


Abstract
Radioactive iodine (RAI) therapy with 131I is the standard of care for treatment in many patients with differentiated thyroid cancer. Because 131I is typically administered as a pill, and much of its radioactivity is excreted via the urine, there can be challenges in patients who cannot swallow pills, absorb iodine via the gastrointestinal tract, or eliminate RAI via the urine (i.e., dialysis patients and patients with renal failure). In this article, we present 3 cases in which the standard 131I treatment protocol for thyroid cancer could not be used because of these challenges, and we discuss the strategies used to overcome them. Provider collaboration and treatment customization are critical in overcoming patient-specific challenges.
Radioactive iodine (RAI) is considered a key treatment modality for hyperthyroidism and differentiated metastatic thyroid cancer; its use for these conditions was first documented in 1946 (1). 131I is used to treat Graves disease (therapeutic dose, 370–555 MBq [10–15 mCi]), toxic multinodular goiter (therapeutic dose, 555–1,110 MBq [15–30 mCi]), and thyroid cancer (therapeutic dose, 1,110 MBq [30 mCi] or more) (2–4).
With a half-life of 8.02 d, 131I emits γ-rays and β-particles, the latter causing localized therapeutic destruction of thyroid tissue (5). The γ-rays emitted by 131I pass through body tissues and can therefore be valuable for diagnostic imaging (5). Together, these properties make administration of 131I a useful adjunctive therapy for hyperthyroid disorders and thyroid cancer. In view of the marked increase in the incidence of thyroid cancer over the past several decades, the use of RAI as a supplementary treatment is likely to remain important (6). In general, 131I is administered as a pill and much of the administered activity is excreted in the urine. Although these administration and excretion routes are generally not an issue for most patients, there are exceptions, such as in patients who cannot swallow pills or absorb the administered dose or in patients undergoing dialysis, in which the normal urinary elimination is not possible. In this article, we present 3 cases in which the standard treatment protocol was not possible because of these challenges, and we inform providers of some available options should they encounter similar cases.
CASE REPORT
Case 1
Case 1 was a boy with a past medical history of Noonan syndrome with dysphagia diagnosed at birth. At 4 y of age, the patient came to our institution with an enlarged right thyroid lobe and was diagnosed with multiple thyroid nodules on a neck ultrasound. The ultrasound demonstrated a diffusely abnormal thyroid gland with microcalcifications, and the right and left cervical lymph nodes were abnormally enlarged with suggestive microcalcifications. These findings were highly suspected of representing thyroid malignancy, and a fine-needle aspiration of the right thyroid nodule revealed papillary thyroid cancer. The following week, CT of the neck and chest with contrast medium was performed, finding a lobulated heterogeneous mass in the right thyroid gland and multiple suggestive lymph nodes (Fig. 1). The following month, a thyroidectomy was performed with radical neck dissection to remove the suggestive nodes. A pathology report of the thyroid described a 4.2-cm primary papillary thyroid cancer with positive margins. In addition, angioinvasion and perineural invasion were present. Fourteen positive lymph nodes were identified at right neck levels II, III, IV, and VB and at left levels IIb and III. A pathologic stage classification, based on the eighth edition of the AJCC Cancer Staging Manual (7), was determined to be at least pT3aN1b(cMx).
