


Abstract
At a time when reducing the radiation dose to patients and the public has become a major focus, we assessed the radiation exposure rate from patients after an 18F-FDG PET/CT scan and evaluated different interventions to reduce it. Methods: We enrolled 100 patients, divided into 2 groups. For both groups, the radiation dose rate was measured with an ionization survey meter immediately after the scan. For group 1, the patients then voided and their dose rate was measured again. For group 2, the patients waited 30 min before voiding, and we measured the dose rate before (group 2A) and after (group 2B) they voided. Results: In total, 74 of the 100 patients exceeded the 20 μSv/h (2 mR/h) threshold immediately after the scan. In group 1, the mean dose rate decreased by 20.0% from the postscan measurement, with 12 of 36 remaining at or above 20 μSv/h. In group 2A, the mean dose rate decreased by 23% from the postscan measurement, with 9 of 38 remaining at or above 20 μSv/h. In group 2B, the mean dose rate decreased by 35% from the postscan measurement, with 1 of 38 remaining at 20 μSv/h. Conclusion: Nearly 75% of patients undergoing an 18F-FDG PET/CT scan exceed 20 μSv/h when leaving the imaging facility. The most effective method to reduce radiation exposure was to have the patient void 30 min after the examination.
The increased use of diagnostic imaging throughout the world has caused a drastic increase in the radiation exposure of the population and has raised concerns about potential cancer risks associated with this trend, as well as unfavorable media coverage (1,2). PET/CT has emerged as the gold standard to stage and restage various types of malignancies, while also seeing a steady incline in the number of studies performed. These patients are receiving not only radiation from the CT component of the examination but also lingering radiation from the radiopharmaceutical, 18F-FDG. Compared with CT and radiography, both nuclear medicine and PET/CT studies inherently expose the general public to additional radiation due to the administration of radiopharmaceuticals. This concern has led to various new techniques and has paved the way for technologic advancements to both improve image quality and simultaneously reduce the radiation to which a patient is exposed.
The Nuclear Regulatory Commission has well-established guidelines for the release of patients undergoing therapeutic procedures (3). The maximum accepted exposure of the public from a material source—20 μSv/h (2 mR/h)—is used as a benchmark to reduce exposure to as low as reasonably achievable (4). However, guidelines addressing the release of a patient undergoing diagnostic nuclear medicine or PET/CT examinations are not as clear. Nevertheless, medical facilities are under increased scrutiny to reduce the radiation exposure of both patients and the public.
Although the half-life of 18F-FDG is relatively short (110 min), many patients have multiple tests and clinical appointments in a single visit. It is therefore important to consider the time frame immediately after a scan. At a time when reducing the radiation dose to patients and imaging staff has become a major focus, this study set out to explore the effectiveness of reducing the radiation exposure of the public from a patient who received a standard-of-care 18F-FDG PET/CT examination. We sought a low-cost solution with the least impact or inconvenience to the patient and the PET/CT department. In addition, renal function was evaluated as a potential variable affecting this exposure. As proof of principle, we also evaluated the difference in radiation exposure between a small group of patients undergoing 18F-fluciclovine PET/CT, with an imaging time of 3–5 min after injection, and patients undergoing 18F-FDG PET/CT, with an imaging time of 60 min.
MATERIALS AND METHODS
This project was undertaken as a quality improvement initiative. The members of the Institutional Review Board reviewed this study and determined it did not need approval under their guidelines.
