


Abstract
18F-fluciclovine PET is approved for prostate cancer recurrence imaging. According to the radiopharmaceutical package insert, only 3% of the tracer is expected to be excreted in the urine over the first 4 h. Yet, in clinical practice we noticed a higher percentage of bladder excretion. We sought to evaluate and quantify early 18F-fluciclovine bladder radioactivity and determine whether refraining from voiding before 18F-fluciclovine injection would mitigate it. Methods: In total, 159 patients underwent 18F-fluciclovine PET/CT imaging as part of their clinical workup. The first 36 patients were instructed to void just before 18F-fluciclovine injection; the subsequent 123 patients were not asked to void. The SUVmax and SUVmean of the bladder, aorta, marrow, liver, and bladder volumes were determined. Comparing SUVmean of bladder to background, we characterized bladder radioactivity as insignificant (bladder < aorta), mild (bladder > aorta < marrow), moderate (bladder > marrow < liver), or intense (bladder > liver). Differences between the protocols were investigated. Results: Overall, 22% (35/159) of patients had moderate bladder activity and 8.8% (14/159) had intense bladder activity. A negative association was found between bladder volume and SUVmean. A significant difference was found between the voiding and nonvoiding groups, with 38.9% (14/36) versus 17.1% (21/123) of patients, respectively, having moderate bladder activity and 22.2% (8/36) versus 4.9% (6/123) of patients, respectively, having intense bladder activity. Conclusion: Refraining from voiding before 18F-fluciclovine injection results in significantly lower urinary bladder radioactivity than does purposeful voiding before injection. We have modified our practice accordingly, particularly as moderate and intense bladder activity may mask or mimic local prostate cancer recurrence. Mechanisms underlying this phenomenon should be further investigated.
Prostate cancer imaging using the synthetic amino acid analog 18F-fluciclovine (Axumin; Blue Earth Diagnostics Ltd.) was recently approved by the Food and Drug Administration. The synthetic amino acid 18F-fluciclovine enters cells via amino acid transporters and is not metabolized by the cells or incorporated into protein synthesis (1). Normal biodistribution of 18F-fluciclovine includes the liver, bone marrow, pancreas, and skeletal muscles (2–5). The amino acid transporters also mediate 18F-fluciclovine reabsorption by the kidneys at the proximal tubules, which results in slow urinary excretion over time (1). Slow 18F-fluciclovine urinary excretion makes it a favorable radiotracer for pelvic tumor imaging because of reduced potential for interference from intense bladder activity, especially in the evaluation of locally recurrent prostate cancer (4,6–10). High bladder 18F-fluciclovine activity may interfere with the evaluation of local prostate cancer recurrence, as it may mimic or mask areas of local prostate cancer recurrence. 18F-fluciclovine prescribing information states that only 3% of the administered radioactivity is excreted in the urine in the first 4 h after injection (11). Schuster et al. reported intense 18F-fluciclovine bladder activity (≥liver) in 15.2% of the delayed images (approximately 30 min after radiotracer injection) obtained from 128 patients who underwent 18F-fluciclovine PET/CT, yet no intense uptake was reported in early images (∼5 min after radiotracer injection) (5).
In our clinical practice, however, we have noticed a higher than expected degree of 18F-fluciclovine urinary excretion using the standard PET/CT protocol, which includes instructing the patient to void before radiotracer injection and commencing PET acquisition at approximately 4 min after radiotracer injection. As part of our quality control process, we decided to examine a new protocol in which the patients are not asked to purposefully empty their bladder before the start of the study, in the expectation that a distended urinary bladder may mitigate the quantity and intensity of early 18F-fluciclovine excretion.
In this analysis, we retrospectively evaluated and quantified early 18F-fluciclovine bladder excretion in our clinical practice. We also examined whether the nonvoiding protocol affects bladder activity and compared these results with a subset of patients studied before we changed the protocol.
