


Abstract
Assessment of residual activity is critical for quality assurance after 90Y radioembolization. The resin microsphere manufacturer’s indirect method of estimating the residual activity is laborious and vulnerable to inaccuracies. Furthermore, the method cannot localize the exact site of residual activity. 90Y PET/CT for qualitative and quantitative assessment of residual activity has not, to our knowledge, been described. We show an example of 90Y PET/CT of residual activity in the delivery apparatus and catheters packed inside the delivery box. Focally intense residual activity was clearly localized to the stopcock junction. Residual activity was directly quantified by setting the PET volume-of-interest isocontour threshold to 1%.
Radioembolization using 90Y-labeled resin microspheres (SIR-Spheres; Sirtex Medical Ltd.) is a treatment modality for inoperable hypervascular liver tumors. After radioembolization, measurement of residual activity within the delivery apparatus is critical for quality assurance and training. The presence of significant residual activity (generally > 5% of prescribed activity) should trigger a procedural audit.
The manufacturer of resin microspheres has devised a method of indirectly estimating the residual activity based on relative count rates. The prepared v-vial of known activity is first placed into a standard cylindric acrylic glass container. Using a dose-rate meter at a fixed 30-cm distance, its dose rate is averaged from 4 positions around the container. After radioembolization, all delivery apparatuses and catheters are packed into the same container and the entire process repeated. The residual activity is then calculated from the percentage difference in count rates.
This method is simple, albeit laborious and vulnerable to inaccuracies. Inaccuracies may occur because of variations in geometry and positioning of items within the container, effects of self-absorption, probe directionality, and backscattering (1). There is also radiation exposure from additional manual handing. Furthermore, this method can determine whether significant residual activity is present but cannot localize the culprit. Localizing the culprit is critical to providing specific and relevant feedback to the operators involved.
