


Abstract
Racial and ethnic disparities in the prevalence of neurodegenerative diseases exist. This study examined the agreement between gold standard diagnosis and visual assessment of dopamine transporter (DaT) imaging in Hispanic and non-Hispanic patients being evaluated for Parkinsonian syndromes (PS). Methods: A retrospective review of DaT imaging and demographic data was performed with institutional review board approval. Documented interpretation by visual assessment was used to classify scans as normal or abnormal. The gold standard for the final diagnosis of PS was determined by a neurologist after 2 or more years of clinical follow-up. Data were analyzed with a z-test for uncorrelated samples. Results: In 30 Hispanic patients, DaT imaging was abnormal in 17, normal in 12, and nondiagnostic in 1. Of those with abnormal imaging, PS was confirmed in 16 of 17. Of those with normal imaging, no PS was confirmed in any patient. Sensitivity was 100%, and specificity was 92%. The single patient with nondiagnostic imaging was excluded. Of 77 non-Hispanic patients, visual assessment of DaT imaging was abnormal in 51. Of those with abnormal imaging, PS was confirmed in 48 of 51. Of those with normal imaging, no PS was confirmed in 22 of 26. Sensitivity was 92%, and specificity was 88%. There was no statistically significant difference (z = 0.34) in the rates of agreement between the gold standard and DaT imaging in Hispanic versus non-Hispanic patients. The study sample size afforded a power of 0.60. Conclusion: No significant difference was found in the accuracy of DaT imaging between Hispanic and non-Hispanic patients. Accuracy was high for both groups.
Parkinson disease (PD) and other Parkinsonian syndromes (PS) are neurodegenerative diseases that result from the loss of dopaminergic neurons in the nigrostriatal pathway. Clinically, PD often manifests as movement disorders characterized by the presence of tremor, rigidity, and bradykinesia on physical examination. Clinical examination alone may be insufficient to differentiate between PD and other movement disorders, such as essential tremor (1,2). In addition to the clinical findings, dopamine transporter (DaT) SPECT using 123I-ioflupane (DaTscan; GE Healthcare) aids in the diagnosis of PS by assessing the density of dopaminergic neurons in the striata (1,3–6). Use of DaT imaging further increases diagnostic accuracy in patients with suspected PS (7).
Racial and ethnic disparities in the prevalence of neurodegenerative diseases are well documented (8–11). Epidemiologic studies that examined the effect of race or ethnicity on the diagnosis of PD have thus far yielded mixed results. For example, one large study conducted on a population derived from an insurance database in Northern California found an increased incidence of PD in Hispanics (11). Another study conducted using a disease registry and Medicare claims in an urban Manhattan population found that the incidence of PD was higher for blacks than for whites or Hispanics (12). Additional studies found a higher diagnosis of PD in whites than in Hispanics or African Americans (10,13). The incidence of PD diagnoses varies by region in the United States, with higher incidences in the Midwest and Northeast (10).
The purpose of this study was to determine the rates of agreement between reference standard diagnosis and visual assessment of DaT imaging in Hispanic and non-Hispanic patients being evaluated for PS.
MATERIALS AND METHODS
Subject Population
We conducted a retrospective review of DaT imaging performed at our institution from 2011 through 2014. The institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived. Demographic and imaging data were collected from the electronic medical record. Data from 107 subjects were included in the final analysis. The subject population included 30 Hispanics and 77 non-Hispanics. The patients’ ages ranged from 31 to 88 y old; 61 women and 46 men were imaged (Table 1).
Study Population Demographics
Clinical Assessment for PS
Rest tremor most often occurs in the setting of PD or parkinsonism. The Unified Parkinson Disease Rating Scale was used to follow the longitudinal course of parkinsonism, including tremors, for patients in this study. Examinations were performed in the movement disorder clinic by neurologists specializing in movement disorders. The gold standard for the final diagnosis of PS was determined by the subject’s neurologist after 2 or more years of clinical follow-up.