MATERIALS AND METHODS
Patient Population
We retrospectively assessed scans of 159 patients who underwent 18F-fluciclovine PET/CT imaging at our institution as part of their clinical evaluation from August 2016 to November 2017. This retrospective cohort analysis was approved by the Institutional Review Board and was in compliance with the Health Insurance Portability and Accountability Act. The requirement to obtain documentation of informed consent was waived.
Imaging Protocol
PET/CT images were acquired on an Ingenuity time-of-flight PET/CT scanner (Philips). All patients were instructed to fast for 4–6 h before the injection of 18F-fluciclovine. Patients were allowed to have water with medications. 18F-fluciclovine (PETNET Solutions) was injected as an intravenous bolus while patients were in the PET/CT scanner with arms down, followed by a flush injection of sterile 0.9% sodium chloride. The mean dose ± SD was 370 ± 44.4 MBq (range, 173.9–425.5 MBq). The patients subsequently underwent a CT scan from the mid thigh to the skull base while supine with arms up, without oral or intravenous contrast medium. PET image acquisition began at exactly 4 min after injection (the technologist used a stopwatch), from the mid thigh to the skull base, while the patients were supine with arms up. The first 36 patients were instructed to empty their bladder before the injection of 18F-fluciclovine as part of the standard protocol. Because we noticed that many patients had unexpectedly high urinary 18F-fluciclovine excretion, we changed the protocol prospectively to eliminate purposeful voiding before the scan, as part of our clinical quality control process. Thus, the subsequent 123 patients were no longer asked to void immediately before the scanning.
Image Analysis