In recent years, postradioembolization 90Y PET/CT of minuscule internal pair production has been shown to be clinically useful for the qualitative and quantitative assessment of target and nontarget microsphere biodistribution (2–4). However, its use for residual activity assessment has not, to our knowledge, been described to date.
MATERIALS AND METHODS
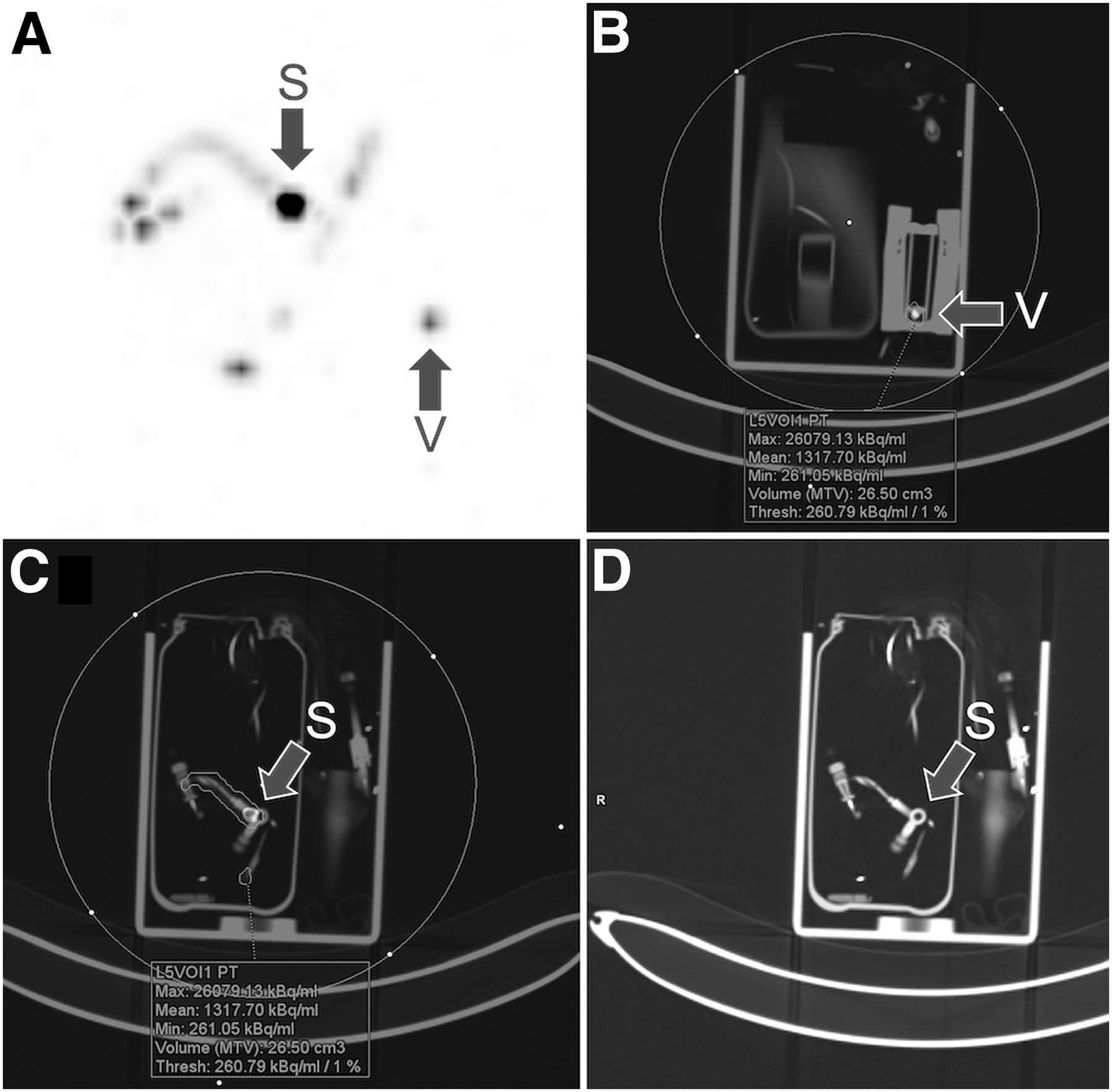
Figure 1 depicts 90Y PET/CT of residual activity within the delivery apparatus and catheters, packed within a plastic storage bottle and placed inside the standard acrylic glass delivery box. The syringe used in the transfer of microspheres from the shipping vial into the v-vial was not included but was visually clear of microspheres; hence, any residual activity was assumed negligible. 90Y PET/CT was performed within an hour of radioembolization on a Biograph Horizon scanner (Siemens) over 20 min. PET images were reconstructed using the Siemens TrueX time-of-flight iterative algorithm, 3 iterations and 10 subsets, a gaussian filter of 5 mm in full width half maximum, and a 180 × 180 matrix. Low-dose CT was performed for localization, attenuation correction, and scatter correction. The images were displayed in a 3-mm slice thickness and were analyzed using Siemens SyngoVia software. The institutional review board approved this report, and the requirement to obtain informed consent was waived.
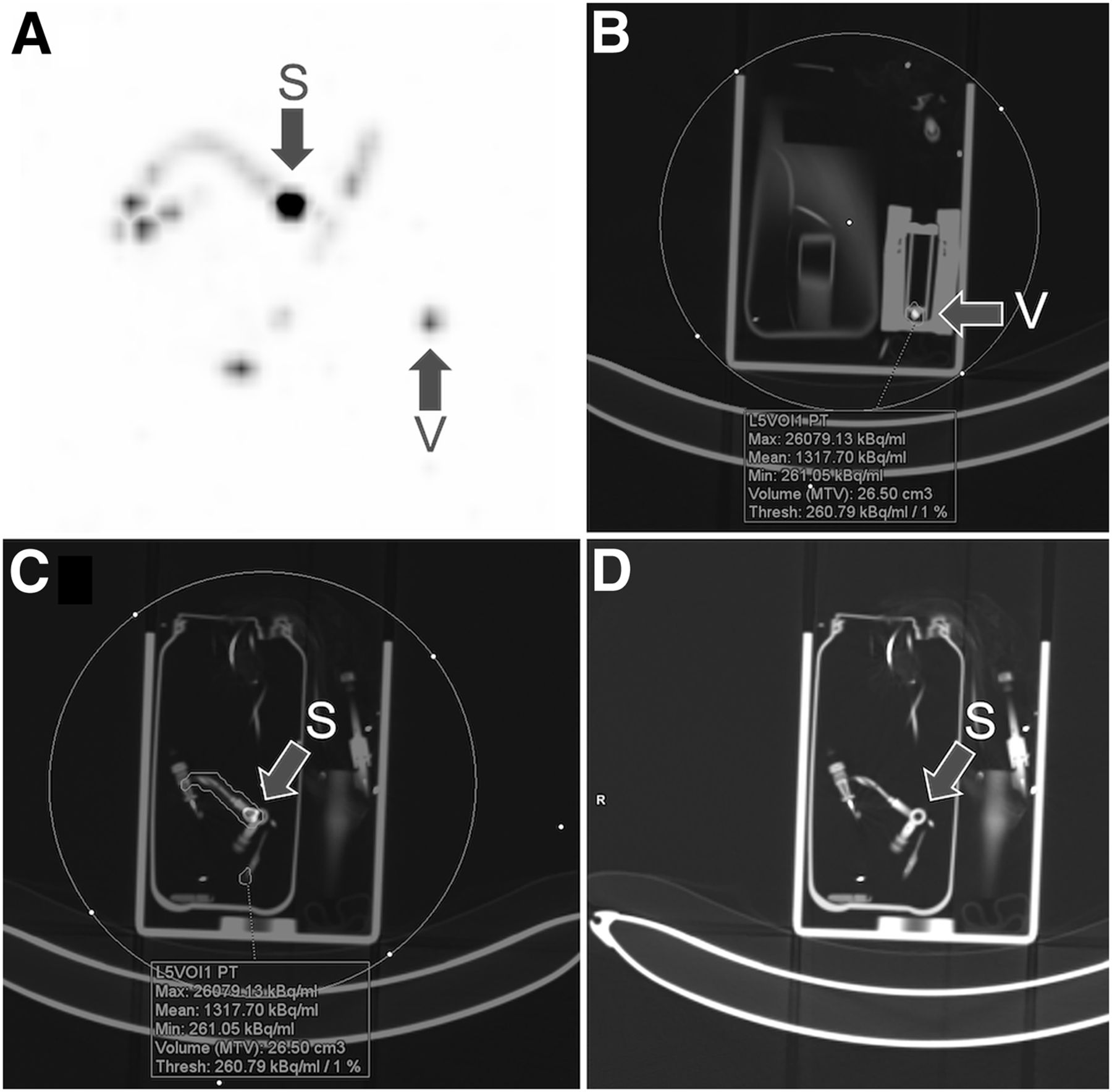
(A) Maximum-intensity projection shows mild residual activity along tubing and catheters, with focus of intense activity at stopcock junction. (B) Mild residual activity at bottom of v-vial. (C) Intense residual activity clearly localized to stopcock junction. (D) Stopcock junction as shown on low-dose CT. Volume of interest is encircled. MTV = metabolic tumor volume; S = stopcock junction; V = v-vial. Color version of this figure is available as supplemental file at http://tech.snmjournals.org.
