


Abstract
A new protocol for rapid SPECT/CT blood pool imaging consisting of fewer image-angle acquisitions (fewer-angle SPECT/CT, or FASpecT/CT) was evaluated for localization of focal sites of soft-tissue inflammation, infection, and osteomyelitis. Methods: Immediately after dynamic flow and standard planar blood pool imaging with 99mTc-methylene diphosphonate, FASpecT/CT was performed with a dual-head γ-camera consisting of 6 steps over 360°, 12 total images with 30° of separation between angles, and 30 s per image, requiring a total imaging time of approximately 3 min. Images were reconstructed using iterative ordered-subset expectation maximization. Before use in a patient-care setting, various FASpecT/CT acquisition protocols were modeled using a phantom to determine the minimum number of stops and the stop duration required to produce a reliable image. Results: FASpecT/CT images provided excellent 3-dimensional localization of spine osteomyelitis, soft-tissue infection of the foot, and tendonitis of the hand and foot using a 3-min image acquisition time. The FASpecT/CT acquisition protocol required 1.3–3.5 min, including camera movement time. This was a reduction of 72%–90% from the time required for the standard 60-angle, 20-s SPECT/CT acquisition. Conclusion: The ability of FASpecT/CT blood pool images to help localize focal sites of hyperemia and inflammation can increase exam sensitivity and specificity. Additionally, using a FASpecT/CT protocol decreases imaging time by up to 90%.
Blood pool imaging is frequently performed as the second phase of 3 phases in scintigraphic bone scanning to demonstrate inflammation associated with osteomyelitis. Focal regions with increased activity on the 3 phases of flow, blood pool, and delayed imaging are deemed to be 3-phase–positive and consistent with a diagnosis of osteomyelitis, although this finding also occurs with fracture, recent orthopedic hardware placement, and neuropathic joints (Charcot arthropathy) (1,2). A challenge with standard planar blood pool images is that specific localization of the focal region of increased blood pool, that is, hyperemia or inflammation, is not possible, limiting interpretation of the study. This is particularly true in regions with overlying normal hyperemic muscles and other soft tissues, such as the calf and spine. Blood pool localization is also poorly defined in the forefoot, in which focal soft-tissue blood pool activity cannot be readily distinguished from blood pool activity in the bone, primarily because of the small size of the anatomic structures.
This challenge of precise anatomic localization is found with all planar imaging in nuclear medicine and has led to the rapid proliferation of exams using SPECT/CT (3). SPECT/CT has been shown to increase sensitivity and specificity in 3-phase bone scans and to result in changes in management versus planar imaging alone (4,5). The primary diagnostic limitation of SPECT/CT is patient motion and misregistration, which are due at least in part to the long acquisition times of SPECT, ranging from 20 to 30 min. Additionally, this long acquisition time is impractical for the blood pool phase of a 3-phase bone scan. Solutions to these problems have been posited, including immobilizing the body part being imaged and reducing the image acquisition time (6–10).
Advances in iterative reconstruction, now available in most nuclear medicine clinics (11), have played a significant role in enabling reduced-dose or rapid acquisitions. Iterative reconstruction of images comprising a greatly reduced number of angular image samples has also been described for reconstruction of 3-dimensional images in other image-based fields, such as photoacoustic imaging and cone-beam CT imaging (12,13). For example, iterative reconstruction of sparse-view (30 image angles as opposed to 900 image angles) cone-beam CT has been shown to produce high-quality tomographic images (12), and photoacoustic imaging with iterative reconstruction derived from as few as 15 detectors has been shown to produce tomographic images similar to those using 120 detectors (13).
Our hypothesis was that it would be possible to develop an imaging protocol that would enable SPECT/CT imaging of the blood pool phase of the 3-phase bone scan to improve localization. In this article, we describe a method of reducing the SPECT/CT acquisition time to approximately 3 min, which we refer to as fewer-angle SPECT/CT, or FASpecT/CT. FASpecT/CT images were obtained of the blood pool phase of bone scans with a greatly reduced number of acquisition angles, specifically 6 steps over 360°, 12 total images with 30° of separation between angles, and 30 s per image, requiring a total SPECT imaging time of approximately 3 min. The FASpecT images were acquired rapidly after 99mTc-methylene diphosphonate (MDP) administration for specific localization of sites of inflammation and infection. FASpecT/CT has previously been reported as a method to decrease the required imaging time or increase the detection efficiency for radioiodine pretherapy and posttherapy imaging (10).
MATERIALS AND METHODS
The study was approved by the institutional review board, and the need for written informed consent was waived. Imaging studies were initially performed with a phantom to compare the characteristics of standard SPECT/CT and FASpecT/CT images with differing acquisition times and angle samples. Subsequently, FASpecT/CT was performed on 4 patients to demonstrate its clinical use for tomographic blood pool imaging.
