


Abstract
A pilot study was performed to determine whether the raw data from routinely obtained upright and supine myocardial perfusion scan (MPS) imaging could be used as an opportunity to screen for obstructive sleep apnea (OSA). We hypothesized that abnormal respiratory motion seen only on supine imaging (not upright imaging) corresponds with OSA. MPS supine-only respiratory motion was compared with known OSA diagnoses and with risk factors known to be associated with OSA. Methods: We reviewed 154 consecutive MPS studies from patients at our institution, including both exercise and chemical stress testing. All examinations were obtained because there was clinical suspicion of myocardial ischemia. We used the MPS panogram to assess for respiratory motion on supine stress or upright rest or stress imaging. We obtained the age, sex, body mass index, hypertensive history, and continuous positive airway pressure or OSA diagnosis history. Results: We compared the patients who had supine, stress-only respiratory motion with the remaining patients, assessing their OSA risk factors and known OSA diagnoses. In total, 65 patients (42.2%) had 3 or more OSA risk factors and 26 patients (16.9%) had a known OSA diagnosis. A similar percentage of patients with abnormal supine-only respiratory motion and patients with 3 or more OSA risk factors had a known OSA diagnosis, 9 (16.7%) and 14 (21.5%), respectively. Conclusion: We found a similar prevalence of known OSA diagnoses in patients with abnormal supine-only respiratory motion on MPS studies and patients with 3 or more OSA risk factors. The pilot study suggests that assessment of motion on MPS studies may provide an opportunity to also screen for OSA.
Obstructive sleep apnea (OSA) is a silent, growing problem in the United States and developed world, associated with multiple comorbidities and mortality (1–7). Some of the morbidities are directly caused by OSA, such as motor vehicle accidents, whereas others are associated with, but not necessarily caused by, OSA (7). These associated morbidities include stroke, hypertension, cardiovascular disease, and cardiac dysrhythmias (1–3,6). OSA is also associated with increased all-cause mortality (6). Consequently, it is important to identify OSA early, when intervention can prevent or alleviate some of these health issues.
The gold standard in OSA diagnosis is polysomnography, which can be expensive and not accessible for many patients (5,6,8–10). Many questionnaires have been developed to screen for OSA, followed by confirmation with polysomnography (8–22). The STOP-BANG questionnaire, developed by Dr. Frances Chung, has demonstrated the best sensitivity among multiple individual studies and systematic reviews (11,12,15–18,20–22). The letters of the acronym STOP-BANG refer to the yes/no metrics of the questionnaire, including Snoring, feeling Tired (fatigued or sleepy) during the daytime, Observed apneic events, high blood Pressure, Body mass index greater than 35 kg/m2, Age greater than 50 y, Neck circumference greater than 40 cm, and male Gender (11,22). Patients with 3 or more positive STOP-BANG metrics were found to have a high risk of OSA, compared with patients with fewer than 3 positive metrics. Subsequent studies and systematic reviews demonstrated the superiority of the STOP-BANG questionnaire and the increased probability of moderate to severe OSA in patients with higher STOP-BANG scores (20).