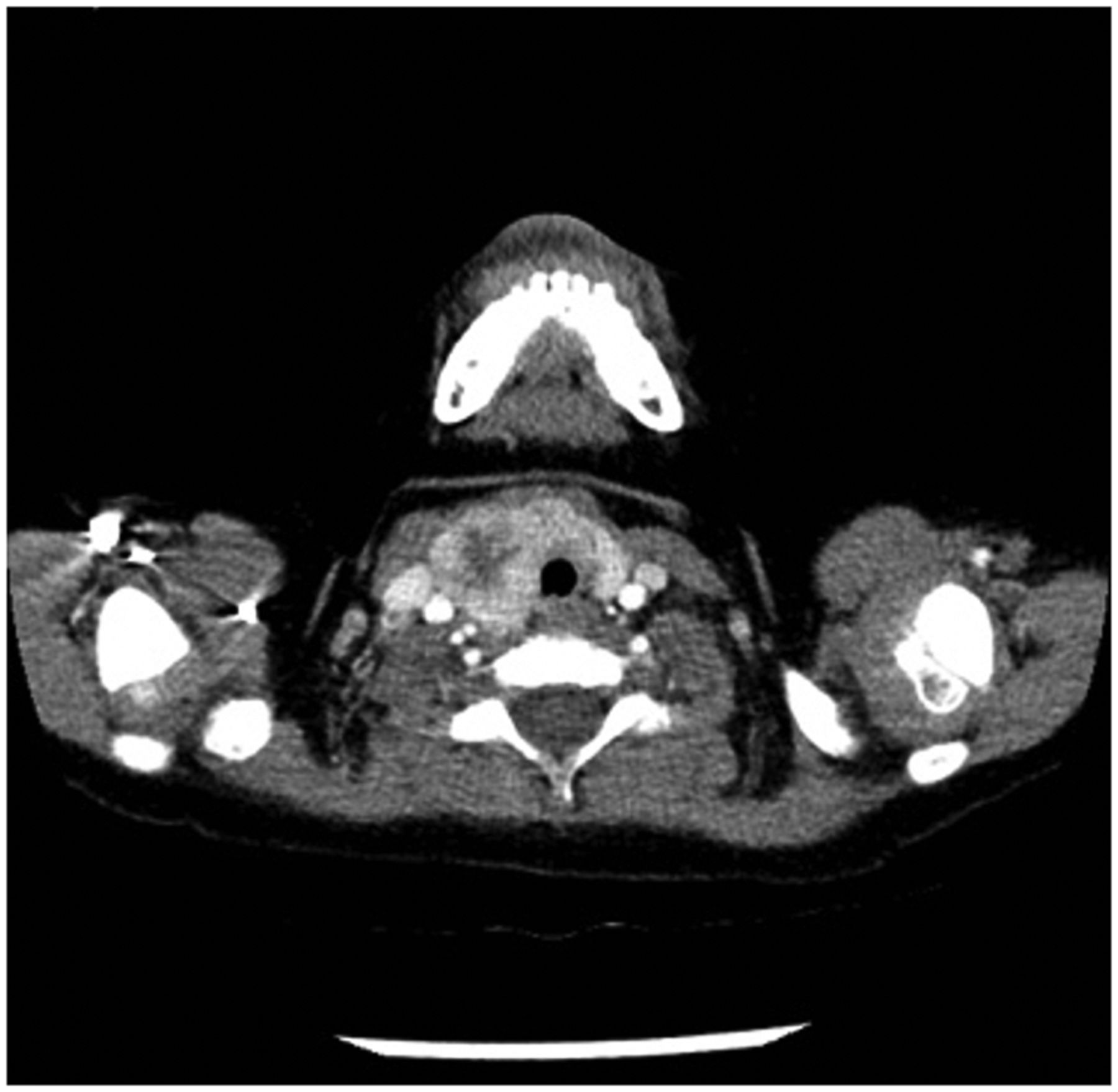
Case 1 CT scan. Axial CT demonstrates lobulated and heterogeneous 3.4 × 2.9 × 3.3 cm mass in right thyroid and extending into right superior paratracheal space. Abnormal right cervical and bilateral paratracheal lymph nodes and nonspecific 2-mm nodule in left lower lobe of lung were also seen. Findings were suggestive of thyroid cancer with cervical nodal metastases.
Given the patient’s intermediate-risk thyroid cancer, a recommendation was made for treatment with 131I. However, this case presented challenges due to the patient’s young age and difficulty swallowing. Because of the patient’s dysphagia, it was not feasible to administer the standard 131I pill orally. A multidisciplinary joint decision was made to proceed with liquid 131I therapy. Because the patient had extensive bilateral neck involvement on pathology, a pretherapy scan was recommended to assess for macroscopic residual disease burden.
Since 131I is volatile, liquid administration required special preparations. Specifically, to avoid staff exposure to 131I, a pharmacist provided a 5- to 10-mL oral solution of 131I mixed with grape juice in a French square glass vial with a screw cap. The patient drank through a straw with a spinal needle that was attached to poke the Teflon (DuPont) septum within the cap. These preparations were designed to minimize evaporation of liquid 131I. An anterior and posterior whole-body scan with SPECT/CT imaging of the neck was taken 24 h after oral administration of 55.5 MBq (1.5 mCi) of Na131I (123I was not available as a liquid for the diagnostic scan). Focal uptake was noted in the thyroid bed region in the neck, consistent with remnant thyroid tissue. There were no visible suggestive cervical or distant foci of RAI uptake to suggest metastasis.