Phantom Studies
Phantom Description
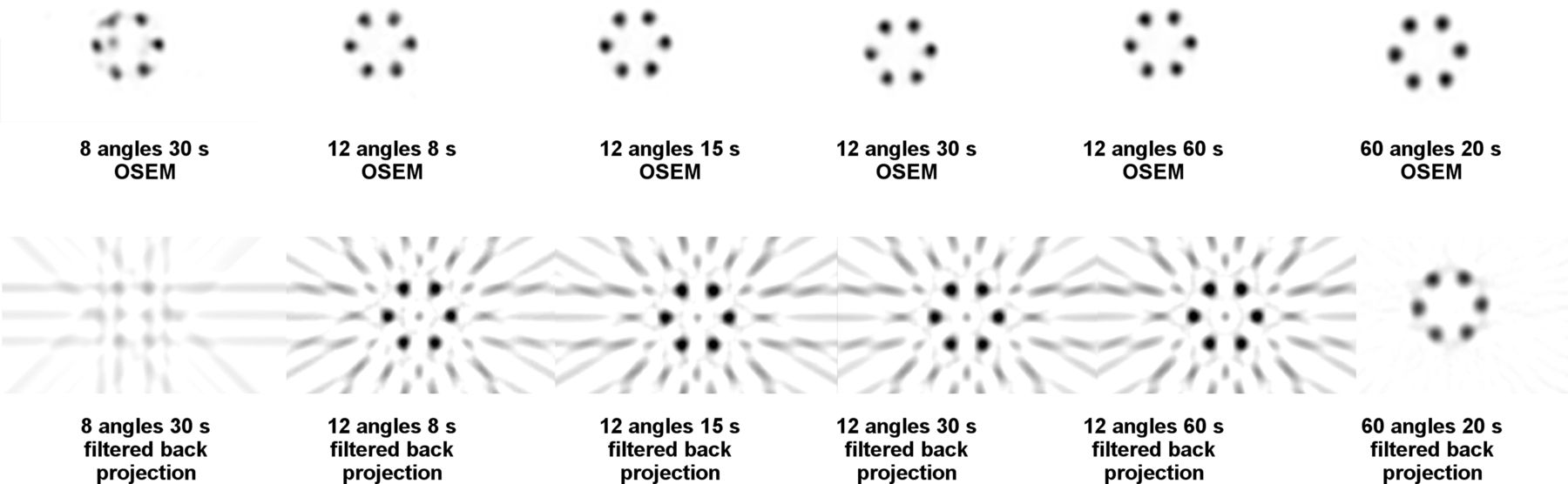
A phantom was used to compare images acquired with different times and angle-sample parameters. This phantom consisted of 19 water-filled glass cylinders containing 25 mL of water each and mounted into a hexagonal configuration. All cylinders were fully filled with water, and 6 of the outer cylinders were filled with 2.6 ± 0.07 MBq of 99mTc-MDP of activity. In the first phantom, the 6 cylinders were spaced evenly on the outer ring as seen in Figure 1. In the second phantom, the 6 cylinders were placed randomly in the outer ring, with several of the cylinders being adjacent to one another as seen in Figure 2. This amount of activity (0.104 MBq/mL of water) was chosen in accordance with our medical physicist based on an approximation of blood pool activity anticipated at 5 min after administration when a 925-MBq 99mTc-MDP bone dose is distributed within the average human clinical circulating blood volume of 5,000 mL, allowing for clearance of approximately 50% of the activity from blood.
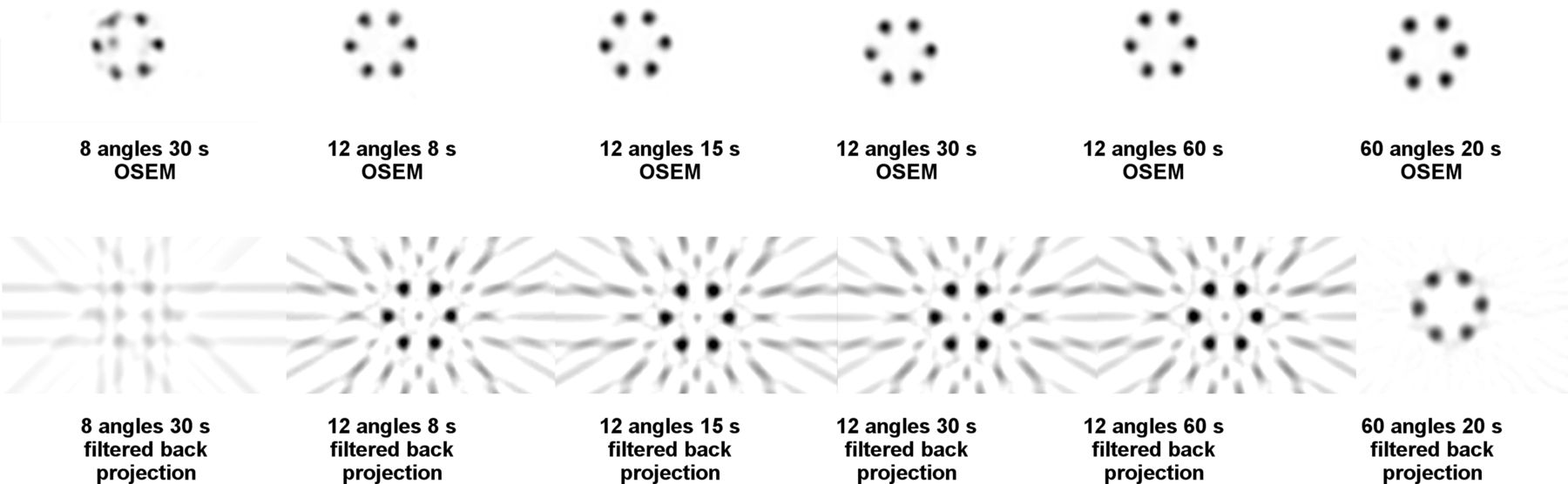
SPECT images of phantom with symmetrically distributed cylinders acquired with various image angles and times. SPECT acquisitions in top row are processed with OSEM, and same SPECT images in bottom row are processed with filtered backprojection. Images are labeled with number of images and times for acquisitions. Standard SPECT protocol is 60 angles and 20 s per image.
