


Abstract
On rare occasions, differentiated thyroid carcinoma causes tumor thrombosis in the great veins. Multimodality treatment with surgery, radioiodine therapy, and targeted therapies is used to manage tumor thrombosis associated with thyroid malignancies, though no established guidelines exist. We present a woman with a tracer-avid tumor thrombus in the right brachiocephalic vein after surgery for follicular thyroid carcinoma. Follow-up revealed an excellent response after treatment with 131I as a single modality for both remnant and tumor thrombus.
Tumor thrombosis may be detected as an incidental finding in various malignancies but is rare in thyroid cancer. An association between a tumor thrombus and both poorly and well-differentiated thyroid malignancies has been reported. Previous studies demonstrated varying involvement, ranging from the internal jugular vein to the right atrium (1–4). Established guidelines on the management of tumor thrombosis associated with thyroid malignancies are still lacking, though treatment options include combinations of surgery, 131I ablation, and external-beam radiotherapy. In patients with obvious signs of venous obstruction, a few investigators have reported a better outcome from using thrombectomy of the affected veins followed by adjuvant external-beam radiotherapy or 131I therapy for the residual disease (2–4). However, surgery is associated with an increased risk of morbidity and mortality (1–4). 131I therapy as a single modality has rarely been used, as extensive tumor thrombosis may result in unsuccessful treatment (5). This case report demonstrates successful treatment of a tumor thrombus from follicular thyroid carcinoma using 131I therapy as a single modality.
CASE REPORT
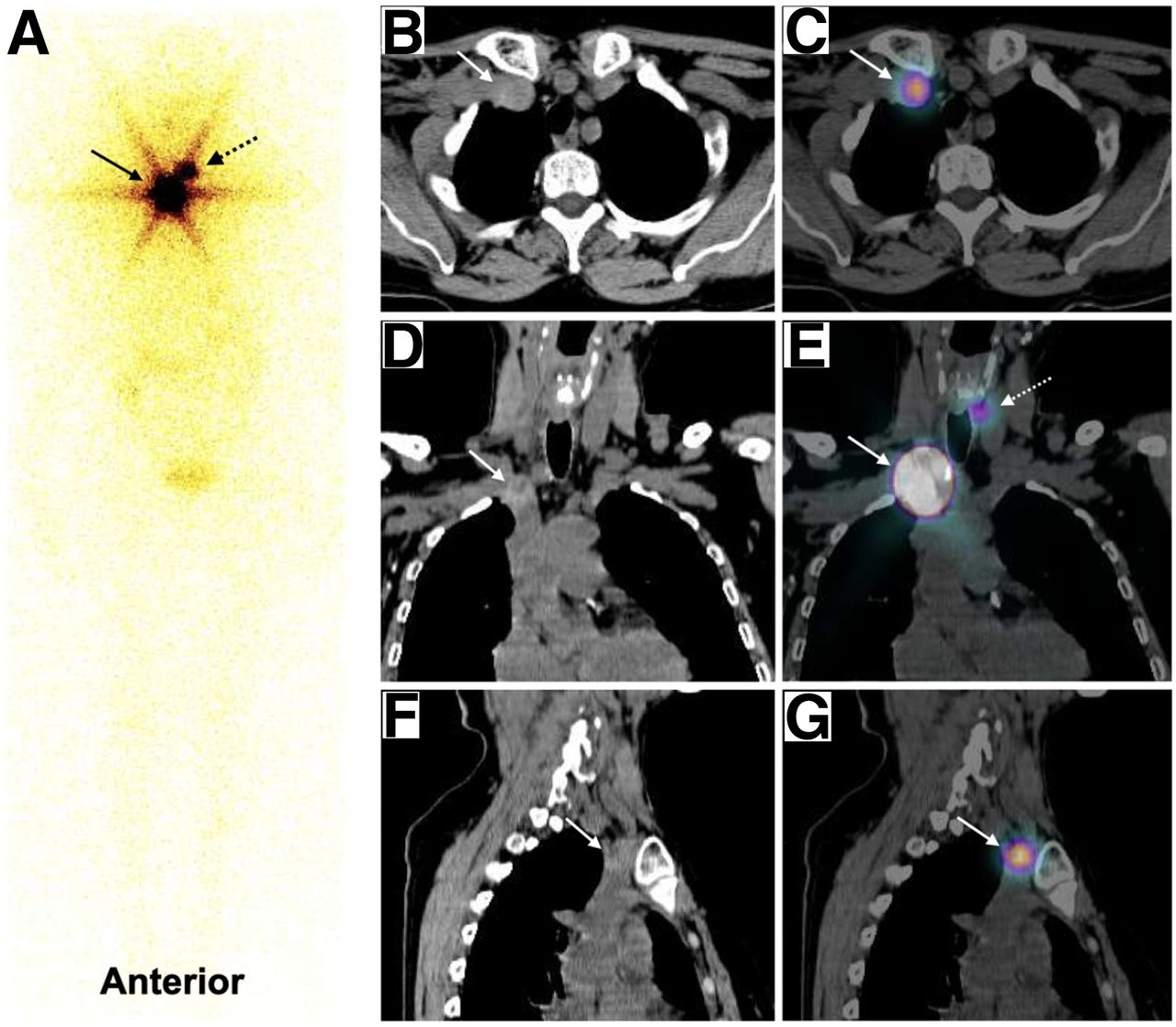
A 64-y-old woman who had undergone total thyroidectomy for follicular thyroid carcinoma presented with a postoperatively elevated level of stimulated serum thyroglobulin (>300 ng/mL) and a normal level of serum antithyroglobulin (14.1 IU/L). Her diagnostic whole-body 131I scan revealed a tracer-avid remnant in the thyroid bed and a small venous thrombus in the right brachiocephalic vein (Fig. 1). Contrast-enhanced CT was avoided because of possible interference with the planned 131I therapy. She was treated with 5,550 MBq (150 mCi) of 131I in view of the small size and tracer avidity of the tumor thrombus and the absence of any signs or symptoms of venous obstruction. At the 6-mo follow-up, the patient’s