Images were reviewed on Hermes Gold workstations (Hermes Medical Solutions). On the basis of visualization, bladder radioactivity was defined as positive if the bladder could be visualized on the maximum-intensity-projection images. Subsequently, quantitative data were collected: the SUVmax and SUVmean of the bladder cavity, aorta, marrow (at the level of L3), and liver were recorded. Bladder cavity SUVmean was compared with the SUVmean of the aorta, marrow, and liver. Bladder excretion activity was characterized as insignificant (bladder < aorta), mild (bladder ≥ aorta < marrow), moderate (bladder ≥ marrow < liver), or intense (bladder ≥ liver) (Fig. 1). Subsequently, the patients were divided into 2 groups according to the different imaging protocols: voiding (patients voided just before 18F-fluciclovine injection) or nonvoiding (patients were not asked to void before 18F-fluciclovine injection). The bladder activities were calculated for all patients. Bladder 3-dimensional volumes were measured using the volume-of-interest interpolation tool of Hermes 3-dimensional software.
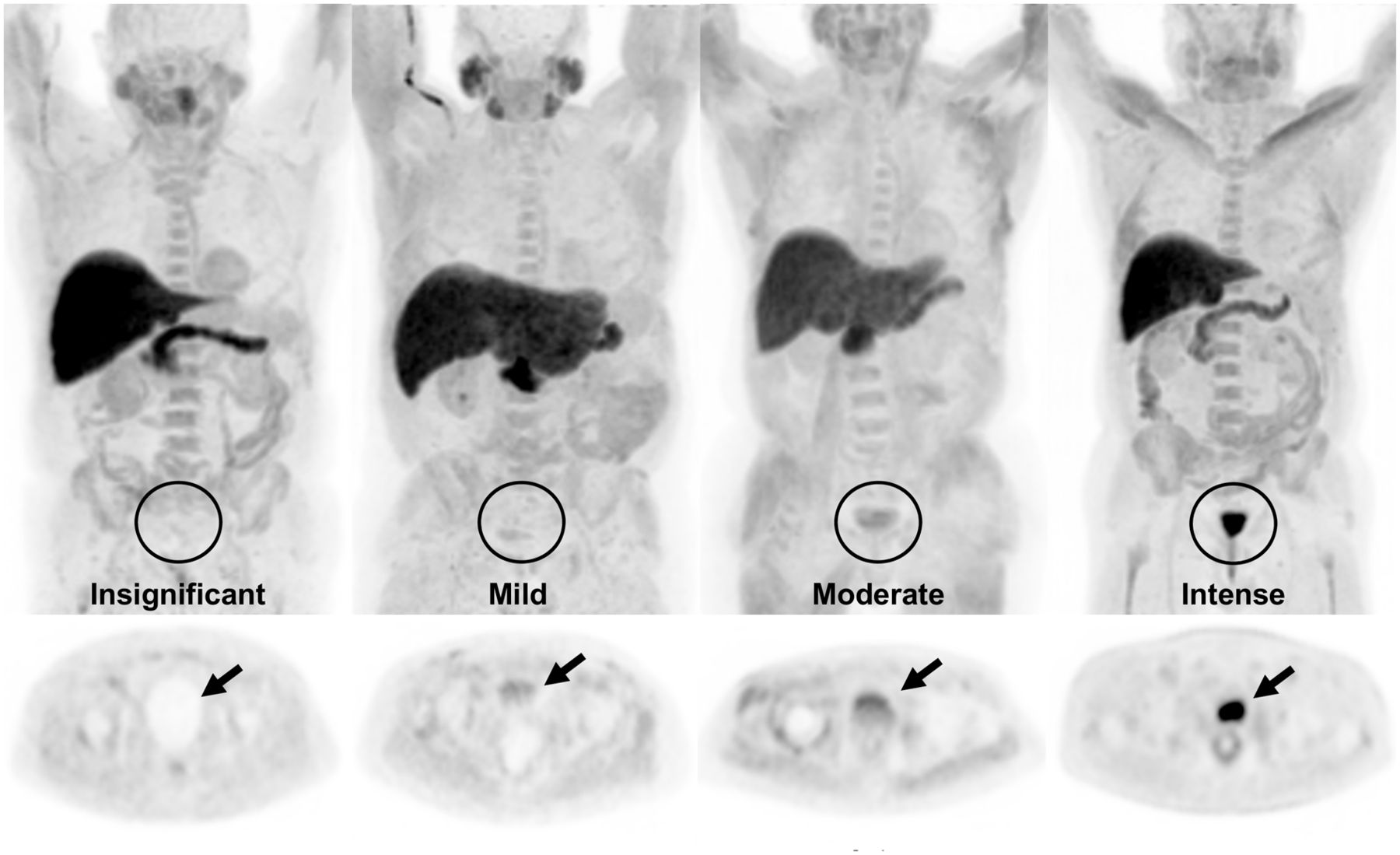
Groups of bladder activity (encircles or arrowed). SUVmax threshold in all images is 7.0.
Statistics
Data analysis was conducted on STATA 15 (StataCorp LLP) statistics software. All continuous variables were expressed as median, with related interquartile range (IQR; 25th–75th percentiles). A Wilcoxon rank-sum test was used to compare differences in the demographic characteristics of the patients between the 2 protocol groups, including age, 18F-fluciclovine dose, and the medians of bladder activity, bladder volume, and background SUVmax and SUVmean. The Pearson χ2 test was used to compare the statistical significance of differences in bladder activity between the 2 protocol groups. The Spearman correlation between bladder volume and bladder SUVmean was determined. A P value of less than 0.05 was considered to be statistically significant.
RESULTS
Demographics
The median patient age was 69 y (IQR, 64–73 y). The median SUVmean of the bladder was 1.6 (IQR, 1.6–3.6). The median ratios of bladder to aorta, marrow, and liver were 1.1 (IQR, 0.4–2.3), 0.52 (IQR, 0.2–1.1), and 0.5 IQR, (0.2–1.1), respectively. All demographic characteristics and measured activities are summarized in Table 1.
