


Abstract
The skeleton is the third most common site for metastasis overall, after the lungs and liver. Accurate diagnosis of osseous metastasis is critical for initial staging, treatment planning, restaging, treatment monitoring, and survival prediction. Currently, 99mTc-methylene diphosphonate whole-body scanning is the cornerstone of imaging to detect osseous metastasis. Although 18F-sodium fluoride (18F-NaF) was one of the oldest medical tracers for this purpose, it was replaced by other tracers because of their better physical properties, until recently. Continued development of PET scanners has opened a new era for 18F-NaF, and given its higher sensitivity, there have been increasing applications in imaging. In this review, we will discuss the history, technical aspects, radiobiology, and biodistribution of this tracer. Finally, we compare the accuracy of 18F-NaF PET with other conventional imaging methods for detection of osseous metastasis.
The most common primaries for bony metastasis are breast and prostate cancers followed by pulmonary, renal, and thyroid malignancies. Appropriate diagnosis of bone metastasis is critical for initial staging, restaging, treatment monitoring, and survival prediction. Currently, whole-body scintigraphy and SPECT with 99mTc-methylene diphosphonate (99mTc-MDP) is the imaging standard for detection of osseous metastasis. 18F-sodium fluoride (18F-NaF) is a positron-emitting radiopharmaceutical used for skeletal imaging. It provides diagnostic information superior to that of 99mTc-MDP bone scans due to higher sensitivity and specificity in a wide variety of osseous metastasis (1). Combined information provided by PET and CT not only confers superiority in the characterization of malignant and benign processes but also reduces the additional imaging work-up, thus preventing diagnostic delays. Image quality, multiplanar information, and anatomic localization are further improved with the better spatial resolution of modern equipment and scanners. Previous work, including multiple case series, clinical trials, and metaanalyses, have demonstrated the advantages of 18F-NaF PET/CT for the detection, evaluation, and treatment planning of bony metastasis (2–12). In this article, we have discussed the history, technical aspects, mechanism of action, radiobiology, and comparative diagnostic performance of 18F-NaF with 99mTc-MDP bone scanning, 18F-FDG PET, CT, and MRI.
HISTORY
18F-NaF, one of the oldest radiopharmaceuticals, became standard for nuclear bone imaging in the 1960s using conventional γ-cameras, before the availability of PET scanners. In the 1970s it was largely replaced by 99mTc-labeled compounds because of their better physical characteristics (e.g., longer half-life and lower photon energy) for imaging with γ-cameras (13). 18F-NaF was initially approved by the U.S. Food and Drug Administration in 1972 for bone scintigraphy but was subsequently withdrawn in 1975 for nonclinical reasons. In the 1990s, with the advent of whole-body PET scanners, it became possible to obtain high-resolution and high-contrast imaging using 18F-NaF. This led to the return of 18F-NaF in 1993 for diagnostic imaging, followed by Food and Drug Administration approval in 2000. Progressive development, the growing availability of PET/CT scanners, and years of shortage of 99Mo–99Tc generators led to further interest in 18F-NaF. In 2011, it was approved by the Centers for Medicare and Medicaid Services under the National Oncologic PET Registry for detection of osseous metastasis (1). The registry was closed to accrual on December 14, 2017, with over 65,000 18F-NaF PET scans performed on Medicare beneficiaries (14,15). As of this writing, the Centers for Medicare and Medicaid Services is not reimbursing 18F-NaF PET/CT scans on Medicare beneficiaries. Failure of approval by the Centers for Medicare and Medicaid Services was due to the inability of various clinical studies to address the impact of 18F-NaF PET on palliative or curative care, survival, or quality of care (15). This article not only will review the superior image quality demonstrated by 18F-NaF PET but also will serve as a reference for documenting the benefits of 18F-NaF PET over bone scanning.
TECHNICAL ASPECTS
18F is produced by bombarding 18O-enriched water with high-energy protons in a cyclotron. The carrier-free 18F produced is eluted with 0.9% sodium chloride solution, resulting in formation of 18F-NaF. Once produced, the 18F-NaF is commercially available as an isotonic, sterile, colorless, pyrogen-free solution. The 18F has a half-life of 109.7 min and decays into stable 18O with ejection of a positron from the nucleus. This ejected positron annihilates with an electron, producing two 511-keV photons. PET imaging is possible because of these 2 photons, which are emitted at about 180° from one another. Whereas the 99mTc is generator-produced with a half-life of 6 h, 99mTc-MDP is manufactured by mixing 99mTc-sodium pertechnetate with commercially available MDP kits.
Patient preparation is crucial before any imaging study. Unlike 18F-FDG, 18F-NaF does not require patients to be in a fasting state; they can take all their usual medications. Good hydration and frequent urination are strongly recommended to promote tracer excretion, which results in a lower radiation dose and better image quality. With 18F-NaF, images can be obtained as early as 30–45 min after injection. However, as compared with 99mTc-MDP, the effective radiation dose for 18F-NaF is higher. For example, about a 370-MBq (10 mCi) dose of 18F-NaF delivers 8.9 mSv to an adult patient, which is approximately 70% higher than the typical 99mTc-MDP dose (16). When the accompanying attenuation correction low-dose CT is used, the effective radiation dose is usually less than 10 mSv. By convention, as with other radiopharmaceutical agents, 18F-NaF PET/CT should be avoided in pregnant patients, unless the potential benefits outweigh the radiation risk to the mother and fetus. During lactation, interruption of breastfeeding is not advisable (16,17). Thus, there are potential risks and benefits associated with administration of 18F-NaF that must be considered before patients are selected for imaging (Table 1).