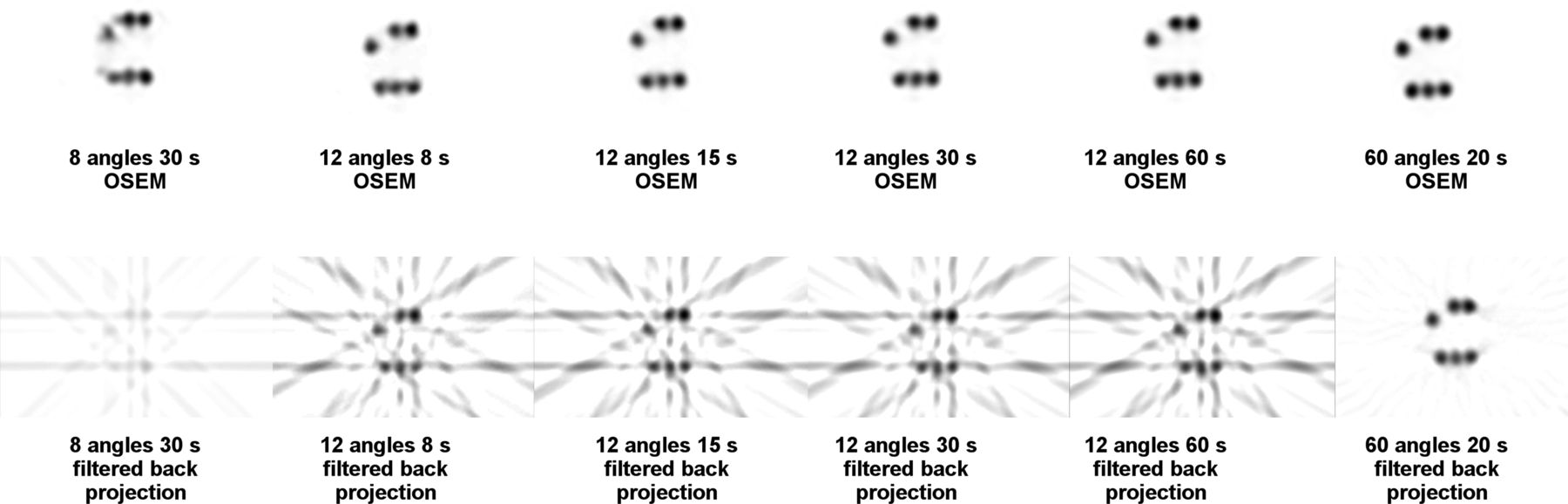
SPECT images of phantom with randomly placed activity-containing glass vial cylinders. Image parameters are same as in Figure 1.
SPECT Image Acquisition
SPECT imaging studies of each phantom were performed using differing acquisition times and a differing number of total image-angle samples for visual comparison of image quality. Images were acquired using reduced numbers of angle samples: 8 views for 30 s, 12 views for 8 s, 12 views for 15 s, 12 views for 30 s, and 12 views for 60 s per image sample. A standard SPECT acquisition of 60 views for 20 s was obtained for comparison. SPECT data were processed with both ordered-subset expectation maximization (OSEM) iterative reconstruction and filtered backprojection. The OSEM images were processed with 2 iterations and 10 subsets using a Butterworth filter with a critical frequency of 0.48 and power of 10. The filtered backprojection images were processed using a Butterworth filter with a critical frequency of 0.48 and a power of 10. Transaxial images of slices through the center of the cylinders are shown in Figures 1 and 2 for all the different SPECT acquisitions.
Clinical Studies
Immediately after injection of 925–1,110 MBq of 99mTc-MDP in 4 different representative clinical patients, dynamic flow and planar blood pool images were acquired over each patient’s region of concern using a 128 × 128 matrix over 3 min. Immediately