Demographics and Overall Bladder Activity and Volume
Overall Bladder Activity
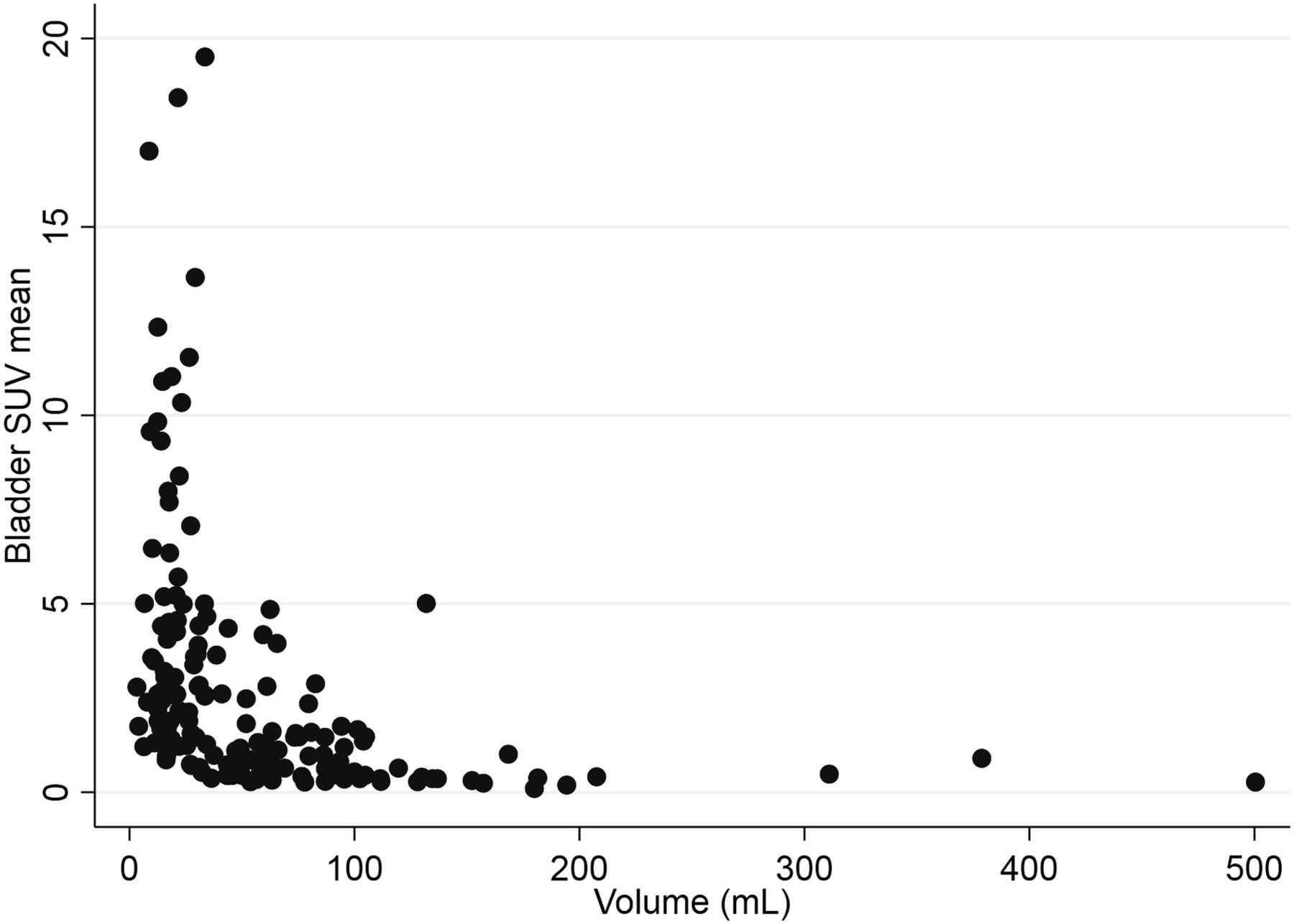
On subjective visualization, bladder radioactivity was noticed on the maximum-intensity-projection images of 53.5% (85/159) of patients. On quantitation, insignificant bladder activity was found in 48.4% (77/159) of patients, mild activity in 20.8% (33/159), moderate activity in 22.0% (35/159), and intense activity in 8.8% (14/159) (Table 1). A significant negative association was found between bladder volume and bladder SUVmean (ρ = −0.64, P < 0.001) (Fig. 2). Significantly larger volumes were noted in the group with insignificant bladder activity, and smaller volumes were found in the group with intense bladder activity (P < 0.001).