Patients undergoing standard-of-care 18F-FDG PET/CT examinations who were willing to be included in our measurements were enrolled in the study until the total reached 100 patients (61 men and 39 women; mean age, 54 y). The patients received a weight-based 18F-FDG dose (range, 233.1–558.7 MBq [6.3–15.1 mCi]; mean, 421.8 MBq [11.4 mCi]), which was followed by an approximately 60-min uptake time (range, 51–93 min; mean, 62 min). They were then instructed to void immediately before a standard-of-care whole-body PET/CT acquisition (acquisition time range, 14–47 min; mean, 26 min). After the scan, each patient was then measured with an ionization survey meter (Victoreen ion chamber survey meter, model 450; Cardinal Health, Inc.) placed 1 m from the patient. A dedicated area within the hospital was used for measurement to ensure consistency. All measurements were performed by the same technologist, with the survey meter aimed at the bladder. Patients were randomly divided into 2 groups of 50 patients each based on availability after the PET/CT examination. For both groups, the radiation dose rate was measured with an ionization survey meter immediately after the scan. For group 1, the patients then voided and their dose rate was measured again. For group 2, the patients waited 30 min before voiding, and the dose rate was measured before (group 2A) and after (group 2B) they voided. Consideration of renal function was also investigated; renal function data and estimated glomerular filtration rate values within 2 wk of the scan were available for 77 of the 100 patients.
A small sample of 12 men (mean age, 62 y) undergoing standard-of-care 18F-fluciclovine PET/CT for biochemically recurrent prostate cancer was also evaluated. Although the 18F dose was comparable, the difference in protocols between the 18F-fluciclovine and 18F-FDG patients was assessed (3–5 vs. 60 min). All patients received the standard 370-MBq (10-mCi) dose, and images were acquired 3–5 min afterward. On completion of imaging, each patient was measured with the ionization survey meter in the same way as for the 18F-FDG PET/CT scans. Patients were instructed to wait 30 min and dose rates were remeasured. Each patient was then instructed to void, and the final dose rates were measured.
RESULTS
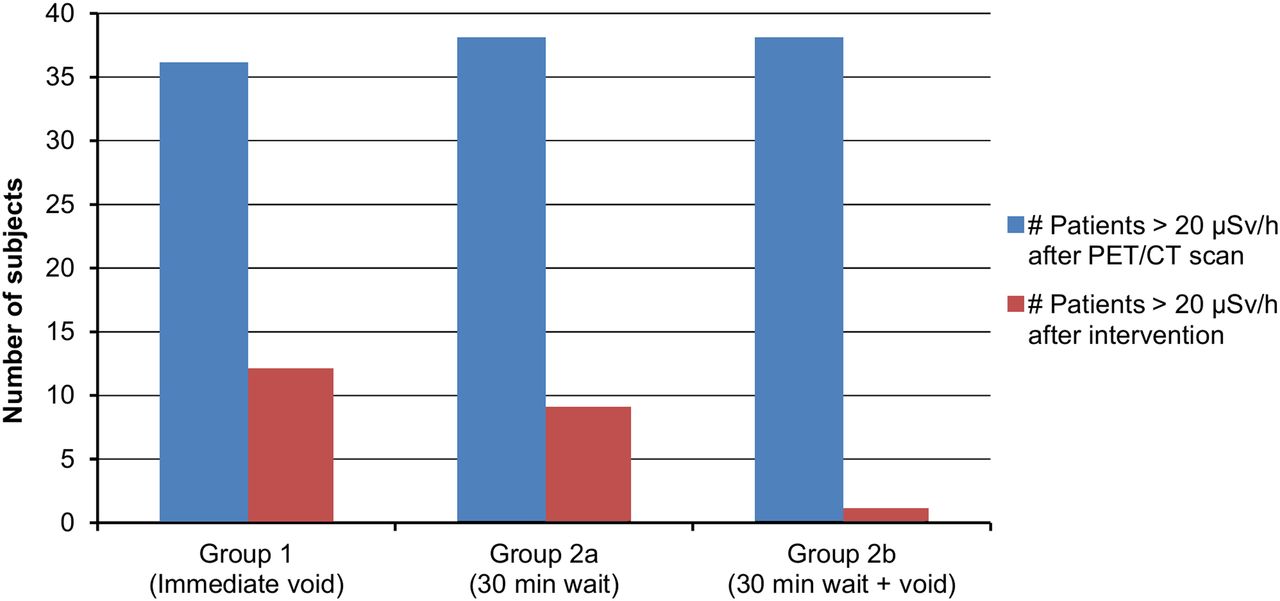
In total, 74 of the 100 patients (74%) exceeded 20 μSv/h (2 mR/h) at 1 m immediately after their PET/CT scan. Of these, 36 (49%) were from group 1 and 38 (51%) were from groups 2A and 2B. In group 1, the mean dose rate decreased by 20.0% (from 23 to 18.3 μSv/h) from the postscan measurement, with 12 of 36 (33%) remaining at or above the 20 μSv/h threshold. In group 2A, the mean dose rate decreased by 23% (from 23.4 to 18 μSv/h) from the postscan measurement, with 9 of 38 (24%) remaining at or above 20 μSv/h. In group 2B, the mean dose rate decreased by 35% (from 23.4 to 15.1 μSv/h) from the postscan measurement, with 1 of 38 (3%) remaining at 20 μSv/h (Fig. 1).