MECHANISM OF ACTION AND RADIOBIOLOGY
The 18F-NaF uptake mechanism in the bones is similar to that for 99mTc-MDP but with better pharmacokinetics, faster clearance from blood, and higher uptake in the bones. 18F-NaF has minimal protein binding, which allows for a high first-pass extraction and fast soft-tissue clearance (18). Approximately 50% of the injected tracer is taken up by the bones immediately after injection (19). Uptake of 18F-NaF in a bone undergoing remodeling is 10 times that in normal bone (20). The remaining tracer is rapidly cleared from plasma and excreted by the kidneys, with only 10% of the tracer remaining in the blood after 1 h, resulting in a very high bone-to-background contrast. The low protein binding and decreased background uptake allow 18F-NaF PET scanning to be done 1 h after administration of the radiotracer, earlier than for 99m Tc-MDP scanning, which is typically 3–4 h after injection. The urinary bladder receives the highest radiation dose, followed by osteogenic cells and red marrow, respectively. 18F-NaF binds to areas of new bone formation and is a marker of blood flow and osteoblastic activity, with blood flow being the rate-limiting step for uptake (13,17). The mechanism of uptake for 18F-NaF in the bones is similar to that for 99mTc-MDP. Bone deposition occurs via chemisorption, in which the OH− ions in hydroxyapatite are exchanged for 18F− ions, converting hydroxyapatite to fluorapatite. Though the uptake mechanisms of 18F-NaF and 99mTc-MDP are similar, they exhibit differences in pharmacokinetics and radiobiology characteristics.
NORMAL BIODISTRIBUTION
The biodistribution of 18F-NaF is dependent on the differential regional blood flow and target organs (Fig. 1). The 2 primary target organs for 18F-NaF uptake are the skeleton and urinary bladder (21). Though 18F-NaF demonstrates uniform tracer distribution in bones, the non-homogeneous patterns in adults are attributable to differences in regional blood flow and bone crystal surface area. Comparatively, in children and adolescents, intense and symmetric tracer uptake can be seen in the metaphysis. Urinary washout is the major route of excretion and leads to the visualization of kidneys, ureter, and urinary bladder. The intensity of tracer in the urinary tract depends on renal function, hydration state, and the interval between tracer injection and imaging acquisition. Hyperemia in the soft tissue can cause soft-tissue uptake. Active sclerotic lesions have diffuse increased uptake. An osteolytic lesion or lesion with minimal osteoblastic reaction can show a variable level of uptake, ranging from undetectable to a rim of activity to intense uptake. However, the mechanism of uptake is not limited to neoplastic processes, as any process, benign or malignant, that causes bone remodeling and increased turnover will show increased uptake. In the past, the degree of uptake was not considered sufficient to distinguish between benign and malignant lesions. Therefore, SUVs were not routinely used in the interpretation of 18F-NaF PET/CT scans (17,18). Although there seems to be controversy on the differentiation of benign from malignant bone lesions based on SUV, several reports indicate that an SUVmax of 55–100 is concerning for a malignant process, whereas degenerative changes typically have an SUVmax of less than 50 (22–24). Also, the pattern of uptake may be characteristic or suggestive of a specific etiology, and the CT component of PET/CT is helpful in localizing and differentiating malignant from benign conditions.
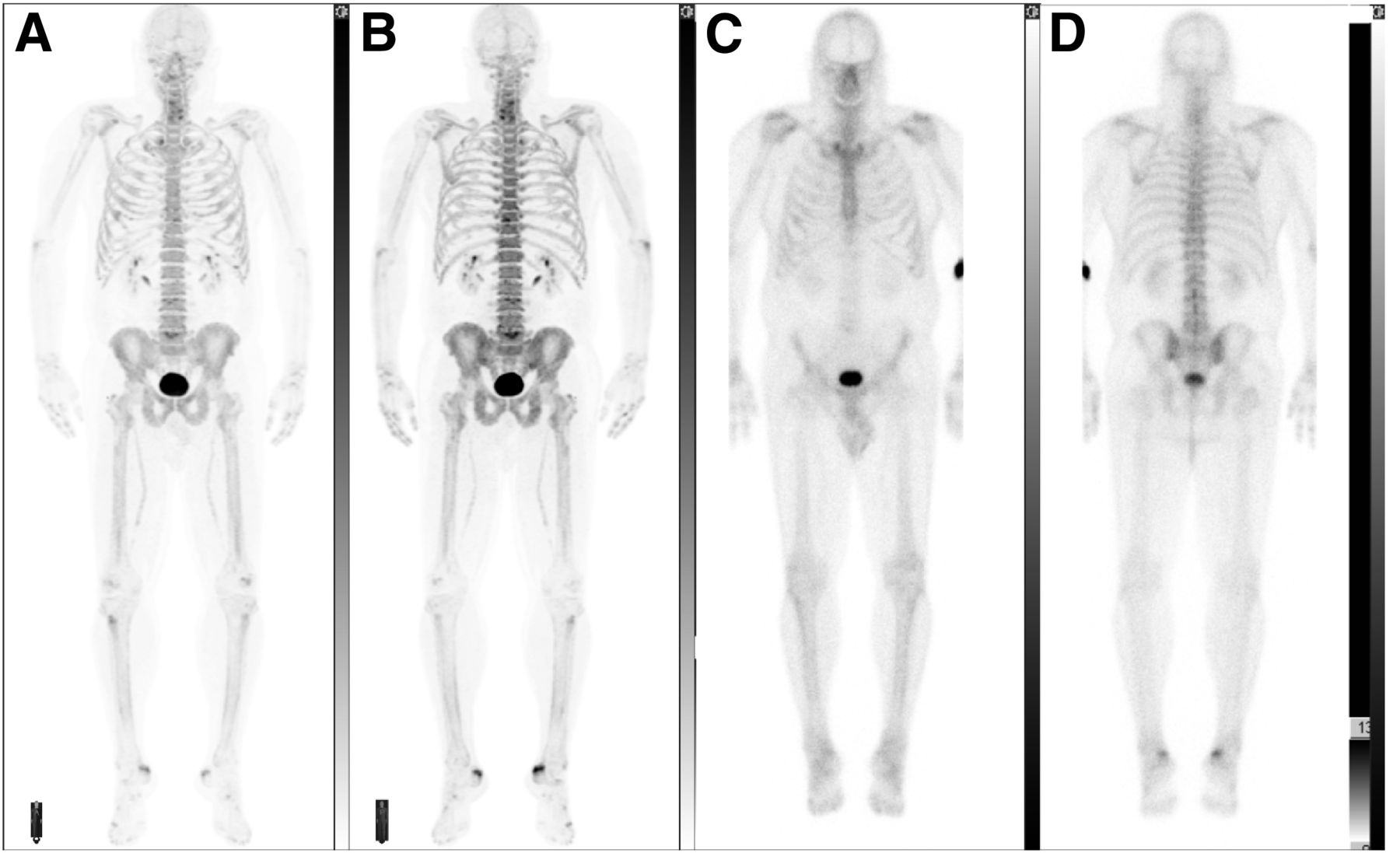
A 66-y-old man with history of prostate adenocarcinoma, seen for evaluation of bony metastasis after androgen deprivation therapy and definitive radiotherapy. (A and B) Anterior and posterior maximum-intensity projections of 18F-NaF PET scan show normal physiologic biodistribution. Mild scattered degenerative changes are seen in spine. (C and D) Anterior and posterior views of whole-body 99mTc-MDP bone scan of same patient performed 3 wk earlier show normal physiologic biodistribution. Both scans show no metastatic lesions.