RESULTS
Qualitatively, maximum-intensity projection depicted mild residual activity along the tubing and catheters (Fig. 1A), with a focus of intense activity. Mild residual activity was also seen at the bottom of the v-vial (Figs. 1A and 1B). The intense activity was clearly localized to the stopcock junction (Figs. 1C and 1D), a common site of resin microsphere trapping (5).
Quantitatively, a volume of interest was drawn around the entire delivery box (Figs. 1B and 1C), with the isocontour threshold set to 1%. The overall residual activity was directly calculated as the simple product of volume-of-interest radioconcentration (kBq/mL) and volume-of-interest volume (cm3). The measurements displayed in Figures 1B and 1C show the overall residual activity to be 35 MBq. In this example, the v-vial activity before radioembolization was 1.93 GBq; therefore, the residual activity was only 2% and in keeping with quality standards. The residual activity estimated using the manufacturer’s indirect dose-rate-meter method was less than 1%.
DISCUSSION
The delivery apparatus is assembled from multiple components; hence, there are many potential sites for microsphere trapping. The key advantage of 90Y PET/CT over the manufacturer’s indirect dose-rate-meter method is the ability to identify the location of the trapped microspheres, in addition to their direct quantification. Such specific feedback is valuable for quality assurance and to identify technical issues with preparation of the delivery apparatus or injection of the microspheres.
CONCLUSION
90Y PET/CT is a useful quality assurance tool for localization and direct quantification of residual activity within the delivery apparatus after radioembolization.
DISCLOSURE
Yung Kao has previously received research funding and speaker fees from Sirtex Medical Limited. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 24, 2020.
- Received for publication October 14, 2020.
- Accepted for publication November 9, 2020.





{kind=link}