Comparison of patients above 20 μSv/h threshold measured immediately after PET/CT scan vs. patients above 20 μSv/h after various interventions to reduce radiation exposure.
Of the 77 patients with renal function data, only 12 (16%) had reduced renal function (estimated glomerular filtration rate < 60). Of these, 11 (92%) were above 20 μSv/h immediately after the scan, whereas 47 (72%) of the 65 patients with normal estimated glomerular filtration rate were above 20 μSv/h after the scan (Fig. 2). The data suggest that patients with reduced renal function have higher radiation exposure than those with normal renal function. However, this difference was not statistically significant, with a P value of 0.274.
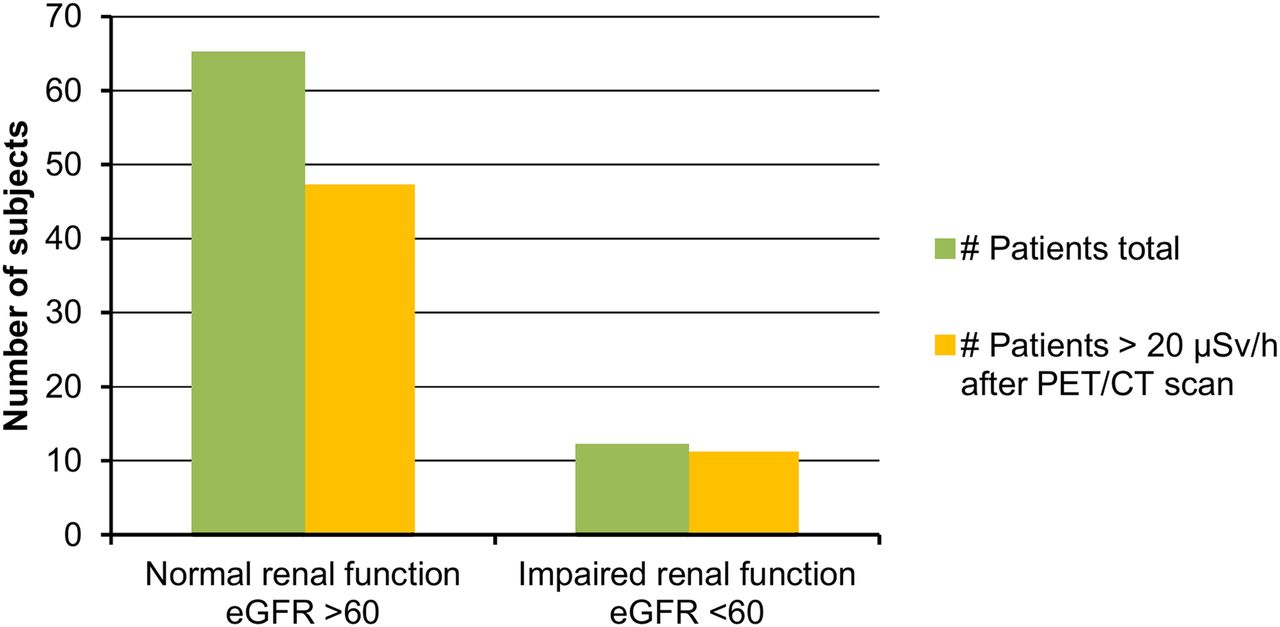
Comparison of patients with normal estimated glomerular filtration rate (eGFR) vs. patients with abnormal eGFR. Shown are total patients in each group based on eGFR, as well as patients above 20 μSv/h threshold immediately after imaging.
