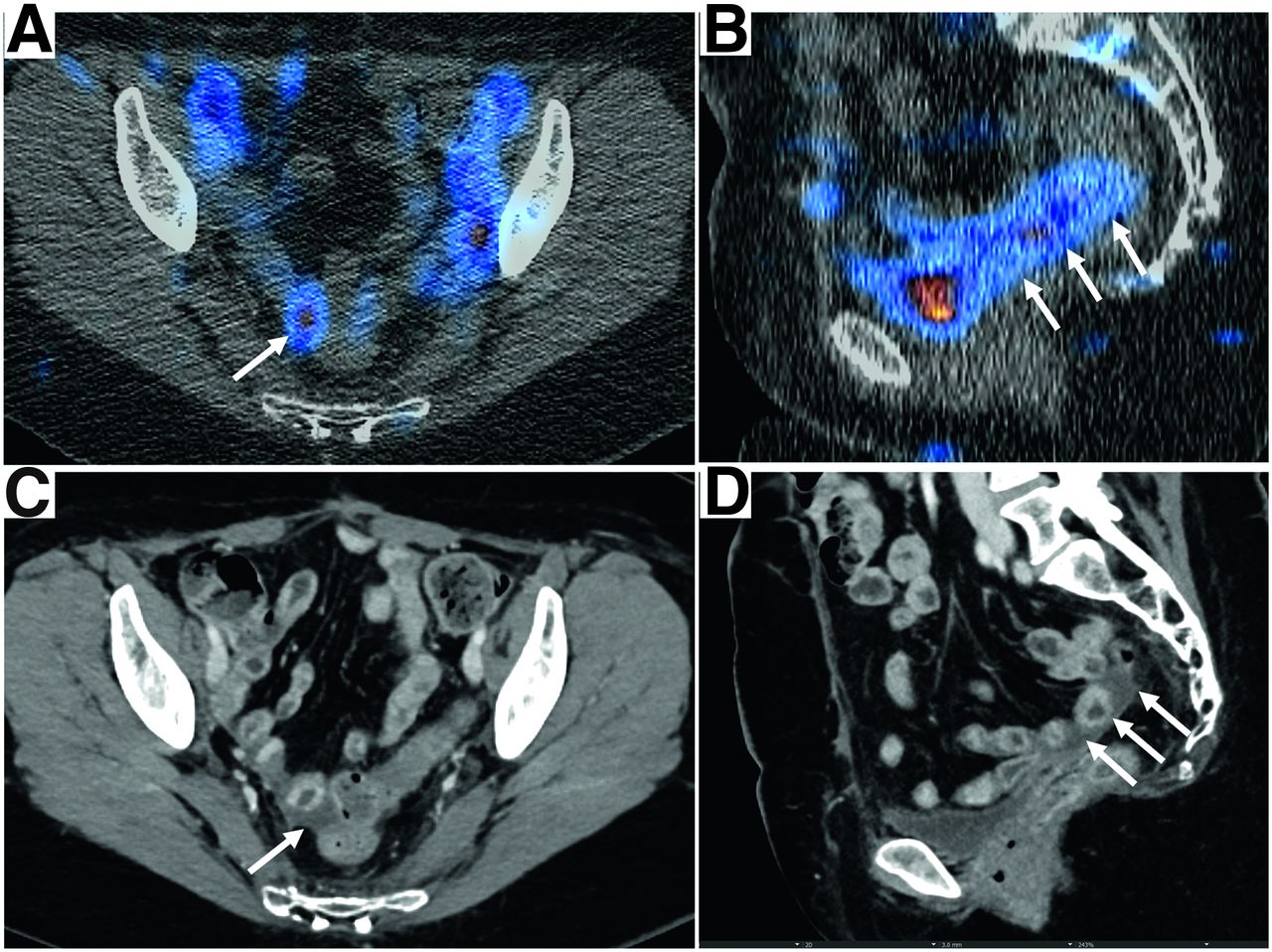
A 52-y-old woman with a history of cervical carcinoma after radical hysterectomy and pelvic lymphadenectomy with radiation therapy presented with bilateral lower extremity swelling. Physical examination revealed moderate nonpitting edema of the lower extremities, left greater than right, with associated dermal thickening, hyperkeratosis, and xerosis. Lower extremity lymphoscintigraphy was performed with subcutaneous injection of 18.5 MBq of 99mTc-labeled filtered sulfur colloid into the second web space of both feet. Planar images at 1 h after injection showed appropriate dynamic radiotracer drainage bilaterally to the ilioinguinal lymph nodes. Three-hour delayed planar images demonstrated dermal backflow in the left thigh, compatible with lymphedema. Incidentally, extranodal radiotracer distribution was noted in the pelvic floor, extending superiorly along the right pelvic sidewall and paracolic gutter (Fig. 1). SPECT/CT demonstrated abnormal extranodal radiotracer spreading in the dependent portion of the pelvis, which corresponded to a small volume of pelvic ascites on the diagnostic CT scan (Fig. 2.) A diagnosis of iatrogenic lymphedema of the left lower extremity with concomitant asymptotic pelvic lymphatic leakage was achieved.