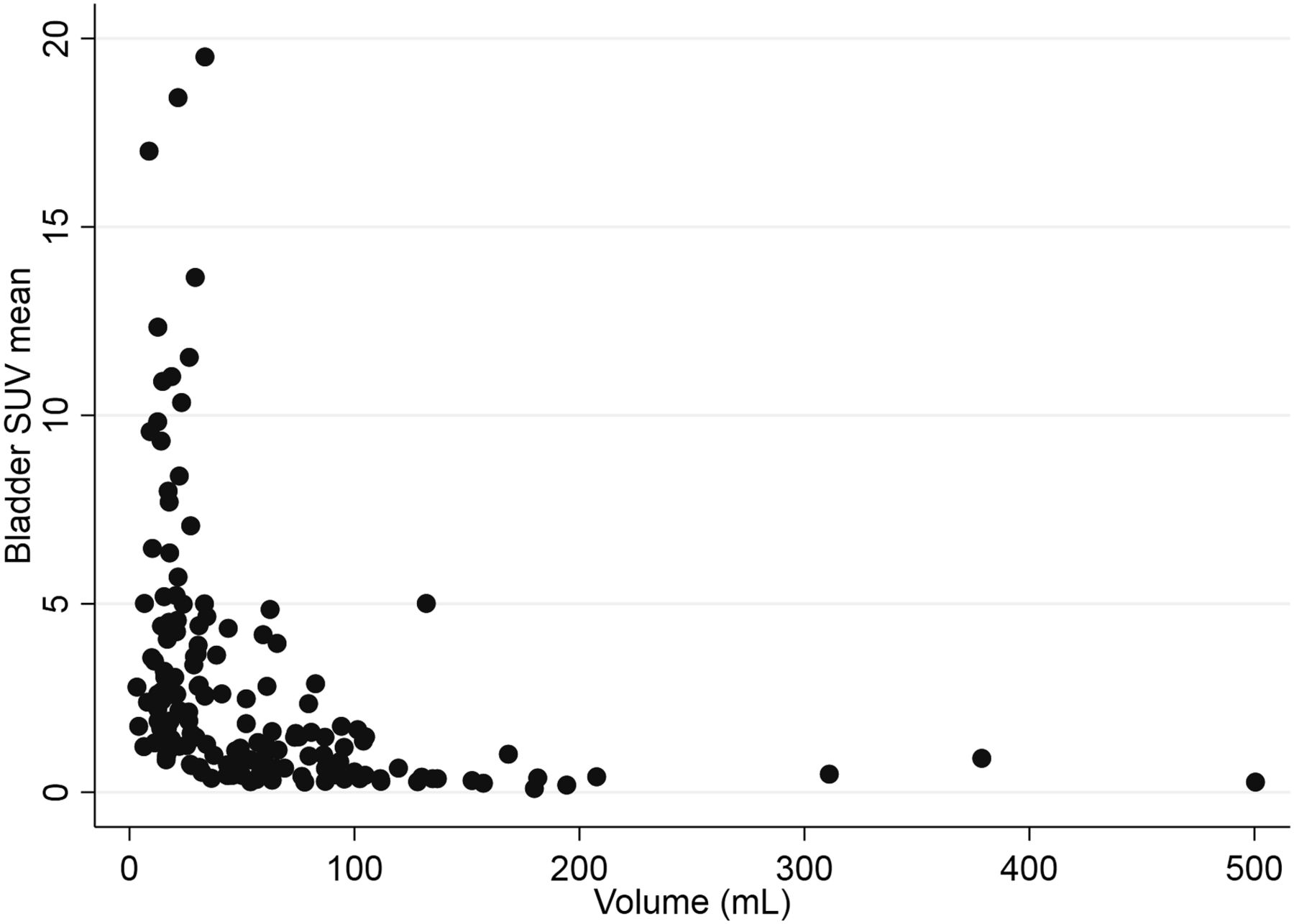
Bladder radioactivity and volume scatterplot. Spearman ρ = −0.64 (P < 0.001).