The following day, the patient was admitted (as per the patient’s legal guardian’s request because of situations in the home) to our hospital for high-dose RAI therapy. For the therapeutic dose of 2,775 MBq (75 mCi) of Na131I in a liquid form, the dose was again mixed with grape juice and ingested via a method similar to that for the pretherapy scan.
The patient was discharged 2 d after being admitted and returned the following week for a posttherapy anterior and posterior whole-body scan supplemented by SPECT imaging of the neck (Fig. 2). A year after therapy, the patient received a follow-up neck ultrasound to evaluate the surgical bed. Postsurgical changes related to total thyroidectomy were observed, but no new suggestive soft-tissue nodules or lymph nodes were found. There were a few bilateral nonspecific soft-tissue nodules, but they were unchanged from his last ultrasound the previous year and were felt to represent postsurgical and posttreatment changes. The most recent lab results using an ultrasensitive thyroglobulin assay showed an expected very low level of thyroglobulin (0.6 μg/L; reference range, 1.4–29.2 μg/L) and undetectable thyroglobulin antibodies of less than 2.00 IU/mL.

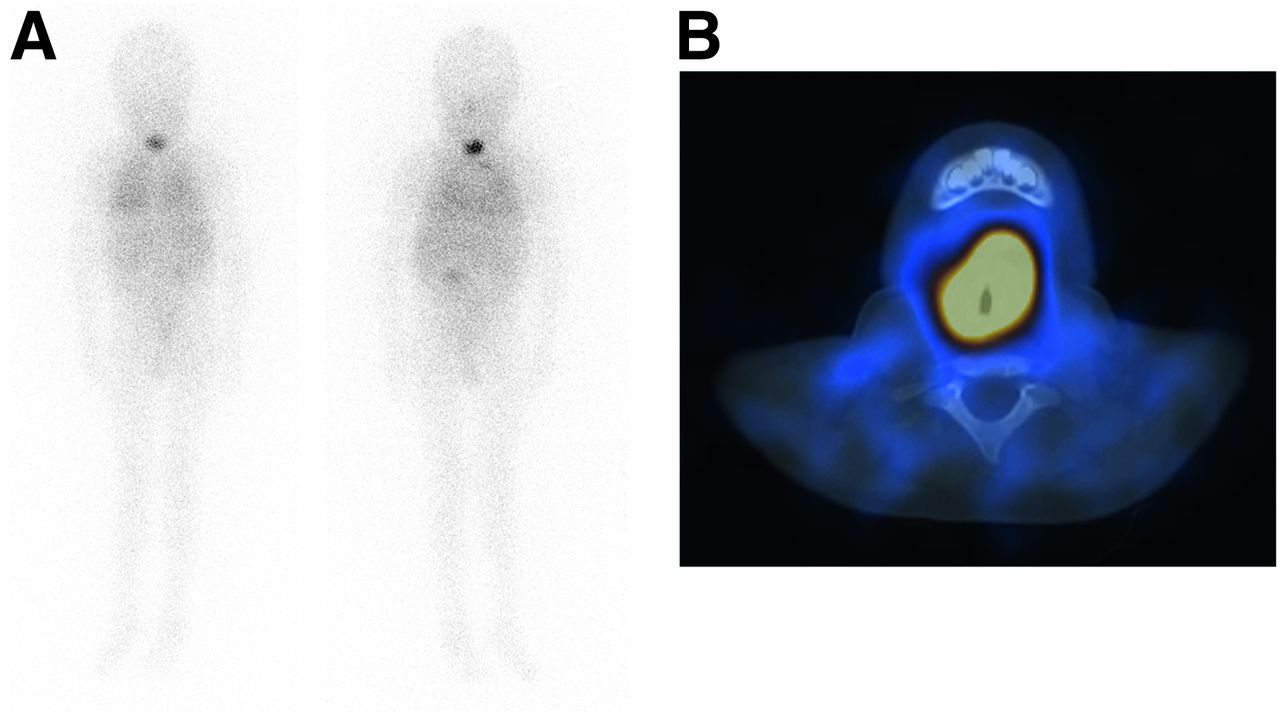
Case 1 posttherapy scan. (A) Whole-body scan obtained after administration of 2,775 MBq (75 mCi) of 131I. (B) SPECT imaging of neck. These images are consistent with residual thyroid tissue, as focal tracer uptake was noted within thyroid resection bed.