The dose of 18F-NaF for PET/CT is 148–370 MBq (40–100 μCi)/kg in adults, with the maximum dose being 370 MBq (10 mCi). Given the smaller administered dose and shorter half-life of 18F-NaF, the absorbed dose of 18F-NaF is similar to that of 99mTc-MDP (17,18,21,25). Although images may be obtained as early as 30–45 min after injection of 18F-NaF, it is preferable to wait for about 1–1.5 h for better image quality. The recommended imaging protocol for 18F-NaF PET is beyond the scope of this article, and readers are referred to the protocol guideline of the Society of Nuclear Medicine and Molecular Imaging (17).
COMPARISON
18F-NaF Versus 99mTc-MDP
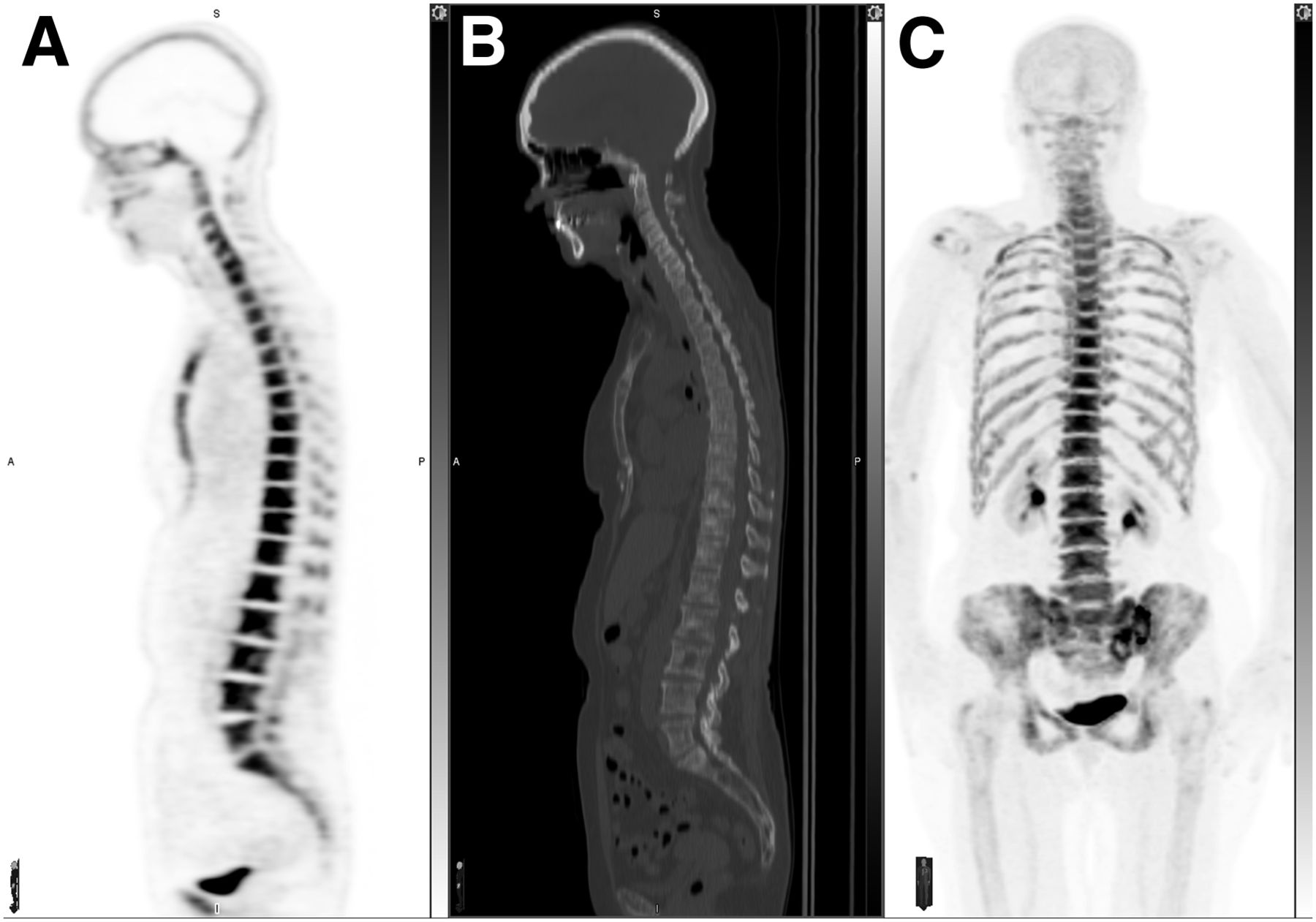
In comparison to the 99mTc-MDP whole-body scan, 18F-NaF has better image quality because of better spatial resolution (4–5 mm), higher target-to-background ratio, and higher overall sensitivity in lesion detection (17,26). The increased spatial resolution of 18F-NaF PET is especially helpful for detection of small metastases in the spine (Fig. 2).