level of stimulated serum thyroglobulin (66.4 ng/mL) showed a trend to decrease, with a normal antithyroglobulin level and negative findings on 131I scanning. She was treated with 4,810 MBq (130 mCi) of 131I in view of the incomplete biochemical response. Subsequent follow-up at 6 mo after the second therapy revealed a significant decline in her level of stimulated thyroglobulin (2.28 ng/mL), with negative results on 131I scanning (Fig. 2) and neck ultrasonography. The next follow-up, at 1 y after therapy, revealed an excellent response (stimulated thyroglobulin < 0.2 ng/mL, antithyroglobulin < 15 IU/L), with negative results on 131I scanning and neck ultrasonography. She is on a suppressive dose of thyroid hormone and has been asymptomatic on subsequent follow-up visits.
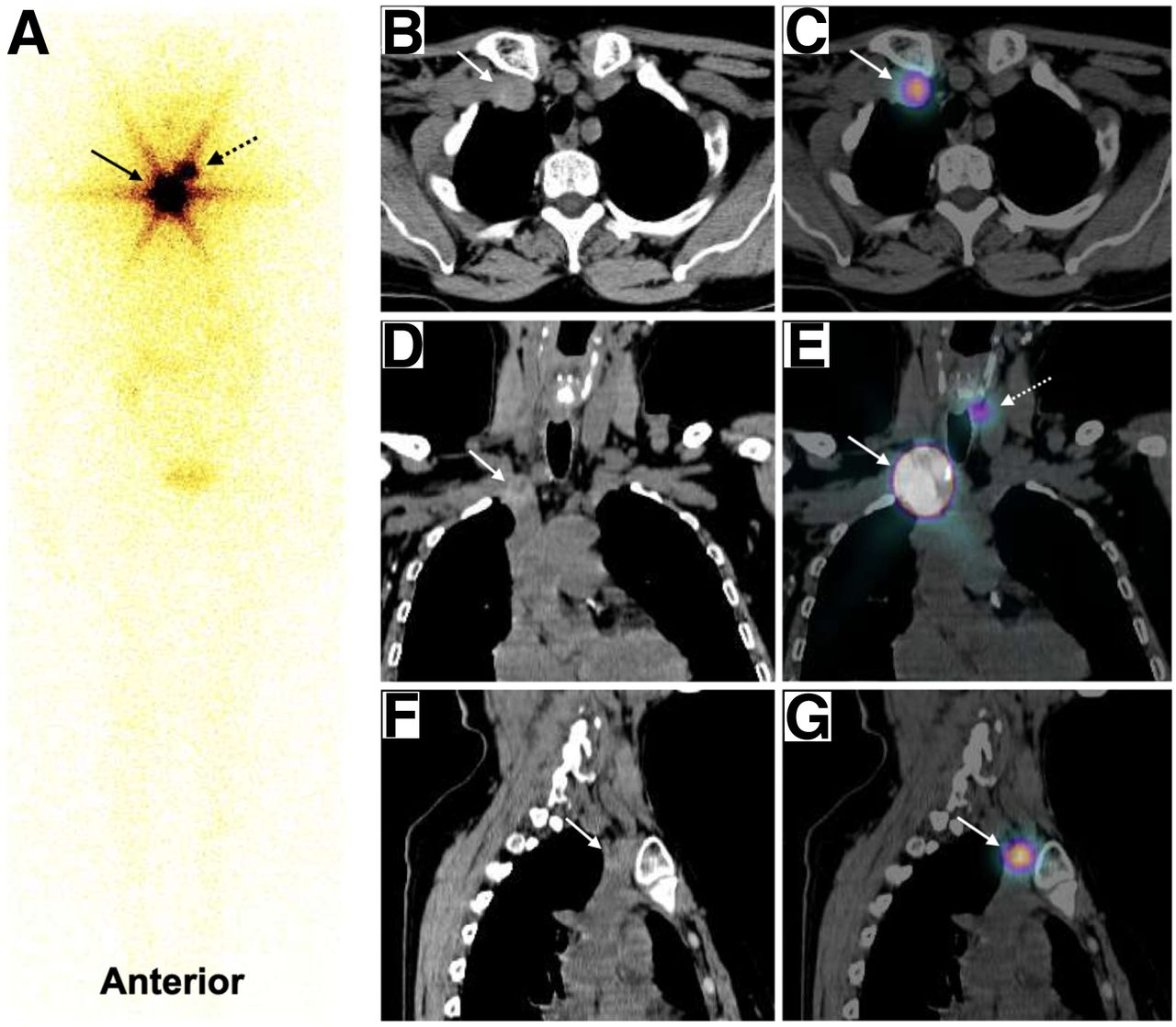
(A) Initial whole-body 131I planar images on Siemens Symbia T-series, showing focal tracer uptake in neck (dashed arrow) and intense focal tracer uptake in upper thorax (solid arrow). (B–G) CT images (B [axial], D [coronal], and F [sagittal]) and fused images (C [axial], E [coronal], and G [sagittal]) showing tracer uptake in remnant (dashed arrow) and relatively hyperdense thrombus in right brachiocephalic vein (solid arrows).