after these planar images, FASpecT/CT of the blood pool phase was performed using a dual-head SPECT/CT camera (GE Infinia Hawkeye 4; 6 steps, 12 total images with 30 s per images; Table 1). Immediately afterward, CT was performed with the patient in the same position. Images were reconstructed with GE Healthcare Xeleris functional imaging software using the iterative reconstruction parameters specified for FASpecT in Table 1. Example FASpecT/CT blood pool images of clinical patients with spine osteomyelitis, soft-tissue infection of the foot, and tendinitis of the wrist and foot are shown in Figures 3–6. Follow-up delayed 3-h bone scanning was performed, and when appropriate, either 67Ga- or 111In-white blood cell imaging was performed as per standard clinical protocols for comparison.
Comparison of Acquisition and Processing Parameters Between FASpecT and Standard SPECT for Blood Pool Imaging
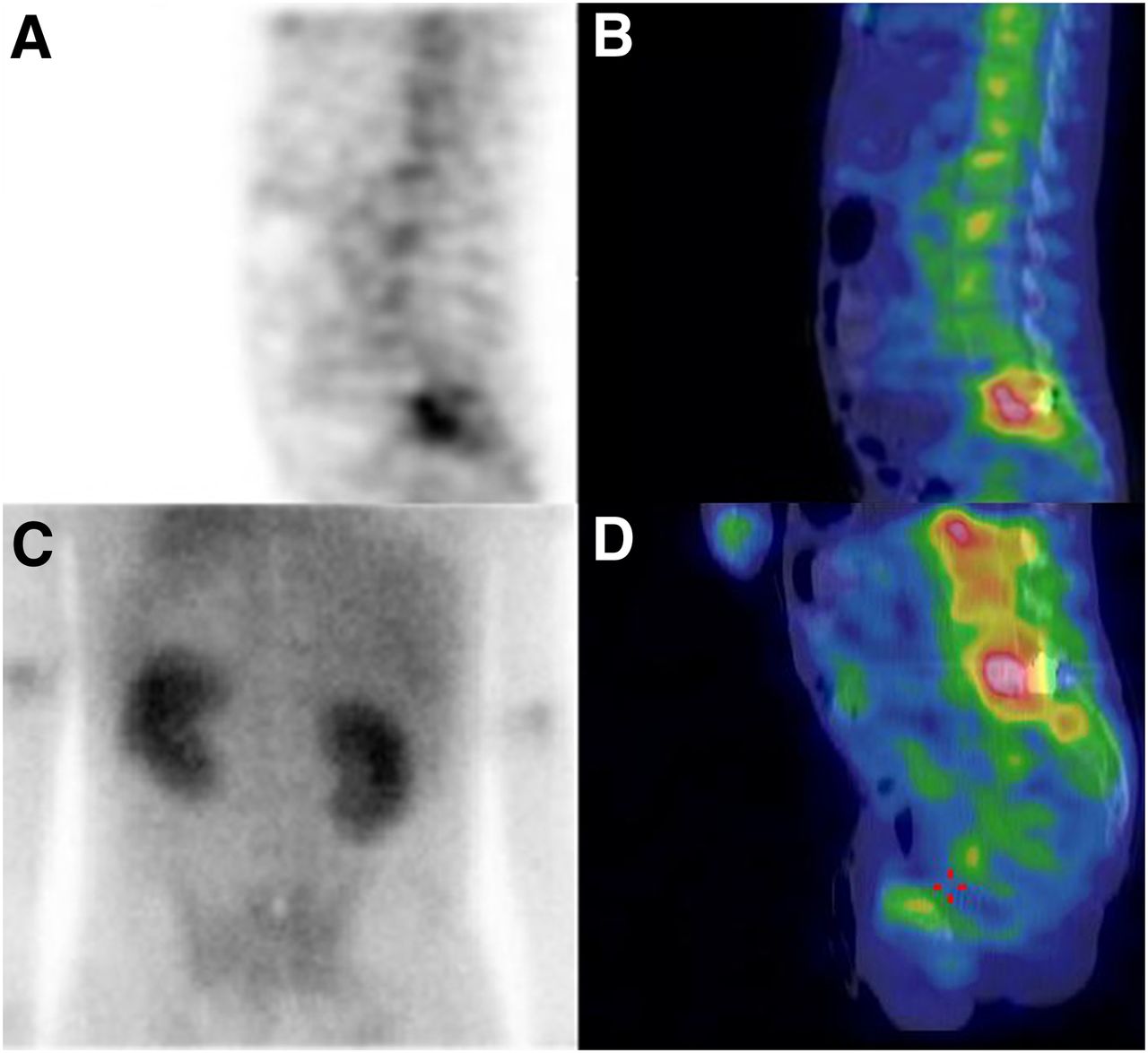
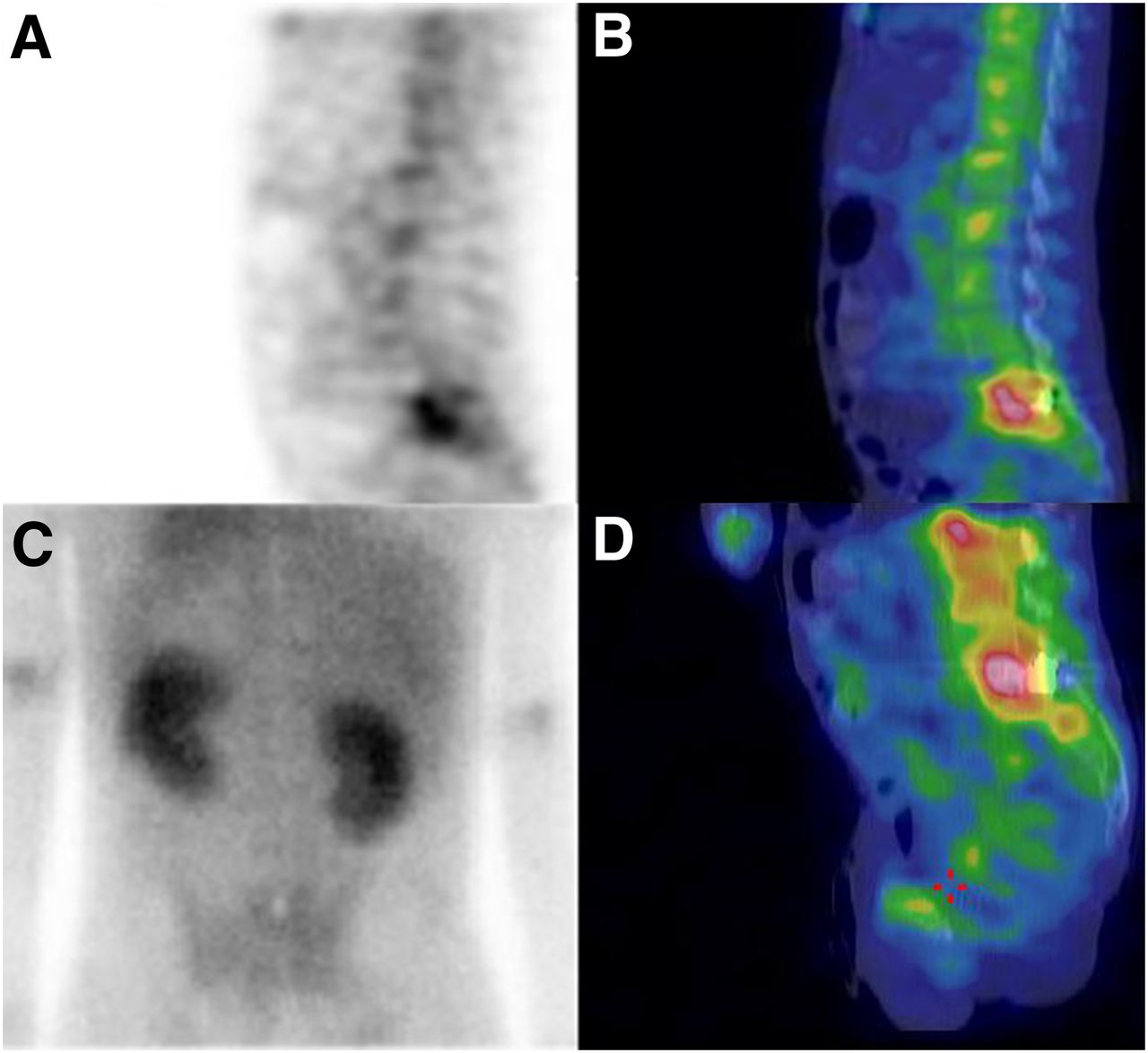
Imaging of spine: FASpecT blood pool sagittal image (A), FASpecT/CT blood pool sagittal image (B), posterior planar blood pool image (C), and 67Ga citrate SPECT/CT sagittal image (D). FASpecT/CT blood pool images demonstrate intense focally increased uptake at L5–S1 vertebrae that is poorly localized on planar image. Subse-quent 67Ga citrate image demonstrates infection corresponding to region of increased blood pool uptake on FASpecT image.