Effect of Voiding Protocol on Bladder Activity
Among the 159 patients, 36 were imaged with the voiding protocol and 123 with the nonvoiding protocol. Bladder SUVmax, bladder SUVmean, and bladder-to-background ratio were significantly higher for the voiding protocol than for the nonvoiding protocol (Table 2). The median SUVmax and SUVmean of the bladder were 4.9 (IQR, 3.4–8.1) and 2.8 (IQR, 2.1–6.0), respectively, for the voiding protocol versus 2.1 (IQR, 1.1–5.6) and 1.3 (IQR, 0.5–2.8), respectively, for the nonvoiding protocol (P ≤ 0.001) (Fig. 3A). The median bladder-to-aorta, bladder-to-marrow, and bladder-to-liver ratios were 2.2 (IQR, 1.5–4.49) versus 0.8 (IQR, 0.4–1.8), 1.1 (IQR, 0.6–2.2) versus 0.4 (IQR, 0.2–0.9), and 0.4 (IQR, 0.2–0.7) versus 0.2 (IQR, 0.1–0.3), for the voiding and nonvoiding protocols, respectively (P < 0.001).
Quantification Differences and 18F-Fluciclovine Bladder Activity Comparison Between 2 Different Protocol Groups

(Top) Bladder SUVmax and SUVmean difference between protocols. (Bottom) Distribution of different bladder activity groups between protocols. *Statistically significant difference (P < 0.05). Mdn = median.
Among the patients in the voiding protocol, the bladder was visualized on the maximum-intensity-projection images in a significantly higher number of scans: 77.8% (28/36) of scans in the voiding protocol and only 46.3% (57/123) in the nonvoiding protocol (P < 0.001).
A significantly higher number of patients with intense bladder activity and a significantly lower number of patients with insignificant bladder activity were found among patients in the voiding protocol, and the reverse was found among patients in the nonvoiding protocol (Fig. 3B). For patients in the voiding protocol, insignificant bladder activity was found in only 19.4% (7/36) of patients, and 22.2% (8/36) of patients had intense bladder activity. For patients in the nonvoiding protocol, insignificant bladder activity was found in 56.9% (70/123) of patients, and only 4.6% (6/123) of patients had intense bladder activity (P < 0.001). No significant differences in the frequency of mild bladder activity were found between the 2 protocols (Table 2).
Overall, lower bladder volumes were associated with the voiding protocol than with the nonvoiding protocol, with a median volume of 18.0 mL (IQR, 12.6–30.6 mL) versus 51.9 mL (IQR, 25.4–87.1 mL), respectively (P < 0.001). For insignificant and mild bladder activity, the volumes were also significantly lower with the voiding protocol (P < 0.05). However, for moderate and intense bladder activity, no significant differences in volume were observed between the voiding and nonvoiding protocols (P > 0.05).