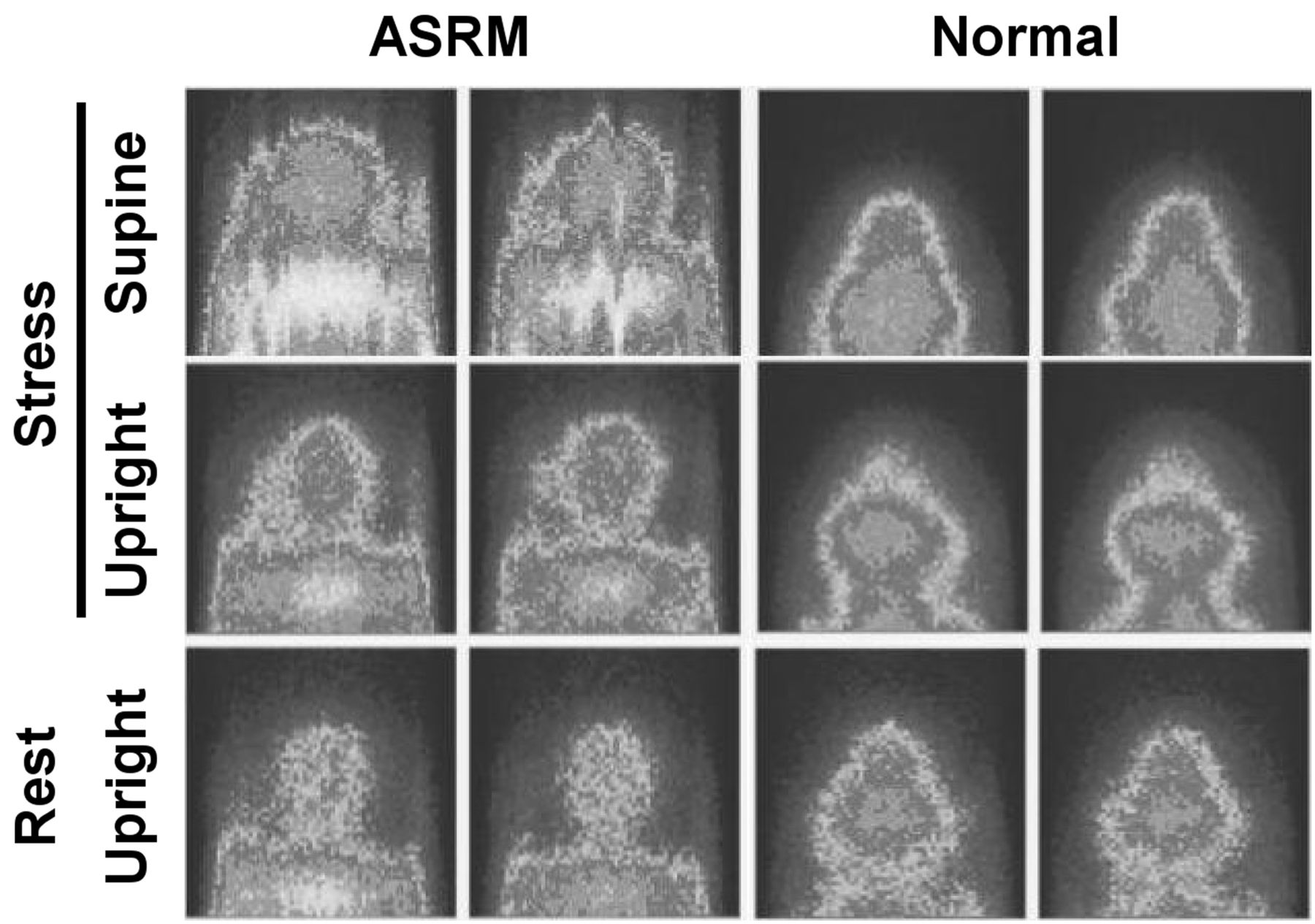
Myocardial perfusion scintigraphy (MPS) is commonly used to risk-stratify patients with suspected coronary artery disease, including preoperative assessment and post–myocardial infarction assessment (23). At our institution, MPS studies are performed on D-SPECT cameras, which incorporate 9 solid-state cadmium zinc telluride detectors surrounding the patient’s left lateral and anterior chest wall (24,25). Rest imaging is performed with the patient sitting upright, whereas stress imaging is performed with the patient both upright and supine. During the imaging, abnormal respiratory motion is seen as a sharp, vertical artifact on the imaging panogram (Fig. 1), whereas a smooth cardiac and diaphragm surface on the imaging panogram demonstrates normal quiet patient respiration. Panograms are D-SPECT quality control images that are the coronal planar projections created by the detectors to assess for vertical motion during MPS. OSA often results in abnormal respiration when patients lie supine, including snoring, apneic events, hypoventilation, and hypoxemia (5,6,26). We hypothesized that MPS patients with abnormal supine-only respiratory motion (ASRM) may be at a higher risk for OSA. The purpose of this retrospective pilot study was to determine whether the panogram portion of MPS examinations can be used as an opportunity to screen patients for OSA, a frequent comorbidity encountered in those undergoing routine MPS.

Representative images from stress supine, stress upright, and rest upright MPS panograms demonstrating abnormal ASRM results on left and normal results on right.
MATERIALS AND METHODS
The institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived.
We obtained the MPS images for 154 consecutive patients seen over the course of 1 mo at our institution. The patients were imaged using a single-day MPS protocol on a Spectrum Dynamics D-SPECT camera system. First, the rest dose was administered and then upright rest imaging was obtained. After a delay, exercise (Bruce protocol) or chemical (regadenoson) stress was performed and the stress dose was administered. Subsequent gated stress imaging was performed with the patient upright and supine. We analyzed the upright rest and upright and supine stress imaging panograms to assess for respiratory motion. Patients were characterized as having normal respiratory motion or ASRM on the basis of their panograms.
We recorded the age, sex, body mass index, and history of hypertension for each patient. Additionally, we searched for a diagnosis of OSA or use of a continuous positive airway pressure machine in the patients’ medical records. We used the same criteria cutoffs as in the STOP-BANG questionnaire (11,22). Because the study was retrospective, we could not assess snoring, reported daytime tiredness, observed apneic events, or neck circumference. We classified patients with 3 or more STOP-BANG OSA risk factors as being at high OSA risk. We used simple descriptive and frequency statistics.
RESULTS
The patient characteristics for the 154 MPS studies are detailed in Table 1. Among the patients, 42.2% were at a high risk for OSA, based on 3 or more risk factors; 16.9% had an OSA diagnosis or a prescription for a continuous positive airway pressure machine in their medical record; and 35.1% demonstrated ASRM on their MPS study.