RESULTS
Phantom Studies
Results for the phantom studies are shown in Figures 1 and 2. The phantom imaging results were compared visually by 4 board-certified nuclear medicine physicians. FASpecT images obtained with iterative reconstruction were superior to those obtained with filtered backprojection. In the images with 12 angle samples, image quality decreased as the acquisition time decreased; however, images with 12 angle samples acquired for 30 and 60 s compared favorably with images with standard SPECT parameters of 60 angles acquired for 30 s. FASpecT required 1.3–3.5 min, including camera movement time. This was a reduction of 72%–90% from the time required for standard 60-angle, 20-s SPECT. Images with only 8 angle samples were inferior to those with 12 angle samples, with image artifacts and poor localization of the activity in the phantoms. The phantom studies with random placement of activity had similar findings.
DISCUSSION
The FASpecT/CT blood pool imaging protocol described in this article provided specific localization of sites of hyperemia and inflammation, facilitating arrival at specific clinical diagnoses and improving patient care. We found that FASpecT/CT has particular promise for the imaging and diagnosis of musculoskeletal pathologies. Figure 3 shows that a precise focus of blood pool activity at the lumbosacral joint was found using FASpecT/CT but not with planar blood pool imaging. This localization of infection was not affected by the metallic artifact from the patient’s spinal fusion hardware. The ability to image specific sites of infection and inflammation in the spine with blood pool tomographic imaging has the potential to favorably impact spine care and direct treatment specifically to sites of spinal inflammation. FASpecT/CT may prove to be an additional tool for improving the diagnosis and treatment of low back pain, the primary cause of musculoskeletal system–related disability in the developed world (14).
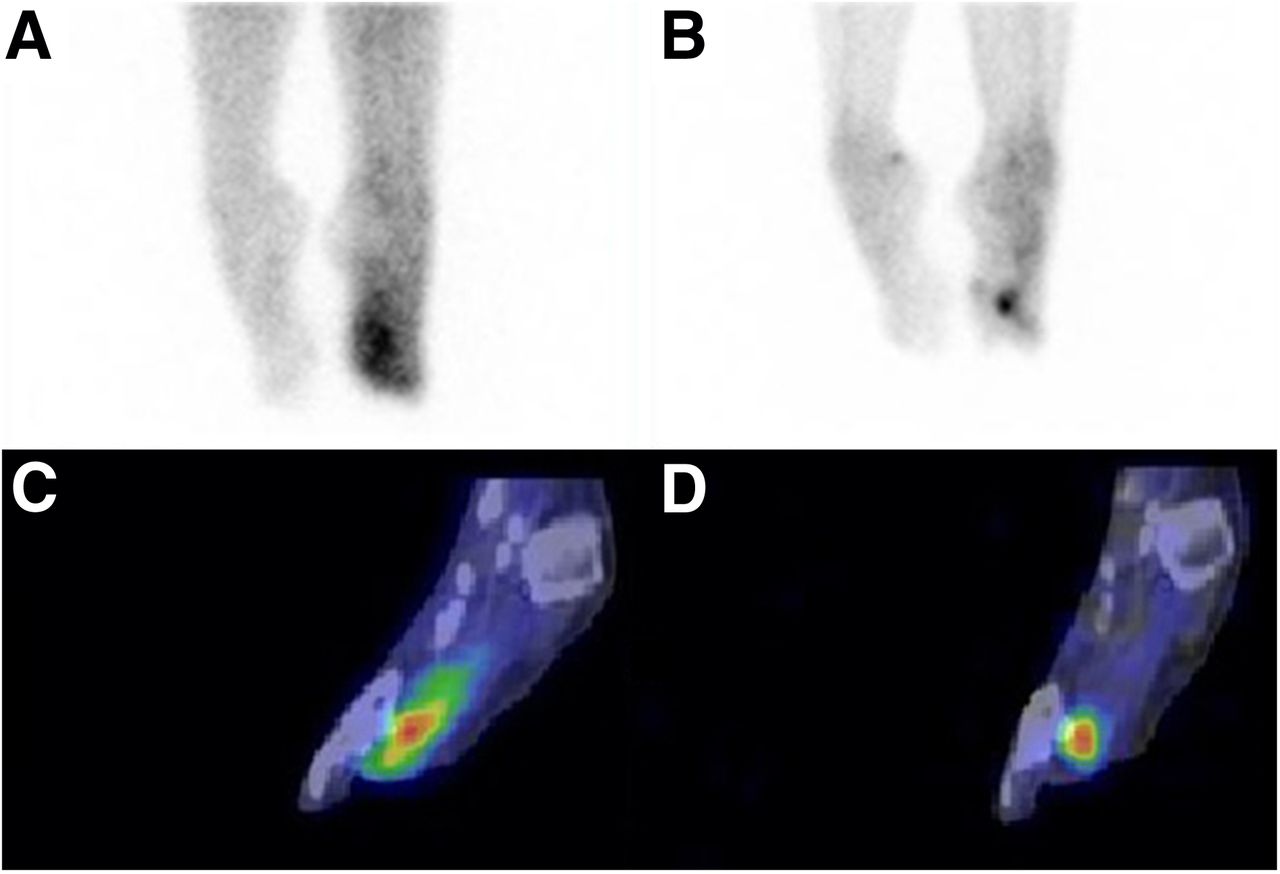
FASpecT/CT also has significant promise in the evaluation of soft-tissue and bone infections of the foot. In Figure 4, the FASpecT/CT images demonstrate increased blood pool activity in soft tissue adjacent to the second metatarsal bone but not within the bone itself. By standard planar imaging alone, the region of the second metatarsal would have inappropriately been found suggestive of osteomyelitis. Follow-up 111In-white blood cell SPECT/CT confirmed that the infection was localized only to the soft tissues of the foot adjacent to the second metatarsal bone, which was the same region as that with blood pool activity on the FASpecT/CT image.