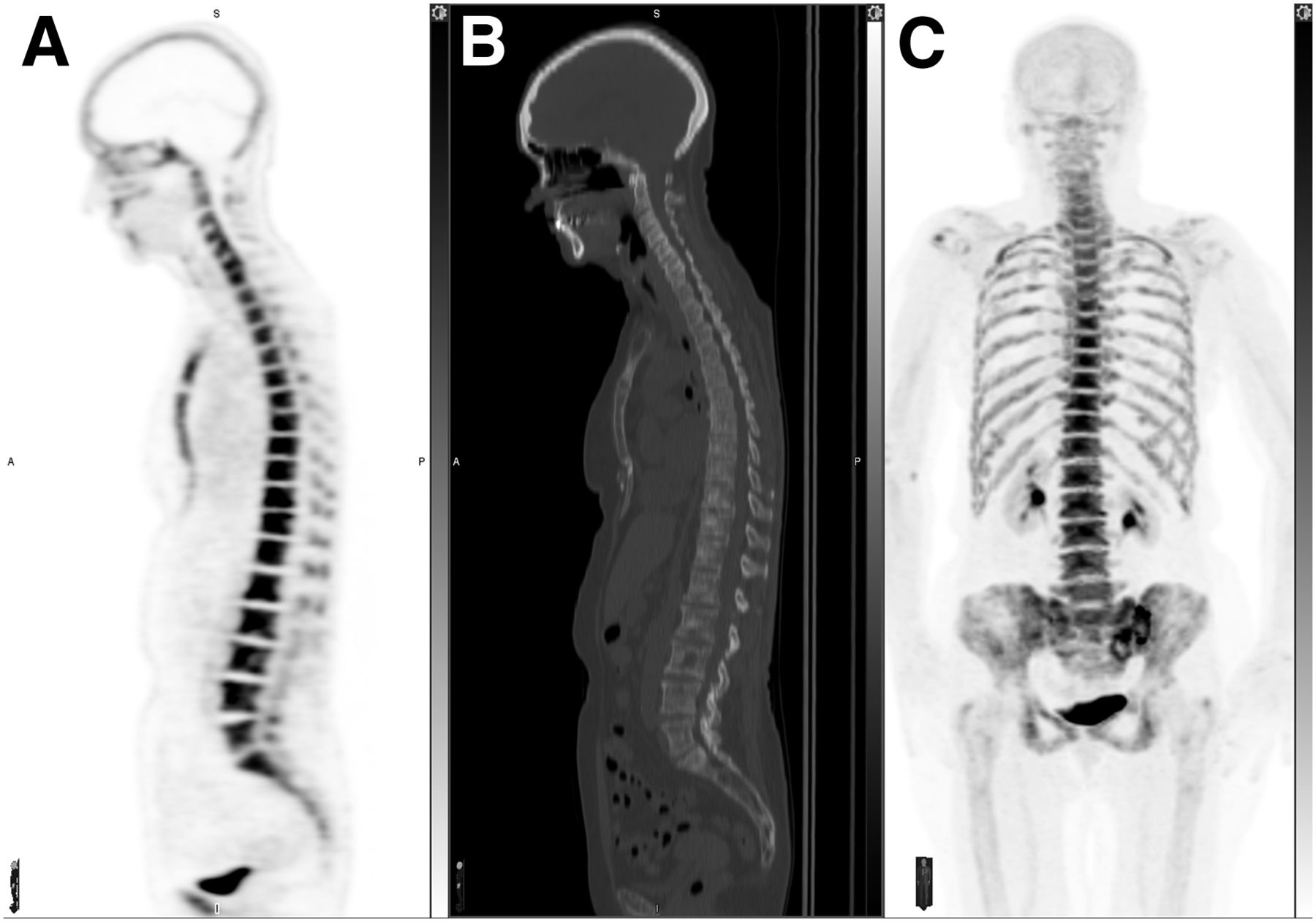
An 81-y-old woman with history of metastatic breast cancer. Sagittal 18F-NaF PET (A) and CT (B) images and anterior maximum-intensity projection (C) show diffuse sclerotic metastasis to entire spine and sternum with abnormally increased tracer uptake. Maximum-intensity projection also demonstrates abnormal uptake in ribs and pelvis.
A major diagnostic application of 18F-NaF PET scan that has been explored is its use in the detection of osseous lesions of metastatic cancers such as breast, prostate, and lung cancers. With growing research on the relevance of 18F-NaF PET in the field of oncology, it has been proven to be an important tool when compared with traditional modalities such as planar and SPECT 99mTc-MDP bone scintigraphy in assessing the extent of metastatic burden for a variety of malignancies (9–11,27–40).
There is evidence that 18F-NaF PET can be positive earlier than 99mTc-MDP whole-body bone scanning in small lytic or blastic metastases (33). A meta-analysis of various studies also compared these modalities and found 18F-NaF PET/CT to be a superior diagnostic tool, with a patient-based pooled sensitivity of 96% and a pooled specificity of 98%, as well as a lesion-based pooled sensitivity of 97% and pooled specificity of 98% (5).