Case 2
Case 2 was a 45-y-old man with a medical history of scleroderma with severe gastric motility disorder. An ultrasound examination followed by fine-needle aspiration a year before treatment led to a diagnosis of papillary thyroid carcinoma. Imaging showed bilateral solid thyroid nodules with microcalcifications. Later that year, the patient underwent thyroidectomy with radical neck dissection. Features typical of papillary thyroid carcinoma, including papillary architecture, nuclear crowding, nuclear clearing, and nuclear-groove and intranuclear pseudoinclusions were observed in sections of both the right and the left thyroid lobes. In both lobes there were 2 foci, and the cancer was confined to the thyroid, with negative margins.
The patient was then referred to our service for RAI. A major challenge in this patient’s treatment was his history of scleroderma and his gastric motility and malabsorption disorder, precluding oral intake and requiring total parenteral nutrition. Because of these challenges, the risks of treatment with oral 131I in this patient included significant difficulties in absorbing the pill and a very high risk of reflux and vomiting. As a result, and per discussions with the patient’s treatment team, the decision was made to proceed with 131I therapy via intravenous administration.
However, unlike in case 1, the alternative method of administration in this case required a special dispensation from the state because the route was no longer oral. Therefore, a one-time request was placed to the Radiologic Health Branch of California for a dispensation to administer intravenous 131I, and the request was granted in April 2018. This request was an amendment to the license for a one-time intravenous use. In addition, a vendor had to be located to provide a sterile form for intravenous administration. The patient was pretreated with 2 daily intramuscular injections of 0.9 mg of thyrotropin alfa (Thyrogen; Genzyme Corp.). After state board approval, a 1,850-MBq (50 mCi) dose of Na131I was administered through an intravenous catheter. No immediate adverse events were observed.
Posttherapy whole-body SPECT/CT imaging of the neck the following week did not find any distant metastatic disease (Fig. 3). One year after treatment, neck ultrasound showed postsurgical findings from thyroidectomy and no new or suggestive findings. Thyroglobulin levels were 0.1 μg/L (nearly undetectable; reference range for intact thyroid, 2.8–40.9 μg/L) and thyroglobulin antibodies were 1 IU/mL (within the reference range of ≤1IU/mL).