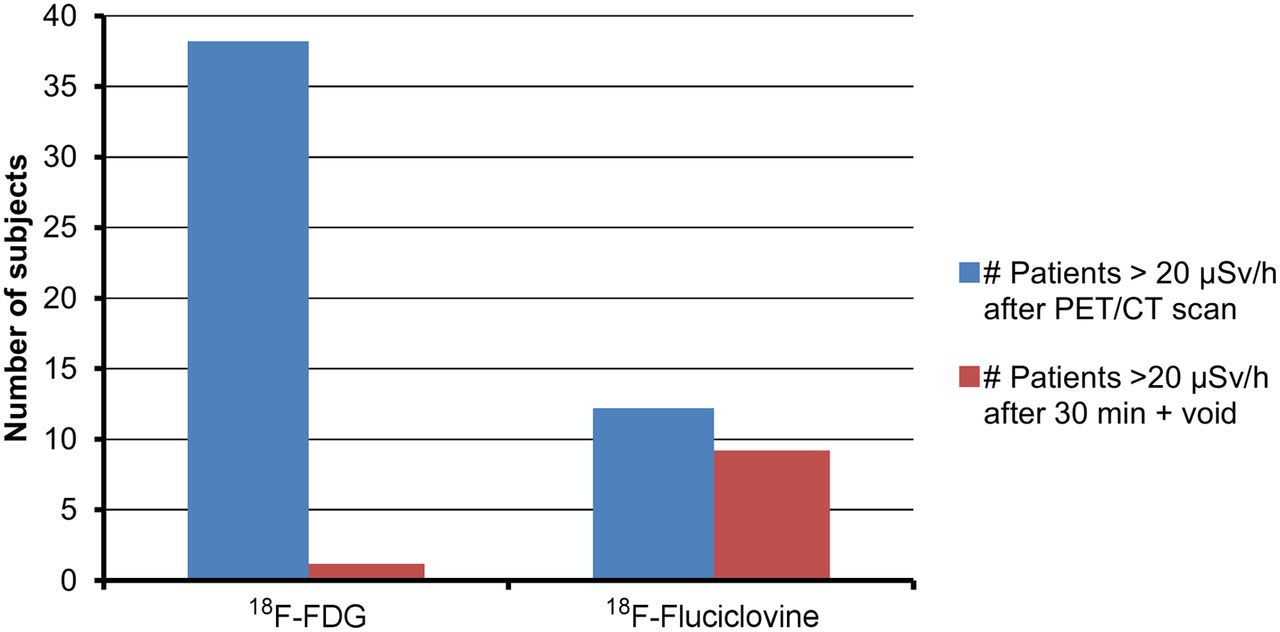
Of the 12 patients undergoing 18F-fluciclovine PET/CT, 12 (100%) remained at or above 20 μSv/h immediately after the scan. After a 30-min wait, the mean exposure decreased by 25% (from 28.2 to 21.2 μSv/h), but 9 patients (75%) remained at or above 20 μSv/h. After a 30-min wait followed by voiding, the mean exposure decreased by 30% (from 28.2 to 19.8 μSv/h), but 9 patients (75%) remained at or above 20 μSv/h. When comparing the most effective intervention—waiting 30 min plus voiding—between the 18F-FDG and 18F-fluciclovine studies, we found that 97% (37/38) of the 18F-FDG patients who initially exceeded 20 μSv/h fell below that threshold, compared with only 25% (3/12) of the 18F-fluciclovine patients (Fig. 3).

Comparison of radiation exposure from patients undergoing 18F-FDG PET/CT scan vs. 18F-fluciclovine PET/CT scan. Shown are number of patients exceeding 20 μSv/h threshold immediately after scan, as well as number of patients continuing to exceed 20 μSv/h after waiting 30 min and then voiding.