Imaging Protocol
Before injection, patients were premedicated with Lugol solution to block uptake of radioiodine by the thyroid gland. Four hours after injection of approximately 185 MBq of 123I-ioflupane, projection data were obtained in a 128 × 128 matrix on a 2-head e.cam camera (Siemens Medical Systems) mounted with low-energy, high-resolution parallel-hole collimators. Projection data were acquired over 120 angles for 30 min. The standard brain protocol was used, whereby the data were reconstructed using filtered backprojection and applying a zoom of 2. As per the manufacturer’s guideline, neither attenuation nor scatter correction was applied.
Visual Reads of the Clinical Scans
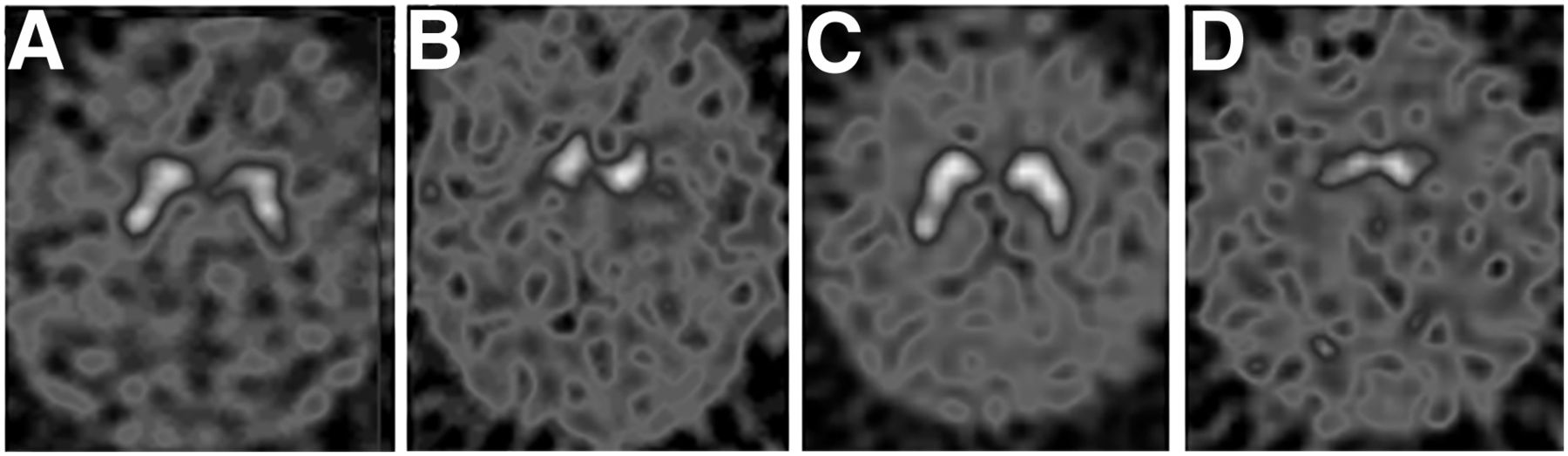
Visual reads were performed on the standard clinical images with no additional manipulation or quantification. The images were transferred to the diagnostic reading station and were read by 1 of 2 board-certified nuclear radiology physicians experienced in interpreting 123I-ioflupane images. Scans were read as having normal findings if the striata demonstrated the classic symmetric comma shapes confirming expected striatal uptake. Scans were read as having abnormal findings if there was unilateral or bilateral loss of the comma appearance consistent with abnormally reduced striatal uptake (Fig. 1).

Representative normal and abnormal 123I-ioflupane scan findings among study population ethnic groups: normal Hispanic (A), abnormal Hispanic (B), normal non-Hispanic (C), and abnormal non-Hispanic (D). Color version of this figure is available as a supplemental file at http://tech.snmjournals.org.
Data were analyzed with a z-test for uncorrelated samples using StatView (version 5.0), which provides a power analysis with each test.