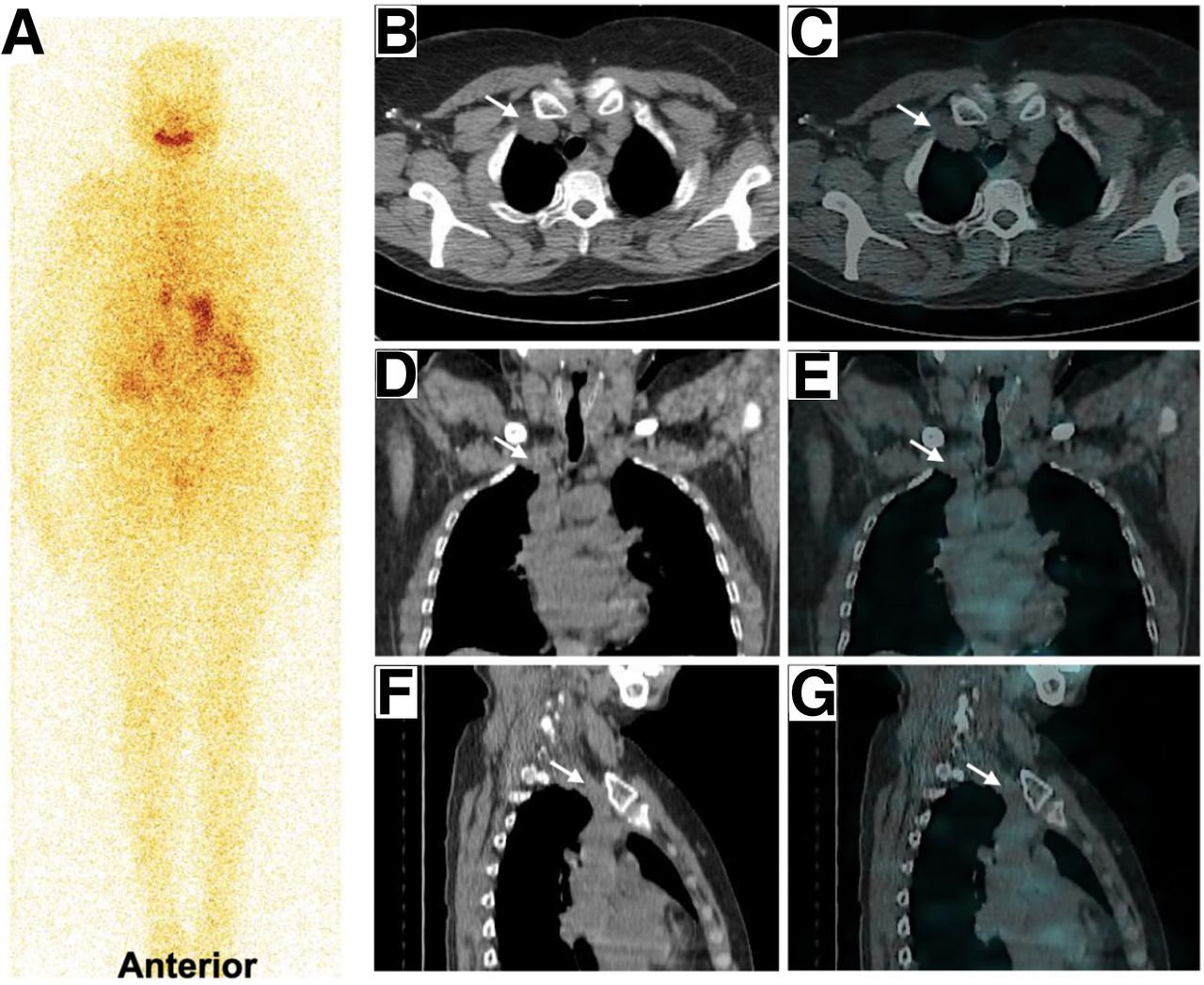
Follow-up whole-body 131I planar images (A), CT images (B [axial], D [coronal], and F [sagittal]), and fused images (C [axial], E [coronal], and G [sagittal]) on GE Healthcare Discovery 670-DR, showing complete resolution of tracer uptake and hyperdense lesion within right brachiocephalic vein (arrows).
DISCUSSION
This patient was incidentally diagnosed with a tumor thrombus in the right brachiocephalic vein on post-thyroidectomy diagnostic whole-body 131I scanning. Though the treatment options available for this patient were surgery, 131I therapy, and external-beam radiotherapy, certain factors such as her age and sex (high risk for surgery), the fact that the thrombus was tracer-avid and small, the absence of any signs or symptoms of venous obstruction, and the presence of a small remnant in the thyroid bed led us to choose radioiodine therapy for this patient. External-beam radiation therapy was not considered, because 131I therapy alone produced an excellent response and because we wished to avoid the morbidities associated with radiotherapy.
CONCLUSION
131I therapy as a single modality may be considered for elderly patients having well-differentiated disease with a small, tracer-avid, unobstructive thrombus, as was done in this index case after a risk–benefit analysis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 4, 2020.
REFERENCES
- Received for publication April 11, 2020.
- Accepted for publication July 9, 2020.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.