DISCUSSION
The ever-expanding use of diagnostic imaging continues to raise concerns about the increased cancer risk from ionizing radiation exposure. This issue has been especially critical for children and young adults. Multiple media reports have surfaced describing the increased cancer risk from medical imaging examinations. During this same period, the use of diagnostic imaging has been increasing at a steady pace. Although the natural background radiation has not significantly changed, the radiation exposure from medical imaging has increased more than 6-fold. According to a report issued in March 2009 by the National Council on Radiation Protection and Measurements, medical imaging contributed about 15% of the overall radiation dose in the United States in the 1980s, compared with about 50% in 2006 (5). The use of PET/CT in the clinical setting has also been expanding with the advancement of medicine and technology. The number of PET/CT systems increased over 10-fold since 2001, and the number of clinical scans performed in the United States alone is estimated at nearly 2 million, which is an increase of 13% over 2015 (6,7).
The concerns about exposure of the public to ionizing radiation from medical imaging have brought about a movement in both the pediatric population with the Image Gently campaign and the adult population with the Image Wisely campaign. To maximize the risk-to-benefit ratio, the medical community attempts to optimize diagnostic image quality while at the same time following the as-low-as-reasonably-achievable principle. The Image Gently and Image Wisely campaigns were developed to educate both providers and consumers in an attempt to curtail unnecessary imaging and reduce radiation exposure (8–10). However, there continues to be debate on whether low-dose radiation exposure can cause cancer (11). In a recent publication, Siegel et al. made the case for terminating these campaigns because of the erroneous extrapolation of the linear no-threshold model from high- to low-dose radiation as well as propagation of radiophobia. The linear no-threshold model for radiation-induced cancer has guided radiation protection policies since the 1950s and is supported by national and international advisory bodies. It is based on the concept that low levels of radiation increase mutations, which lead to increased cancers. However, Siegel et al. claim that low-dose radiation may even help prevent cancer by inducing repair of preexisting and ongoing DNA damage while repairing radiogenic damage (12–15). Nevertheless, from the regulatory standpoint, the linear no-threshold model is accepted and continues to be supported by national advisory bodies (National Research Council and National Council on Radiation Protection and Measurements) (16,17). Furthermore, those questioning the linear no-threshold model are basing the risk versus benefit on only the patient. This point of view should not be the same for the general public or potentially vulnerable patient populations in hospital or clinic waiting areas. It has been shown that the cancer risk increases substantially in patients with a suppressed immune system such as in young AIDS patients, for whom the cancer incidence increases by a factor of 40, or in young organ-transplant patients, for whom the cancer mortality rate increases by a factor of 60 (18,19). Nonetheless, a balance needs to be made between radiation risk and radiation aversion.
Various techniques have been developed to decrease the level of radiation exposure by using weight-based protocols for both the radiopharmaceutical delivered and the CT scan. Furthermore, PET/CT systems with higher sensitivity and improved performance can take advantage of enhanced detector technology (better time-of-flight performance, continuous bed motion, or an extended axial field of view) to reduce the 18F-FDG dose (20,21). According to the Society of Nuclear Medicine and Molecular Imaging guidelines, the typical administered 18F-FDG dose is 370–740 MBq (10–20 mCi) (22). However, patients who weigh more than 75 kg should receive a slightly higher dose to compensate for degraded image quality due to a lower signal-to-noise ratio from excessive attenuation (20).
Although these advancements and techniques address the radiation exposure of patients and radiation workers, they do not address the exposure of the public to patients or the repeated exposure of unmonitored nonradiologic medical staff to patients. Many patients schedule multiple tests and clinical appointments on a single day, exposing not only other patients in waiting areas but also general medical personnel. Multiple studies have been performed to assess the amount of radiation received by medical personnel in various roles (23). Regardless of the validity of the linear no-threshold model, there is justification for the radiation exposure of both patients and radiation workers; however, the same cannot be said for the general public.