RESULTS
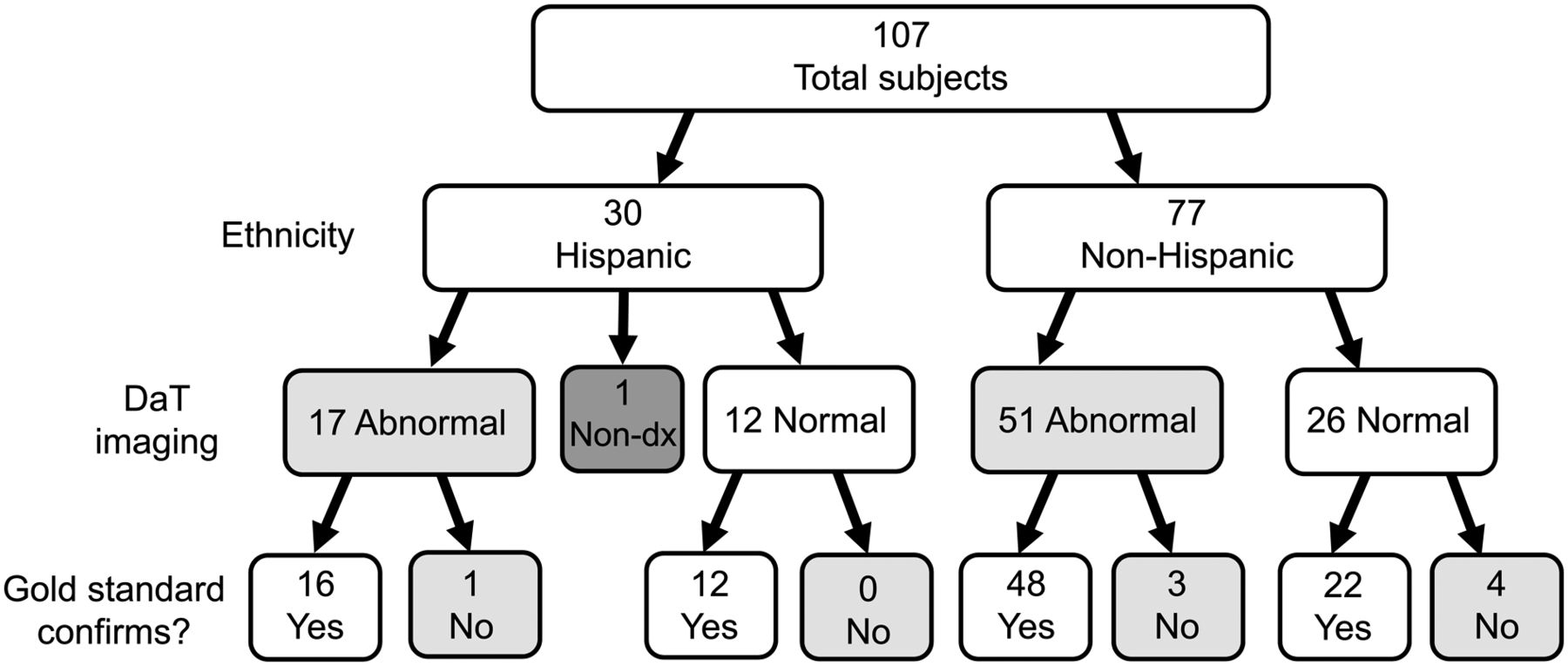
For the 30 Hispanic patients, visual assessment of DaT imaging was abnormal in 17, normal in 12, and nondiagnostic in 1 of the patients with visually abnormal DaT imaging; gold standard diagnosis confirmed PS in 16 of 17. Of the patients with visually normal DaT imaging, gold standard diagnosis confirmed no PS in any patient (12/12) (Fig. 2). Sensitivity was 100%, and specificity was 92%. Positive predictive value was 94%, and negative predictive value was 100% (Table 2). The single patient with nondiagnostic imaging was excluded from these calculations. The scan was nondiagnostic because of extreme patient motion.

Schematic of rates of agreement between gold standard diagnosis and visual assessment of DaT imaging in Hispanic vs. non-Hispanic patients. dx = diagnostic.