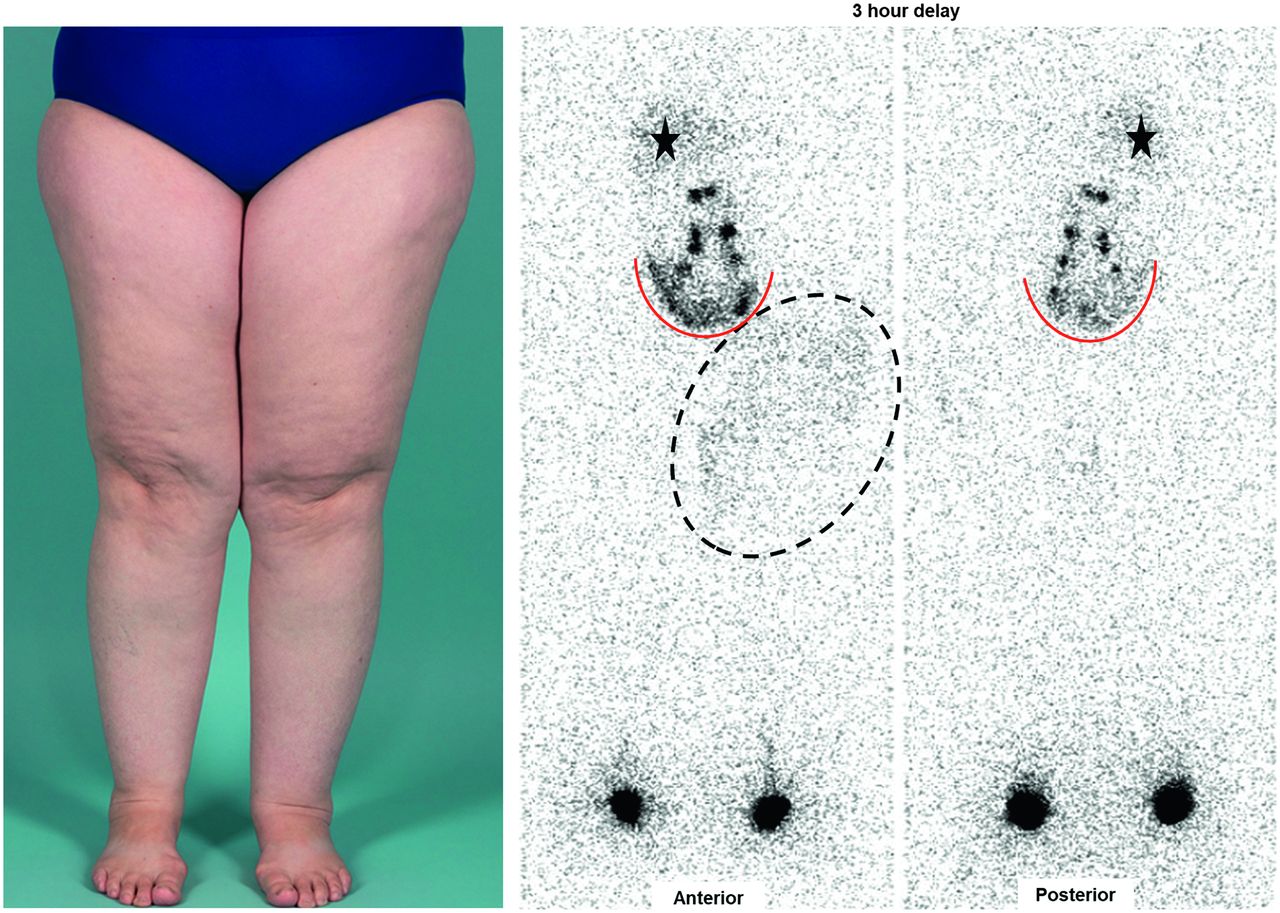
Photograph of lower extremities shows asymmetric swelling of left upper thigh. Three-hour delayed planar images show dermal backflow of left upper thigh, more prominent on anterior view (dashed outline). In addition, there is abnormal U-shaped extranodal radiotracer distribution in pelvis (red curves). Stars denote liver.

Axial (A) and sagittal (B) SPECT/CT images of pelvis demonstrate extranodal tracer distribution along pelvic floor (arrows) with corresponding free tracer fluid in pelvis on contrast-enhanced diagnostic CT images (C and D).
DISCUSSION
The reported incidence of lower extremity lymphedema secondary to treatment (surgery or radiation therapy) in gynecologic malignancy ranges from 10% to 49% (3,4). Lymphoscintigraphy has been adopted as the primary imaging modality in the detection of lymphedema. Despite the lack of standardized imaging protocols and poor spatial resolution, lymphoscintigraphy has demonstrated outstanding sensitivity and specificity in the diagnosis of lymphedema (5). Meanwhile, pelvic lymphatic ascites is an underrecognized complication after pelvic lymphadenectomy. The manifestation of pelvic lymphatic leakage ranges from trace, asymptomatic pelvic fluid to frank abdominal distention. It is usually a self-limited process and may require conservative management. Lymphoscintigraphy is superior to CT in characterization of lymphatic fluid in the pelvis. With advances in lymphedema treatment, it is imperative for nuclear radiologists to be familiar with diagnosis and staging of lymphedema to support appropriate clinical decision making.
CONCLUSION
Lymphoscintigraphy is a reliable, noninvasive imaging modality in diagnosis of extremity lymphedema and pelvic lymphatic leakage.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 24, 2020.
REFERENCES
- Received for publication September 18, 2020.
- Accepted for publication November 9, 2020.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.