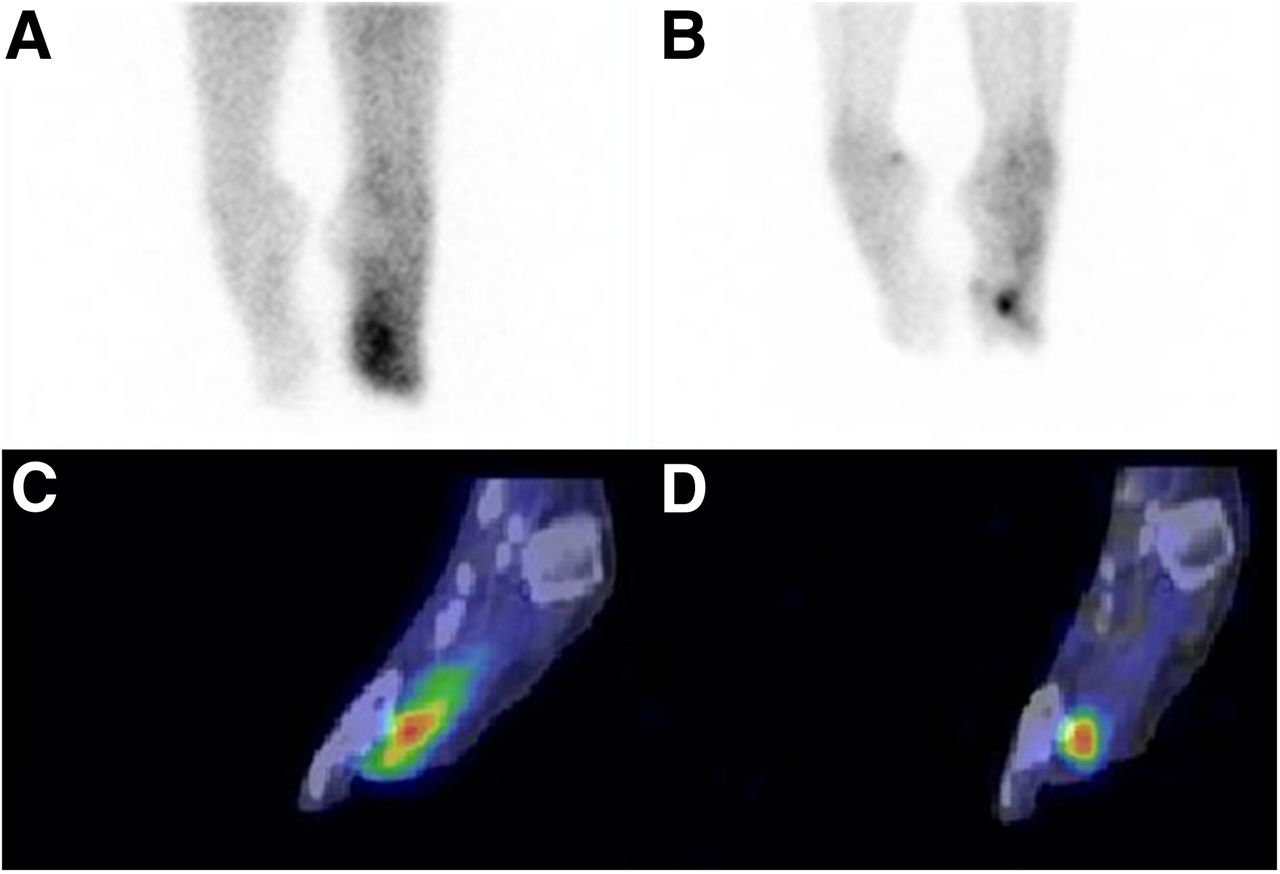
Imaging of feet: anterior planar blood pool image (A), anterior planar delayed bone scan (B), FASpecT/CT blood pool sagittal image of left foot (C), and 111In-white blood cell SPECT/CT sagittal image of left foot (D). Planar blood pool image demonstrates diffuse increased blood pool activity that cannot be precisely localized. Delayed planar bone scan shows focal bone uptake consistent with 3-phase positivity of region of left distal second metatarsal. However, FASpecT/CT blood pool image demonstrates focal soft-tissue blood pool activity of left foot without apparent bone involvement. Subsequent 111In-white blood cell SPECT/CT image shows focal soft-tissue activity without bone activity, correlating with FASpecT/CT blood pool imaging.
In Figure 5, FASpecT demonstrates increased blood pool activity within the extensor pollicis brevis tendon, supporting a diagnosis of de Quervain tenosynovitis, for which early diagnosis is important for proper treatment (15). This diagnosis was not evident from the planar blood pool or delayed-phase images.
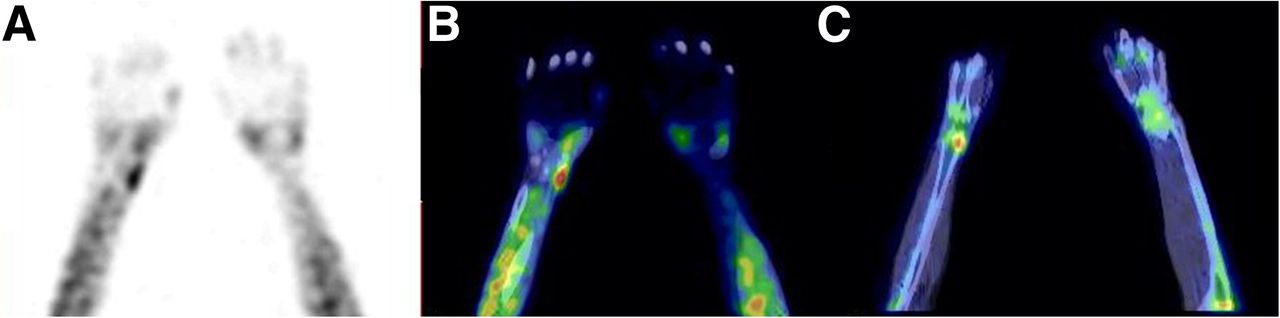
Imaging of hands: FASpecT blood pool image (A), FASpecT/CT blood pool image (B), and delayed SPECT/CT bone image (C). FASpecT/CT blood pool images show increased linear blood pool activity along distribution of right extensor pollicis brevis tendon characteristic of De Quervain tenosynovitis. Delayed bone scan shows focally increased uptake only in distal radius at origin of extensor pollicis brevis tendon, most likely because of increased regional blood flow. Planar blood pool image (not shown) showed minimal asymmetric increased blood pool uptake in right wrist that could not be localized.