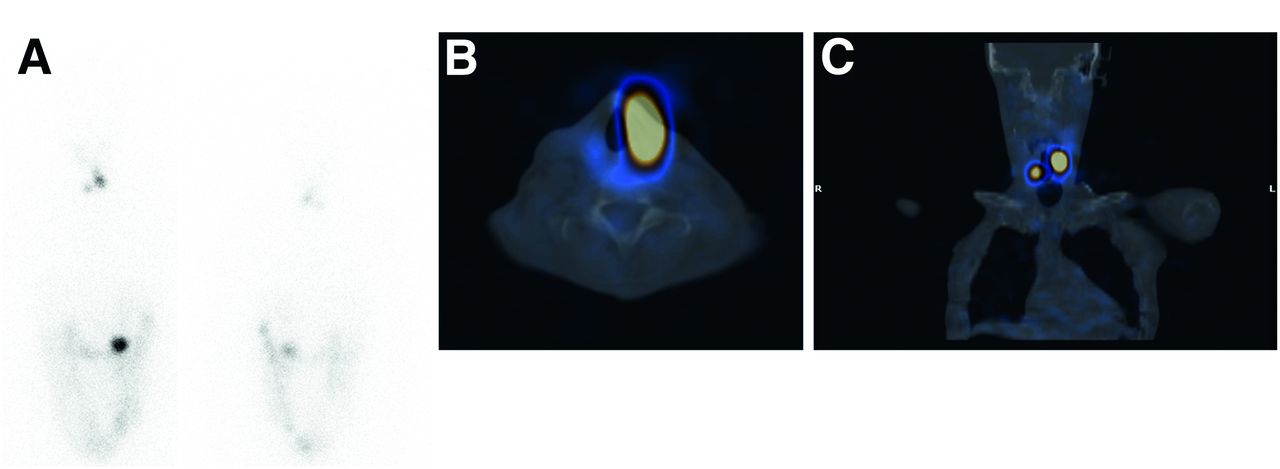
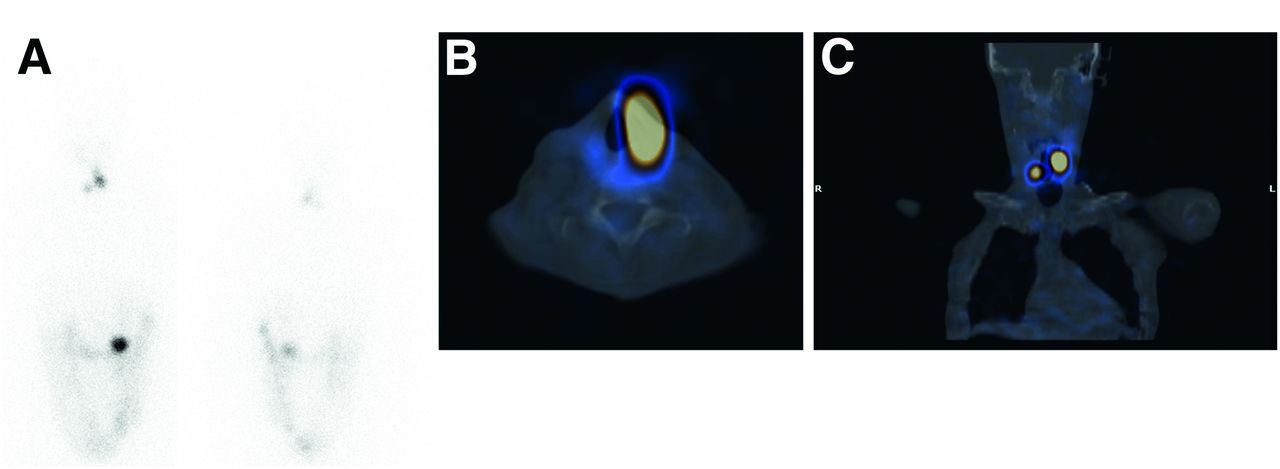
Case 2 post-RAI therapy scan with intravenous administration of 131I. (A) Whole-body scan obtained after administration of 1,850 MBq (50 mCi) of 131I. (B and C) SPECT/CT imaging of neck obtained in axial and coronal planes, respectively, showing focal tracer uptake in thyroid bed, consistent with residual thyroid tissue. No distant metastases were observed.
Case 3
Case 3 was a 59-y-old man with diabetes mellitus, hypertension, and end-stage renal disease on hemodialysis. One challenge with hemodialysis in the context of RAI treatment is ensuring radiation protection for everyone present, as there is a risk that the RAI will contaminate the dialysis machine and increase the level of occupational exposure. In addition to the contamination-control and occupational-exposure issues, there are concerns with waste-disposal, dosimetry, and patient-release issues. Finally, because the 131I is eliminated largely through the dialysate because of the negligible renal clearance, the administered dose might need to be modified from the typical protocol.
The patient was referred from outside our medical center for treatment with RAI after surgery for an 8-cm pT3aNx follicular thyroid cancer with capsular vascular invasion. The patient underwent a whole-body scan with 123I. Anterior and posterior images of the neck and entire body were taken 24 h after oral administration of 95.83 MBq (2.59 mCi) of Na123I. No distant uptake was found to suggest metastasis, and the focal uptake within the thyroid bed was consistent with residual thyroid tissue after recent thyroidectomy.
The hemodialysis requirement presented the challenge of providing radiation protection to those who would be caring for the patient during dialysis. Our workflow for managing this case is illustrated in Figure 4. Specifically, multidisciplinary meetings were held involving radiation safety, nuclear medicine, endocrinology, and nephrology personnel. The decision was made that the radiation safety team would monitor all personnel and equipment and check for contamination of the dialysis machines and ports. The training materials provided to the dialysis lab personnel are included in the supplemental materials (available at http://jnmt.snmjournals.org). Additionally, all dialysis staff received training from radiation safety personnel.