A study on the evaluation of thyroid carcinoma patients for bony metastasis found 18F-NaF PET/CT to be more sensitive than planar bone scanning (12). However, a different study showed only a limited osteosclerotic bone reaction from thyroid cancer metastases on 18F-NaF PET (41).
Comparison between a standard 99mTc-based bone scan with and without SPECT to 18F-NaF PET to evaluate for vertebral osseous metastasis in lung cancer patients showed a significant difference (40). Twelve patients had vertebral metastasis, and the study showed that 18F-NaF resulted in no false-negatives whereas the bone scanning produced 6 false-negatives and SPECT produced one. Further, the results of 18F-NaF PET influenced management in 11% of the study population.
Similarly, in the evaluation of hepatocellular carcinoma by a study from Taiwan, 18F-NaF PET was found to have greater diagnostic and prognostic usefulness than 99mTc-MDP planar bone scintigraphy. 18F-NaF PET had greater accuracy on a lesion basis (95.7% vs. 75.4%, P = 0.0001) (37). Additionally, the study found a significant correlation between the presence of 18F-NaF PET/CT–positive bone lesions and overall survival, whereas such a correlation was not observed with bone scans.
Chakraborty et al. found 18F-NaF PET/CT to have a higher sensitivity, specificity, positive predictive value, negative predictive value, and accuracy in detecting bone metastases in urinary bladder carcinoma than conventional 99mTc-MDP planar bone scans (36). Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were 82.35%, 64.51%, 56%, 86.95%, and 70.83%, respectively, for 99mTc-MDP planar bone scans; 88.23%, 74.19%, 65.21%, 92%, and 79.16%, respectively, for 99mTc-MDP SPECT/CT; and 100%, 87.09%, 80.95%, 100%, and 91.66%, respectively, for 18F-NaF PET/CT. Furthermore, 18F-fluoride PET/CT changed management in 17 of 48 patients (35%).
A study on prostate cancer showed that sensitivity, specificity, positive predictive value, and negative predictive value were 70%, 57%, 64%, and 55%, respectively, for planar bone scans; 92%, 82%, 86%, and 90%, respectively, for multiple–field-of-view SPECT; 100%, 62%, 74%, and 100%, respectively, for 18F-fluoride PET; and 100% for all parameters for 18F-fluoride PET/CT (35). 18F-fluoride PET/CT was statistically more sensitive and more specific than planar or SPECT bone scans (P < 0.05) and more specific than 18F-fluoride PET alone (P < 0.001). SPECT was statistically more sensitive and specific than planar bone scans (P < 0.05) but was less sensitive than 18F-fluoride PET (P < 0.05). Also, 18F-NaF scans detected 81 more lesions, including 34 metastases that were overlooked on planar bone scans.
Another study compared 99mTc-MDP whole-body bone scans with 18F-NaF PET/CT and 18F-fluoromethylcholine PET/CT (42). Poulsen et al. found the sensitivity, specificity, positive and negative predictive values, and accuracy to be as follows: whole-body scanning: 51%, 82%, 86%, 43%, and 61%, respectively; 18F-NaF-PET/CT: 93%, 54%, 82%, 78%, and 81%, respectively; and 18F-fluoromethylcholine PET/CT: 85%, 91%, 95%, 75%, and 87%, respectively. The authors recommended combined 18F-NaF PET/CT and 18F-fluorocholine PET/CT as being accurate in this clinical setting and superior to standard bone scintigraphy. Similar results in other studies have resulted in a call for a change in practice guidelines to prefer 18F-NaF PET/CT and 11C- or 18F-choline PET/CT over 99mTc-based bone scanning for detection and monitoring of bony metastases of prostate cancer (43–45).
Growing research on metastasis detection has shown significantly better sensitivity, specificity, and diagnostic accuracy for 18F-NaF PET or PET/CT than for 99mTc-MDP bone scintigraphy (30,33,35,46). A meta-analysis based on 11 studies encompassing 425 patients to determine the diagnostic accuracy of 18F-NaF PET for detection of metastatic disease showed a sensitivity and specificity of 96.2% and 98.5%, respectively (5). Of the 425 patients analyzed on a lesion basis, 225 showed a sensitivity of 96.9% and specificity of 98.0%. Data analysis by receiver-operating-characteristic curves showed the diagnostic accuracy of PET or PET/CT to be significantly higher than that of planar and SPECT bone scintigraphy.
Although the traditionally used 99mTc-MDP bone scintigraphy has a reasonable sensitivity, the literature shows that the reduced specificity can be improved using SPECT. The accuracy of metastasis detection is further increased with the use of 18F-NaF PET/CT (47). Data indicate improved accuracy of bone lesion detection, with a high negative predictive value, for 18F-NaF PET/CT compared with 99mTc-MDP SPECT and planar 99mTc-MDP—a finding that has significant clinical implications in ruling out osseous metastatic disease with a high degree of confidence (9,29,30,40).
However, a recent study demonstrated that 18F-NaF PET/CT was unable to detect bone metastases within 24 mo of radical prostatectomy in patients with biochemical failure. The report on this study concluded that staging with 18F-NaF PET/CT does not have a superior prognostic value in patients with normal bone scan results in terms of improved patient-related outcomes after radical prostatectomy (48).