Patient Characteristics for Total Study Population
We compared the patient characteristics for normal and ASRM MPS results and did not find any significant differences between the 2 groups (Table 2). When comparing the 2 abnormal groups—that with ASRM and that with a high number (3 or more) of OSA risk factors—we found significantly higher proportions of patients with hypertension, age greater than 50 y, and the male sex in the high-risk group than in the ASRM group (Table 3). Interestingly, we did not find any significant difference in the proportion of patients with an OSA diagnosis between the high-risk and ASRM groups (Table 3).
Comparison of Characteristics for Patients with Normal Respiratory Motion and ASRM During MPS
Comparison of Characteristics for Patients with ASRM or High (3 or More) OSA Risk Factors
Using a high number of risk factors as a standard for performing OSA screening tests, we conducted comparative statistical tests on the proposed ASRM screening test (Table 4). ASRM demonstrated a reasonable specificity and negative predictive value compared with a high number of risk factors but was less sensitive and had a lower positive predictive value.
Statistics Comparing Standard Test (High OSA Risk Factors) with Proposed Test (ASRM)
DISCUSSION
OSA is a growing problem in the developed world, with significant morbidity and all-cause mortality. In view of the pathophysiology of OSA, we hypothesized that ASRM during MPS may help screen for OSA. In this pilot study, we found that a similar proportion of patients with ASRM and patients with 3 or more OSA risk factors had a diagnosis of OSA or a prescription for a continuous positive airway pressure machine in their medical record. We propose that the MPS panogram may be a means to screen for OSA, along with the risk stratification that MPS provides for at-risk cardiac patients.
The gold standard for OSA diagnosis is polysomnography, which can be expensive and may not be available for many patients (6). Consequently, multiple questionnaires have been developed to screen for OSA, with the most sensitive test being STOP-BANG (11,16,20,22). A systematic review of multiple questionnaires demonstrated that the STOP-BANG questionnaire detected various grades of OSA severity with 90%–96% sensitivity and negative predictive values of 46%–90% (20). The same study demonstrated a stepwise-increasing probability of severe OSA with increasing STOP-BANG scores. The challenge with any of the questionnaires is the poor specificity (16,17). Because the MPS study replicates some of the physiology involved in OSA, we hypothesize that the MPS panogram screening method may improve on the specificity statistics (Table 4). If further analysis using the full STOP-BANG questionnaire or polysomnography demonstrates the validity of the MPS panogram screening method, then the questionnaire could be added to MPS patient intake forms. This approach would combine the high sensitivity of the STOP-BANG questionnaire and the reasonable specificity of the MPS panogram screening method. Similarly, if ASRM is discovered on MPS, it could prompt the interpreter to suggest further evaluation for OSA.
A key component of the proposed MPS panogram OSA screening method is the patient positioning in the D-SPECT camera, namely upright and supine. Because traditional SPECT imaging is performed with the patient supine or prone, abnormal respiratory motion in these positions may be due to several factors beyond OSA, including the chemical or physical stress mechanisms or chronic respiratory conditions. ASRM on D-SPECT imaging self-corrects for these other possibilities by changing one variable, the patient position. Abbreviated, rest-only, MPS imaging would not have the same screening effect, because it is the change of position that screens for OSA pathophysiology. Further analysis of respiratory motion on the linogram or sinogram in the traditional supine–prone or rest-only SPECT setting is needed to determine the value of the abnormal-respiratory-motion screening approach in these settings.
As a retrospective, cross-sectional pilot study, there are several limitations to this study. A few patients had an OSA diagnosis or a prescription for a continuous positive airway pressure machine in the medical record (16.9%). Future studies using the prospective gold standard of polysomnography are needed to truly assess the screening ability of MPS for OSA. In assessing OSA risk factors, only 4 of the 8 STOP-BANG questionnaire criteria were assessable; a true comparison to the questionnaire could therefore not be performed. Future studies using the full questionnaire are needed to accurately compare the screening methodologies. Only 13.6% of the patients had a body mass index greater than 35 kg/m2—a percentage that is not representative of the general population at other institutions or of the general OSA population (27,28). ASRM was recorded as a binary outcome whereas the actual ASRM severity varied among the ASRM patients; hence, future studies should compare the OSA and ASRM severity.
CONCLUSION
To our knowledge, this pilot study represents the first in the literature to look at routinely obtained MPS examinations as an opportunity to screen for OSA. When MPS is used to risk-stratify cardiac patients, the additional OSA screening feature may provide the ordering clinician with an additional metric to assist in patient management. Further studies comparing the results with both the full STOP-BANG questionnaire and polysomnography are necessary to determine the usefulness of the technique in OSA screening.
DISCLOSURE
The views expressed herein are those of the authors and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, the Department of the Air Force, the Department of Defense, or the U.S. Government. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 24, 2020.
REFERENCES
- Received for publication April 23, 2020.
- Accepted for publication May 19, 2020.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.