Workflow for management of patients with end-stage renal disease (ESRD) who are on dialysis and referred for RAI.
The following month, the patient received 1,102.6 MBq (29.8 mCi) of Na131I as a pill to treat his follicular thyroid cancer. After a discussion among health-care staff and consultation of the relevant literature, the dose had been lowered from an anticipated dose of 1,850 MBq (50 mCi) because of the use of dialysis, to reduce the radiation dose to the marrow secondary to the lowered clearance. The patient was admitted to our hospital at the University of California, San Francisco for this procedure.
The patient was prepared for therapy by thyroid hormone withdrawal. The outpatient dialysis record showed a normal session the day before the therapy, without any adverse events. After collaboration between the nuclear medicine team, the radiation safety team, the primary nephrologist, and the outpatient nephrologist, the patient received dialysis the day after the RAI therapy, with intermittent hemodialysis for 3.5 h planned for 3 consecutive days after RAI. The patient tolerated the intermittent hemodialysis well. The radiation safety personnel checked the dialysis machines and no contamination was detected. There were no complications or radiation risks after the careful planning.
The posttherapy 131I scan supplemented by SPECT/CT imaging of the neck found no evidence of distant metastatic disease (Fig. 5). Most recently, at 1 y 2 wk after the RAI therapy, the patient underwent anterior and posterior imaging of the neck and entire body without SPECT 24 h after oral administration of 82.88 MBq (2.24 mCi) of Na123I. No abnormal RAI uptake was observed to suggest recurrent or metastatic disease.

Case 3 posttherapy scan. (A) Whole-body post-131I scan. (B–D) Axial SPECT/CT of the lower neck and mid neck, and coronal SPECT/CT of the neck and chest. These images show no evidence of distant metastatic disease. However, they did find 3 discrete regions of tracer activity within neck, consistent with iodine-avid tissue, likely residual thyroid tissue after thyroidectomy.
DISCUSSION
At present, 131I pills are the standard preparation for RAI treatment of hyperthyroidism and thyroid cancer. von Schulthess et al. concluded that capsular 131I is a safe formulation for treatment of thyroid disease, demonstrating that the gastric radiation dose from 131I pills was high only locally and was below the level that would cause tissue necrosis (8). However, unique patient challenges, such as dysphagia, may limit or restrict safe administration of oral 131I in pill form. The patient in case 1 was unable to take pills because of developmental anomalies and a young age and was consequently administered liquid oral 131I. No adverse events took place, and the dose was administered safely without exposing the technologist staff to radiation.
Previous studies concerning 131I therapy describe administration difficulties and alternative treatment protocols similar to those discussed here (Table 1). Aside from difficulty swallowing pills, Aamri et al. reported pill-related issues such as a patient-caused radiation hazard, pill adherence to the container, and technologist mishandling of the substance (9). Halpern et al. suggested that formation of iodine–gelatin complexes in the gastrointestinal tract may reduce thyroidal uptake of capsular 131I relative to the liquid form (10). One proposed solution involved endoscopically depositing the solid 131I pill into the stomach—effectively minimizing risk of spillage, exposure, and incorrect administration (11). However, endoscopy is invasive and carries risks for the patient.
Other Studies on Liquid 131I Administration
Rini et al. commented on the greater-than-intended irradiative impact of encapsulated 131I—particularly when used as a diagnostic tracer—compared with liquid-form 131I (12). Using a pill-form 131I tracer, this group observed a mean diagnostic 131I uptake 14% lower than the corresponding therapeutic 131I uptake (44% vs. 58%), reflecting the higher uptake for a pill that delivers a therapeutic dose than for a pill that delivers a diagnostic dose. They concluded that in hyperthyroid patients treated with liquid 131I, compared with encapsulated 131I, uptake of diagnostic doses of liquid 131I better predicts uptake of therapeutic doses of liquid 131I (12). It is therefore recommended that health teams familiarize themselves with administrative techniques and safety for liquid and intravenous 131I. Although administration of 131I in pill form is the first option, it is important to remember that liquid administration remains a safe and effective alternative, provided appropriate radiation safety precautions are followed (3,13).