PET offers a higher resolution, and as a result, 18F-NaF PET is considered more sensitive than the traditionally used 99mTc-MDP bone scans to detect the minimal osteoblastic activity associated with lytic bone metastases (27,38,49). However, since the accumulation of fluoride is not tumor-specific, it has a reduced specificity for detection of metastatic lesions, sometimes making it difficult to differentiate them from benign bone lesions such as degenerative disease, based on the intensity of tracer uptake or SUV. Furthermore, the comparison shows 18F-NaF PET to have a significantly reduced specificity (62%) compared with 99mTc-MDP SPECT due to the increased sensitivity of PET at detecting bone lesions, which are more likely to be benign and, therefore, result in false-positive findings (47). Cancer patients who require a bone scan for metastasis evaluation are often elderly and have coexisting age-related benign bone lesions such as degenerative or arthritic bone disease. These benign bone processes share the same pattern of fluoride uptake as metastases, resulting in more false-positives than seen if evaluated by PET alone. To overcome this problem, low-dose CT is incorporated with hybrid technology, resulting in an improved specificity of 100% with 18F-NaF PET/CT (Fig. 3) (27).
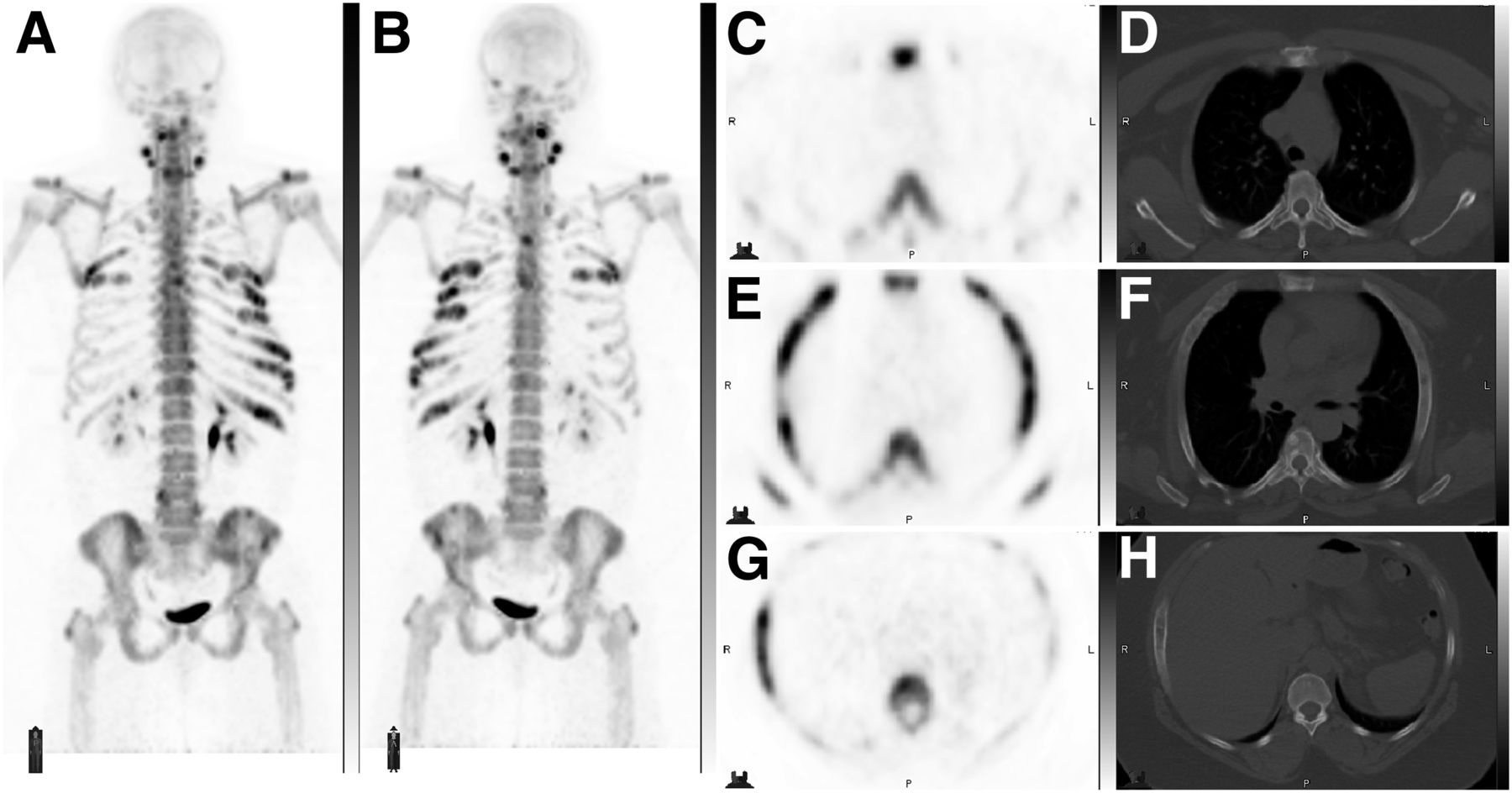
A 48-y-old woman with history of plasma cell dyscrasia. (A and B) Anterior and posterior maximum-intensity projections of 18F-NaF PET scan show multifocal areas of abnormally increased tracer uptake in spine, bilateral ribs, and mandible. (C–H) Selected axial PET and CT bone window images show expansile lesions involving bilateral ribs with ground glass density and associated abnormal tracer uptake. These lesions were stable on multiple follow-up scans and were attributable to polyostotic fibrous dysplasia.
In one prospective study with prostate cancer patients, 18F-NaF PET/CT was able to detect a higher number of bone metastases than 99mTc-MDP bone scintigraphy, with the added advantage of detection at an earlier phase. The number of lesions identified on the first 18F-NaF PET/CT scan and the interval SUV change had a direct correlation with overall survival. As per this study, an increase in SUV by 50% or more correlated with increased mortality (50). Another meta-analysis on 14 studies and 507 patients showed 18F-NaF PET/CT to be superior to 99mTc-MDP bone scintigraphy and SPECT in detecting osseous metastases during staging and restaging of high-risk prostate cancer (51).