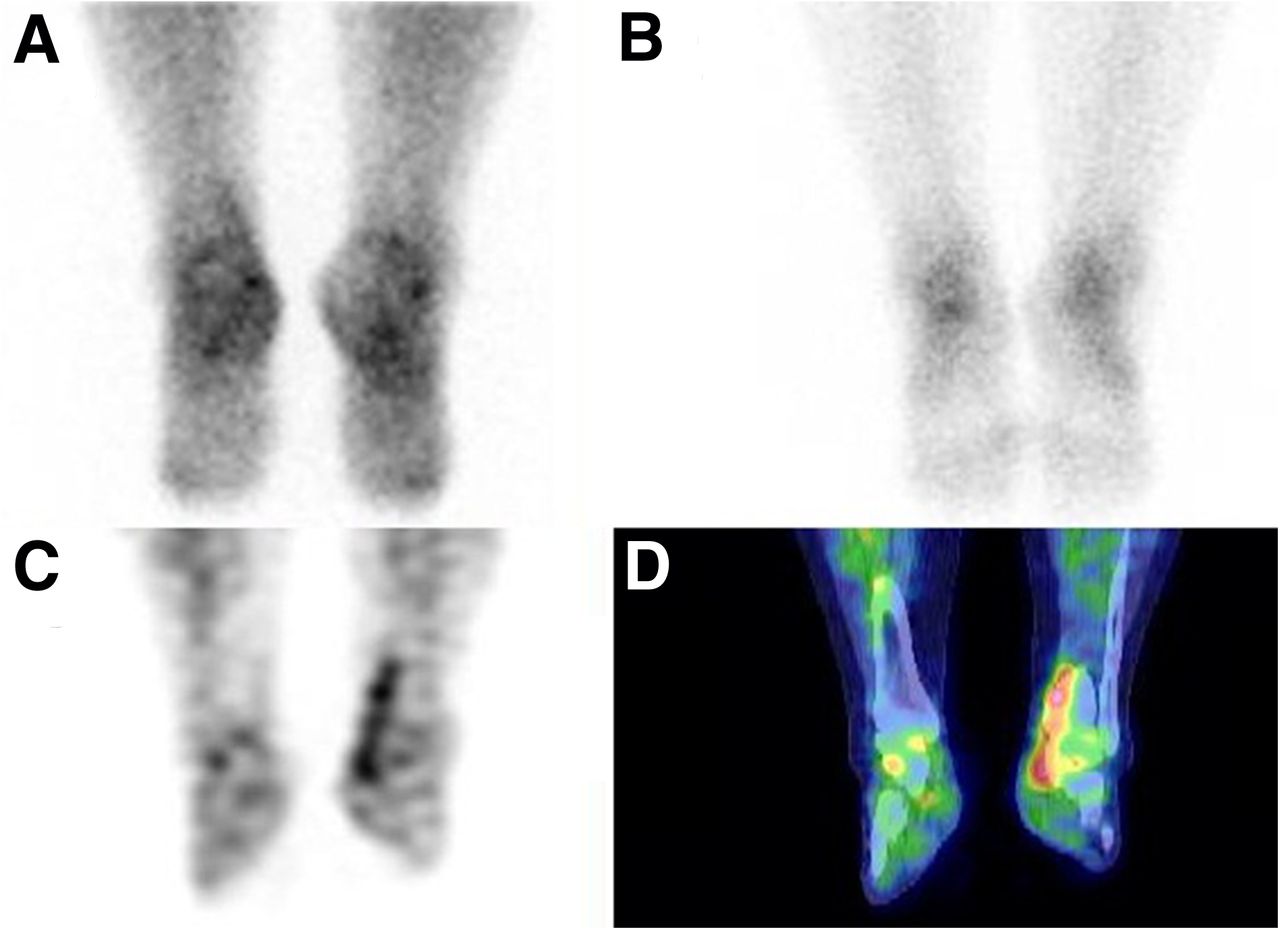
In Figure 6, FASpecT demonstrates linear increased activity associated with the posterior tibial tendon. Again, this localization is not possible on planar images. Early diagnosis of this condition is important as it can progress from tendonitis at stage I to deformity at stage II and a severe disability at stages III and IV (16).