Unlike case 1, the patient in case 2 did not have dysphagia and could swallow but had significant gastrointestinal dysmotility, which often manifested as episodes of pseudoobstruction with gastroparesis. Therefore, the patient was largely dependent on total parental nutrition, and oral or gastrotomy tube treatment was precluded. The decision to use intravenous treatment was made after months of ongoing discussion. The advantages of intravenous treatment relative to oral 131I therapy include enhanced diagnostic accuracy, rapidity, and the ability to treat patients with impaired gastrointestinal absorption (14). The risks include the liquid iodine’s volatility, which makes it more dangerous to handle and increases the risk of major spills and exposure of technologists to radiation. Meticulous care was undertaken, and no spills or other adverse event took place.
Patients are more prone to experience nausea as the 131I dose increases (15,16). Additionally, patients with gastroesophageal reflux disease, gastroparesis, gastric outlet obstruction, and other similar conditions are at increased risk of vomiting (16). Overall, case 2 demonstrated that intravenous administration of 131I is a safe and effective alternative when there is great difficulty with oral administration and gastrointestinal absorption is anticipated.
Case 3 evidenced an instance of end-stage renal disease complicating RAI treatment for follicular thyroid cancer. In patients with normal renal function, the 131I would be excreted through the urinary system; thus, impaired renal function complicates iodine clearance and theoretically potentiates blood radioactivity risks. Although the dialysis machine would likely compensate to some extent for this decreased clearance, hemodialysis patients are still impacted by decreased clearance of 131I (17). In addition, there is a risk that the dialysis staff and machinery will become contaminated (17). In fact, the main challenge with case 3 was in dealing with the radioactive dialysate waste, managing staff exposure, and training the staff. Contingency plans are necessary for addressing fluid spills during dialysis (18). Murcutt et al. supplied an illustrated schematic and protocol for safe hemodialysis of patients in need of ablative 131I RAI therapy, much of which mirrors the methods described here (19). Additionally, under dosimetry guidance, high-dose intravenous treatment of differentiated thyroid cancer patients is safe and may also reduce the radiation dose (20). To limit risks of bone marrow toxicity and further renal insult, therapy doses should not exceed the prescribed amount in any patient, including those patients on dialysis, as Magné et al. have recommended (21). Table 2 describes other instances of successful oral 131I administration in patients with end-stage renal disease on hemodialysis.
Other Studies on Oral 131I Administration for Dialysis Patients
Prior studies have suggested that dialysis patients have increased systemic retention of 131I, and reductions in the administered 131I dose have therefore been suggested, although no uniform consensus exists. Citing rapid iodine clearance, Morrish et al. concluded that dialysis reduces the effective radiation dose and necessitates larger 131I treatment doses to achieve outcomes equivalent to those in patients with normal renal function (22). Jiménez et al. administered to hemodialysis patients the same 131I doses as are received by patients with normal renal function. In their small cohort (n = 3), this protocol avoided overexposure of patients to radiation (23). Alevizaki et al. used a 40%–50% activity reduction of 131I and found that none of their patients experienced short-term side effects or had detectable thyroglobulin levels on their first posttherapy evaluation (n = 5; the inclusion criterion was end-stage renal disease) (24). Vermandel et al. concluded that an approximately 30% reduction from the nominal 131I dose struck the best balance between hematologic toxicity and treatment efficacy (n = 6; the inclusion criterion was end-stage renal disease undergoing hemodialysis) (25). Following their lead, we chose to reduce the dose despite the fact that some of the literature recommended no change in, or even increased, doses; our case involved a 40% reduction from our typical 1,850 MBq (50 mCi) to 1,110 MBq (30 mCi) to minimize radiation exposure of marrow secondary to reduced clearance of 131I.
CONCLUSION
131I is a common treatment for hyperthyroidism and thyroid cancer, and most patients may be treated using standardized protocols as defined by the Society of Nuclear Medicine and Molecular Imaging (13). We have presented 3 cases that created technical difficulties for nuclear medicine and radiation safety staff, who had to come up with alternative protocols to meet each specific challenge. Knowledge of these alternatives should be of particular value to nuclear medicine technologists and physicians who encounter similar cases. The cases we have described highlight the importance of provider collaboration and treatment customization to overcome patient-specific challenges.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 20, 2020.
REFERENCES
- Received for publication August 12, 2020.
- Accepted for publication September 24, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}