18F-NaF PETCT is also more accurate than 99mTc-MDP bone scintigraphy for monitoring bone metastasis from prostate cancer after treatment with 223 Ra-chloride (52). 223Ra-chloride is a Food and Drug Administration–approved α-emitter used in patients with castration-resistant prostate cancer with bony metastases (53). Also, in a study on a small patient population, 18F-NaF PET was superior to 99mTc-MDP whole-body bone scans for evaluation of treatment response in bone metastasis (54).
In conclusion, the literature indicates that 18F-NaF uptake occurs in osteolytic metastasis as well as osteoblastic metastasis (49,55).
18F-NaF Versus CT and MRI
Piccardo et al. studied 39 women with breast cancer with bone metastasis and reported that the sensitivity of detection was significantly better for 18F-NaF PET/CT than for CT alone (91% and 77%, respectively) (27). However, the specificity of 18F-NaF PET/CT was 91% whereas CT had a specificity of 93%. It has been shown that 18F-NaF PET/CT is superior to contrast-enhanced and non-enhanced chest, abdomen, and pelvis CT and to 99mTc-MDP bone scans for the detection of occult bone metastasis in patients with prostate cancer (56).
In addition, 18F-NaF PET is a useful tool to detect iatrogenic disorders such as bisphosphonate-induced osteonecrosis of the jaw. Current modalities for assessment, such as contrast-enhanced MRI and cone-beam CT, have been proven less accurate for this condition (57).
A study by Poulsen et al. used MRI as a gold-standard reference for the detection of bone metastasis in prostate cancer patients. They reported that 114 lesions not detected by MRI were picked up by one or more of the modalities, including whole-body bone scintigraphy, 18F-NaF PET/CT, and 18F-fluoromethylcholine PET/CT. Of these, the most sensitive was 18F-NaF PET/CT, with 68 lesions, whereas 10 lesions were detected by both 18F-NaF PET/CT and 18F-fluoromethylcholine PET/CT (42).
A meta-analysis of 14 studies and 507 patients reported 18F-NaF PET/CT to have a diagnostic performance comparable to that of diffusion-weighted MRI (51). However, more recent studies have shown significantly better sensitivity, specificity, and overall accuracy than for diffusion-weighted MRI (58,59).
18F-NaF Versus 18F-FDG
A published study comparing the detection of bone metastasis by 18F-NaF PET/CT and 18F-FDG PET/CT in head and neck cancer patients at high risk for metastasis found the 2 modalities to have comparable lesion-based sensitivities of 69.4% and 57.1%, respectively, with a P value of 0.126 (60). They also had similar areas under the curve of 0.7561 versus 0.7959 (P = 0.149). When combined, 18F-NaF PET/CT and 18F-FDG PET/CT demonstrated a significantly better lesion-based sensitivity than that for a single modality (P < 0.001). However, a similar advantage was not observed in patient-based analysis, and therefore, their combined use is not advised (61).
Krüger et al. studied 126 non–small cell lung cancer patients and reported a comparison of 18F-NaF PET with 18F-FDG PET/CT for detection of bone metastasis (10). They found concordant metastases diagnosed in 13 of 18 patients. Interestingly, 18F-FDG PET/CT detected a higher absolute number of bone metastases than 18F-NaF PET (73 vs. 55, P < 0.05). However, 18F-NaF PET diagnosed more patients with bone metastases, in that 4 patients showed positive findings on 18F-NaF PET but negative findings on 18F-FDG PET/CT.
Iagaru et al. compared 18F-NaF and 18F-FDG PET/CT for detection of skeletal metastasis in 52 patients (11). They reported 18F-NaF PET/CT to have superior detection of skeletal metastatic disease (24 vs. 16) as well as better image quality. However, the study also showed that extraskeletal metastasis detection by 18F-FDG PET/CT could alter management. Therefore, a combined approach to disease evaluation was suggested. Iagaru et al. conducted another study to test a combination of 18F-NaF PET/CT and 18F-FDG PET/CT as an imaging modality for cancer patients (61). They reported that the combined approach missed none of the lesions detected by 18F-FDG PET/CT and only one skull lesion detected by 18F-NaF PET/CT alone.
A recent retrospective study comparing 18F-NaF PET/CT and 18F-FDG PET/CT in detection of skull-base invasion and bony metastases in nasopharyngeal cancer detected more osseous metastases and had a more accurate assessment of skull-base invasion on 18F-NaF PET/CT than on 18F-FDG PET/CT. For detecting skull-base invasion, 18F-NaF PET/CT had a sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of 100%, 94.7%, 97.8%, 96.3%, and 100%, respectively, whereas for 18F-FDG PET/CT these measures were 65.4%, 100%, 80%, 100%, and 67.9%, respectively. The sensitivity and specificity for detecting bone metastatic lesions were 98.3%, and 65.7%, respectively, for 18F-NaF PET/CT and 42.9%, and 97.1%, respectively, for 18F-FDG PET/CT (Table 2) (62).
Studies Comparing 18F-NaF with Other Radiotracers
Studies comparing 18F-NaF PET/CT and 18F-FDG PET/CT in multiple-myeloma patients found only a 39% correlation for disease assessment, with 343 and 135 lesions picked up by 18F-NaF PET/CT and 18F-FDG PET/CT, respectively (63). Interestingly, 3 patients who showed multiple focal lesions on 18F-FDG PET/CT had no identifiable lesions on 18F-NaF PET/CT. In addition, evaluation of the pelvic area with 18F-NaF and 18F-FDG PET/CT demonstrated 24 and 77 lesions, respectively.
In one prospective study on patients with prostate and breast cancers, 18F-NaF/18F-FDG PET/CT was superior to whole-body MRI and 99mTc-MDP scintigraphy for detection of bone metastasis. The performance of 18F-NaF/18F-FDG PET/CT was similar to a combination of whole-body MRI and bone scintigraphy (Fig. 4) (64).