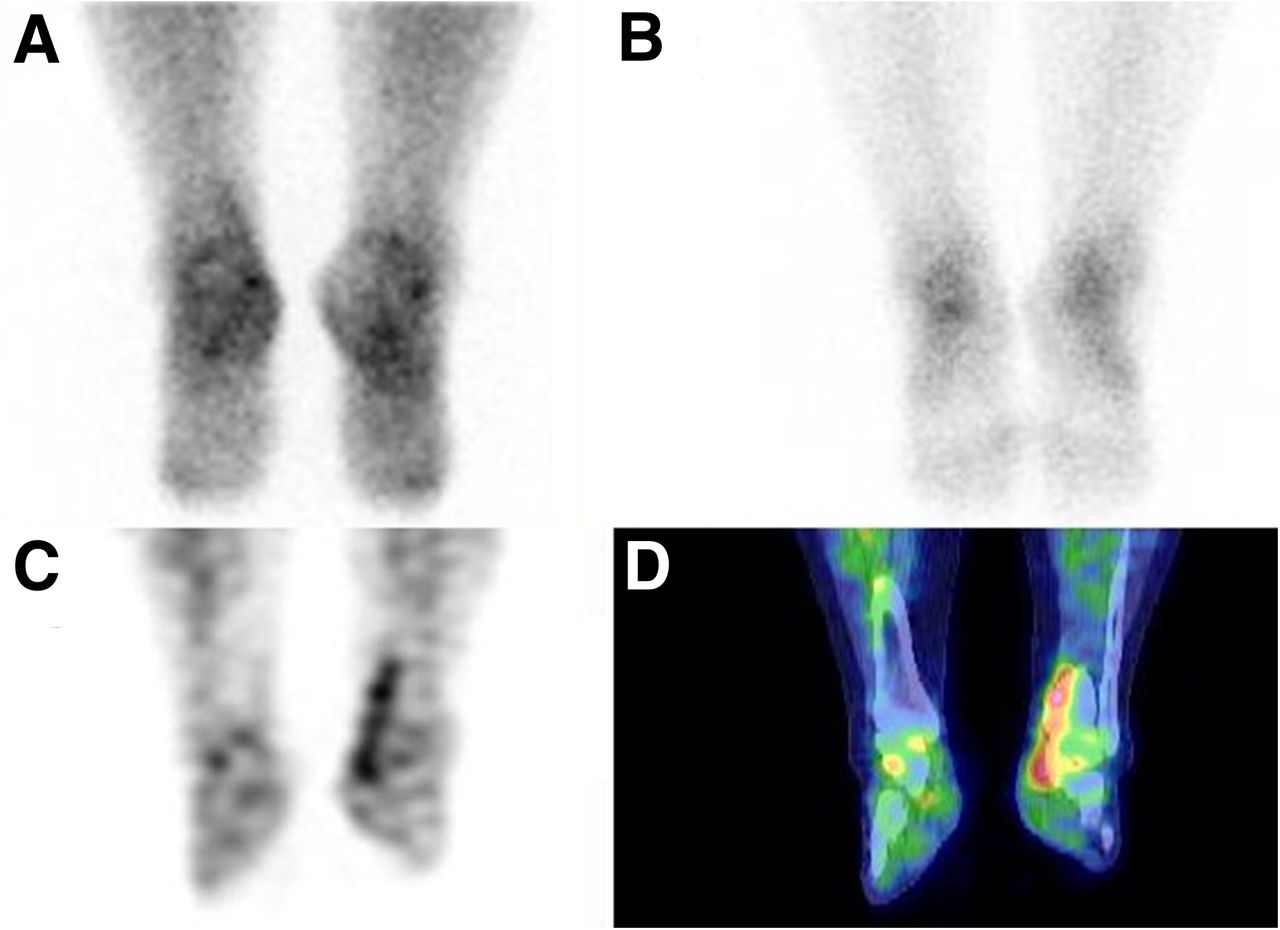
Imaging of feet and ankles: posterior planar blood pool image (A), posterior planar delayed bone scan (B), FASpecT blood pool coronal image (C), and coronal SPECT/CT blood pool coronal image (D). FASpecT/CT blood pool images demonstrate focally increased uptake along posterior tibial tendon consistent with tendonitis. Findings on delayed bone scan are essentially normal, and posterior planar blood pool scan shows asymmetry that cannot be localized.
The iterative reconstruction for FASpecT provides significantly better image quality than filtered backprojection when using a greatly reduced number of angle samples. Although filtered backprojection remains the most commonly used method for reconstructing SPECT myocardial perfusion images (9), iterative SPECT reconstruction has become more popular as a method to reduce image artifacts and noise. The most commonly used iterative reconstruction method is OSEM, although other iterative methods have also been evaluated (17). Currently, the main focus of research using iterative reconstruction has been on reducing the administered doses in cardiac SPECT imaging and developing faster imaging procedures (6–9). A prior study iteratively reconstructed SPECT images containing either 30, 60, or 120 image angles while maintaining constant pixel counts in the reconstructed images. The SPECT images with 30 angle samples compared favorably with those with either 60 or 120 angles. That study concluded that a combination of iterative reconstruction with OSEM and a reduced number of angle samples may be a clinically useful method of reducing the time required for SPECT imaging (18). Although iterative image reconstruction makes it possible to obtain higher-quality 3-dimensional images using fewer angle samples, there have been no prior reports of using fewer-angle protocols to reduce the acquisition time for SPECT blood pool imaging.
FASpecT/CT with greatly shortened imaging times may have applications for dynamic SPECT/CT acquisitions using radiopharmaceuticals other than 99mTc-MDP. SPECT/CT is used routinely in clinical practice for many other types of exams, including parathyroid localization using 99mTc-sestamibi, neuroblastoma evaluation using 123I-metaiodobenzylguanidine, and Parkinson evaluation using 123I-ioflupane, to name just a few. SPECT/CT with a traditional number of imaging angles (60–120) has been described for assessment of occult gastrointestinal bleeding with 99mTc-labeled red blood cells (19) and for assessment of myocardial flow reserve using 99mTc-sestamibi (20). The use of rapidly acquired FASpecT/CT imaging may prove useful in these and other new applications to greatly reduce imaging times. Such applications would have wide-ranging positive effects, including reduced patient motion and increased throughput.
CONCLUSION
The ability of FASpecT/CT blood pool images to help localize focal sites of hyperemia and inflammation can increase exam sensitivity and specificity. Additionally, using a FASpecT/CT protocol decreases imaging time by up to 90%.
DISCLOSURE
No potential conflict of interest relevant to this article was reported. The opinions and assertions expressed herein are those of the authors and do not necessarily reflect the official policy or position of Walter Reed National Military Medical Center or the Department of Defense.
Footnotes
Published online Dec. 24, 2020.
REFERENCES
- Received for publication September 15, 2020.
- Accepted for publication October 22, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.