Our study evaluated simple noninvasive interventions to reduce the overall radiation exposure of the public with no additional cost and only an additional 30-min wait for the patient before being released after imaging. At a time when the Nuclear Regulatory Commission has strict guidelines on the release of a patient treated with a radioisotope, the recommendations about releasing a patient undergoing diagnostic PET/CT are not as clear. In addition, national and international guidelines (Society of Nuclear Medicine and Molecular Imaging, American College of Radiology, and European Association of Nuclear Medicine) neither give recommendations for radiation exposure from patients nor recommend voiding or waiting after a scan before release (20,22,24). Although our data on the reduced radiation exposure after voiding were similar to prior studies, we found that nearly 75% of patients undergoing an 18F-FDG PET/CT scan leave the imaging facility exceeding 20 μSv/h at 1 m (25). We also attempted to address the concern about reduced renal function in these patients. Although renal failure has been shown not to have a significant impact on 18F-FDG biodistribution in PET/CT, our initial data showed a possible correlation between impaired renal function and elevated radiation exposure (26). However, because of our small sample size, this correlation was not statistically significant.
Moreover, the initial data from patients undergoing a 18F-fluciclovine study showed that they exposed the public to a higher level of radiation than did patients undergoing an 18F-FDG study. The higher exposure is most likely due to the elimination of the 60-min uptake phase, given the different pharmacodynamics. Sörensen et al. demonstrated that tumor uptake of 18F-fluciclovine peaks at around 3 min, with a plateau from 3 to 12 min and gradual washout. Lymph node uptake was rapid, with washout even faster than from tumor, and the urinary bladder had gradual uptake (27). Therefore, standard imaging with 18F-fluciclovine is performed 3–5 min after radiotracer administration, compared with 60 min with 18F-FDG (28). Although the 18F isotope is the same in both the 18F-fluciclovine and the 18F-FDG studies, as well as there being a similar injected dose—370 versus 421.8 MBq (10 vs. 11.4 mCi)—the difference in the protocol with 18F-fluciclovine requires a significantly shorter uptake phase. In our study, this difference caused 75% of the 18F-fluciclovine patients to remain above the 20 μSv/h threshold after waiting 30 min plus voiding, versus only 3% for the 18F-FDG patients.
This study may be the first to evaluate the radiation exposure of the public to a patient undergoing an 18F-FDG PET/CT scan and to assess the feasibility of implementing simple interventions to significantly reduce that exposure. Other studies have addressed radiation exposure but in the context of exposure to a patient or technologist (25,29). In addition, the effects of voiding after imaging to reduce exposure have also been studied, but not the combination of waiting plus voiding. In theory, these principles can also be used for other diagnostic PET and nuclear medicine studies before a patient leaves an imaging facility.
Our study is not without limitations. The relatively small sample size limits the statistical significance of the findings, especially when evaluating the effect of renal impairment. A larger sample size could allow for evaluation of various stages and severities of renal disease. Additionally, only 12 patients undergoing an 18F-fluciclovine study were evaluated. Other commonly used Food and Drug Administration–approved PET tracers such as 18F-sodium fluoride and 68Ga-DOTATATE should also be evaluated. We found that even the same isotope can expose the public to vastly different levels of radiation, depending on the protocol. Lastly, this study was limited to the experience of a single institution with a fixed scanner. Because of financial concerns, a fixed PET/CT scanner is not always cost-effective and a mobile PET/CT scanner is often used. However, given the space and time constraints of a mobile scanner, these simple interventions may not be feasible. A prospective multiinstitute study would be better able to assess different patient populations, radiotracers, and protocols and to compare both fixed and mobile facilities.
CONCLUSION
Current guidelines do not advocate measuring the radiation level emanating from patients before they are released after undergoing 18F-FDG PET/CT. Our analysis shows that this level exceeds the 20 μSv/h threshold in nearly 75% of patients after 18F-FDG PET/CT and in all patients after 18F-flucicolvine PET/CT. For 18F-FDG, the most effective method to reduce this level was to have the patient wait 30 min after the examination and then void, with 97% of patients then being below the threshold. This simple intervention is especially important when patients have additional appointments and are in close contact with others. However, this intervention was not as effective for 18F-fluciclovine, dropping only 25% of patients below the threshold. Therefore, more effective techniques should be developed and validated for non–18F-FDG PET/CT scans.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 11, 2019.
REFERENCES
- Received for publication July 2, 2019.
- Accepted for publication August 21, 2019.





{kind=link}
{kind=link}
{kind=link}