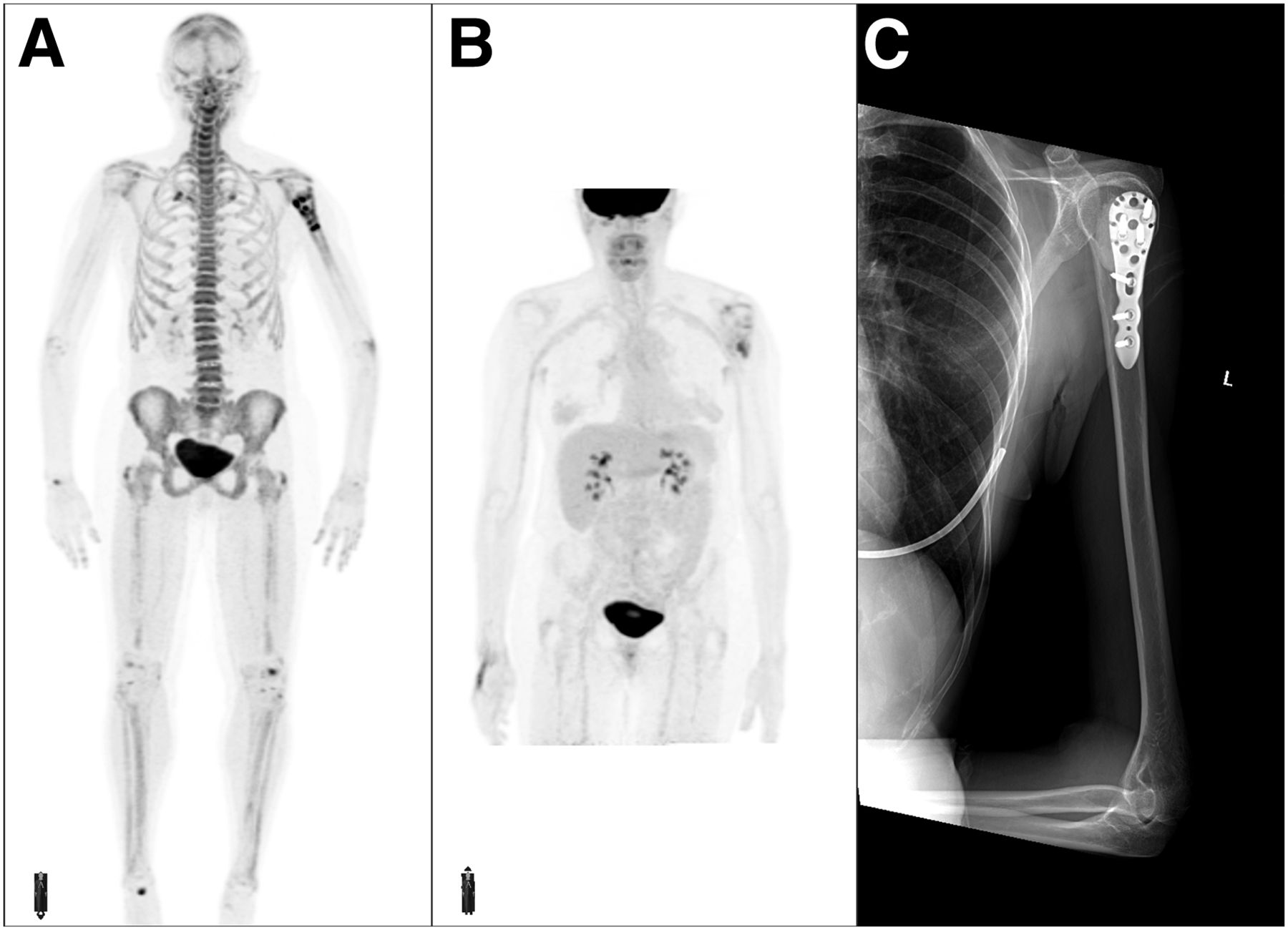
A 58-y-old woman with history of metastatic colorectal cancer, seen after radiation therapy and placement of fixation hardware for lytic metastasis to left proximal humerus. Anterior maximum-intensity projection of 18F-NaF (A) and 18F-FDG (B) PET scans shows heterogeneously increased tracer uptake in left proximal humerus secondary to bone remodeling. No other area of abnormal tracer activity is seen elsewhere. (C) X-ray of left humerus shows cement and fixation hardware.
CONCLUSION
Detection of bony metastases in patients with malignancy is a matter of high clinical importance as it can significantly impact treatment and outcome. 18F-NaF PET has shown excellent diagnostic performance in the detection of bone metastases. Through advancements in PET scanners in recent decades, 18F-NaF PET is now feasible and its radiation dose is comparable to a conventional 99mTc-MDP bone scan. By having a better spatial resolution, better image quality, higher target-to-background contrast, and higher sensitivity, 18F-NaF PET is superior to a conventional 99mTc-MDP bone scan. It has also shown superiority to other imaging modalities, including CT, MRI, and 18F-FDG PET/CT. The challenge posed by the low specificity of this modality has been partially solved by using simultaneous anatomic imaging as a part of PET/CT or PET/MRI. Further, the development of new scanners and reconstruction methods will make it possible to perform 18F-NaF PET with a much lower dose. Currently, 18F-NaF PET/CT scans are not being reimbursed by the Centers for Medicare and Medicaid Services, and additional prospective studies are needed to demonstrate the clinical impact of 18F-NaF PET/CT in various malignancies.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 6, 2019.
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than March 2023. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
REFERENCES
- Received for publication July 31, 2019.
- Accepted for publication October 30, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}