Rates of Agreement Between Gold Standard Clinical Diagnosis and Visual Assessment of DaT Imaging Between Hispanic and Non-Hispanic Patients
For the 77 non-Hispanic patients, visual assessment of DaT imaging was abnormal in 51 (normal in 26). Of these patients with visually abnormal DaT imaging, gold standard diagnosis confirmed PS in 48 of 51. Of the patients with visually normal DaT imaging, gold standard diagnosis confirmed no PS in 22 of 26 (Fig. 2). Sensitivity was 92%, and specificity was 88%. Positive predictive value was 94%, and negative predictive value was 85% (Table 2).
For statistical analysis, the one patient with nondiagnostic imaging was excluded. There was no statistically significant difference (z = 0.34) in the rates of agreement between the gold standard diagnosis and visual assessment of the DaT imaging in Hispanic versus non-Hispanic patients. The study sample size afforded a power of 0.60.
DISCUSSION
The initial clinical trial used to gain U.S. Food and Drug Administration approval for 123I-ioflupane was composed of a patient population that was greater than 95% Caucasian, and most of the early scientific literature validating DaT imaging came from multicenter clinical trials performed in Europe on primarily Caucasian patient populations (1,3). Disparities in racial and ethnic prevalence of neurodegenerative diseases combined with a paucity of 123I-ioflupane clinical trial data on non-Caucasian patients illustrates the need for further validation. Therefore, determining whether the accuracy of DaT imaging may vary as a function of race and ethnicity remains of interest. This study evaluated the agreement between gold standard clinical diagnosis and visual assessment of DaT imaging between the Hispanic and non-Hispanic ethnicities.
The results of our study found no statistically significant difference between Hispanic and non-Hispanic ethnicities. These results are in concordance with a large clinical trial recently conducted by GE Healthcare (ClinicalTrials.gov identifier NCT01952678), which assessed for differences between the gold standard and DaT imaging related to race (14). This GE Healthcare clinical trial compared rates of agreement between clinical diagnosis and imaging diagnosis via visual assessment in non-Caucasian and Caucasian patients with PD versus essential tremor in a study population of 102 non-Caucasians, 7 of whom were Hispanic (6.9%), and 102 Caucasians, 8 of whom were Hispanic (7.8%), finding no statistically significant difference. However, the GE Healthcare study was not designed to evaluate for any differences between Hispanic and non-Hispanic patients, given a low percentage of Hispanic patients included in the study. Furthermore, Hispanics were divided similarly between the non-Caucasian and Caucasian groups.
A limitation of our study was the small sample size, which can impact the statistical power of the results. Our power was calculated to be 0.6, with 0.8 typically being considered the standard. A larger multicenter study could likely address this issue to further support our findings of no differences. The original, standard-of-care, binary visual reads were used for clinical applicability, but using semiquantitative analyses would be an interesting future study.
Our delineation of ethnicity follows the Office of Management and Budget–issued Revisions to the Standards for the Classification of Federal Data on Race and Ethnicity, which categorized 5 races: American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, and white. There are 2 categories for ethnicity: “Hispanic or Latino” and “not Hispanic or Latino.” Hispanic or Latino is further defined as persons of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin, regardless of race.
Given the diversity among the Hispanic population around the world, our results from Hispanic patients in the Southern Arizona region may not be generalizable to all Hispanics. Further studies with a larger study cohort should be conducted to evaluate for any potential differences related to geographic and other possible factors that differ between different groups of Hispanic populations (e.g., genetic). Additionally, the current study was limited by the overall small size of the Hispanic group, although this group was, to our knowledge, the largest studied for this indication. Identification of the Hispanic participants in our study relied on their self-identification documented in the electronic medical record during routine clinical encounters, with this information typically being recorded in the demographic section of the electronic medical record. Many charts of potential participants contained no demographic information, and patients were not included in this study if demographic information was not recorded. It is unclear what factors may influence patients to self-disclose their ethnicity and whether exclusion of patients who did not self-disclose ethnicity may have impacted study results.
CONCLUSION
This retrospective analysis validates that DaT imaging with 123I-ioflupane has similarly high accuracy in both Hispanic and non-Hispanic patients.
DISCLOSURE
Phillip H. Kuo is a consultant and speaker for GE Healthcare. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 11, 2019.
REFERENCES
- Received for publication June 24, 2019.
- Accepted for publication September 6, 2019.





{kind=link}
{kind=link}