DISCUSSION
This retrospective comparative study was prompted by our observation that in our clinical practice, 18F-fluciclovine urinary excretion into the bladder was relatively higher than expected from what has been reported in the published literature. Moreover, we observed that this effect seemed to be minimized by a simple change in protocol in which patients were not instructed to void before 18F-fluciclovine injection and imaging. In this analysis, we sought to quantify the incidence and degree of early 18F-fluciclovine urinary excretion into the bladder and to determine whether the changes we applied to our patient preparation protocol (as part of our quality control effort) mitigated bladder activity. Our analysis confirmed that when we stopped asking the patients to void before the injection of 18F-fluciclovine, we observed a significantly lower number of patients with increased bladder activity (P < 0.05).
Our findings are important because intense 18F-fluciclovine activity in the bladder—though usually visually less bothersome than that seen with 18F-FDG, for example—may still interfere with the evaluation of local prostate cancer recurrence. For example, 18F-fluciclovine activity in the bladder or urethra may mimic or obscure suggestive activity in the prostate or prostate bed. Our findings on the degree and extent of early 18F-fluciclovine urinary bladder activity differ from those in the available literature (2,4). Schuster et al. investigated bladder activity among 128 patients who underwent 18F-fluciclovine PET/CT and reported moderate 18F-fluciclovine bladder activity (≥marrow) in only 3.1% of the scans at 5 min after injection and no intense activity (≥liver). Schuster also reported moderate and intense bladder activity in 59.1% and 14.2% of patients, respectively, but only at a delayed time point of 17 min after injection (5). We documented moderate and intense bladder activity in 38.9% and 22.2% of patients, respectively, in a clinical protocol that commences scanning at 4 min after radiotracer injection and has patients void before injection, as they had been instructed in the referenced research studies. Yet, when patients were not instructed to void before radiotracer injection, moderate and intense bladder activity was present in only 17.1% and 4.9% of patients, respectively.
18F-fluciclovine is advantageous for imaging prostate cancer recurrence, particularly because of its low urinary excretion compared with other radiotracers (1,4,12). 18F-fluciclovine biodistribution in clinical studies demonstrated only minimal and slow urine exertion (2). This phenomenon of sporadically increased early bladder excretion of 18F-fluciclovine in research patients, though not to the degree we have seen clinically, had been investigated by Amzat et al., including its correlation with radiotracer dose, body mass index, body weight, blood urea nitrogen, creatinine, glucose, and routine urinalysis, as well as radiotracer activity in liver, marrow, muscle, and blood pool (13). A subset of patients underwent thin-layer chromatography of their urine. The investigators concluded that the bladder activity reflected a lack of reabsorption of the parent compound in the kidney. Of the investigated parameters, only proteinuria was associated with higher bladder activity in the entire cohort, yet it was not present in most patients with abnormal bladder activity (defined, for this analysis, as activity greater than marrow activity). Work by Ono et al. investigated the mechanism of 18F-fluciclovine reabsorption by the kidneys and found that its slow urinary excretion is mediated in part by reuptake via amino acid transporters but not by drug transporters such as P-glycoprotein. The group reported that alanine-serine-cysteine amino acid transporters, including alanine-serine-cysteine transporter type 2, are likely the primary transporters responsible for 18F-fluciclovine reuptake by renal proximal tubules (1).
On the basis of earlier work and our current analysis, as best as we can determine, the observation of increased bladder activity likely represents relatively earlier urinary excretion of the parent radioligand, similar to what has been reported at delayed imaging in research patients (5,13). This phenomenon is likely secondary to differences in renal reuptake kinetics mediated by amino acid transporters, yet the exact reason for these differences is not fully understood. Validation studies demonstrated that the 18F-fluciclovine molecular structure of the commercial and research preparation, as well as radiochemical purity and identity, is the same, and the complex demonstrated excellent stability over a wide range of radioactivity concentrations (oral communication, Blue Earth Diagnostics Ltd.). As demonstrated in the bladder uptake and volume scatterplot graph (Fig. 2), there is a negative association between bladder volume and bladder SUVmean. Thus, the high bladder excretion seen in the manufactured radiotracer may be mitigated by a distended bladder. It may be that under less carefully controlled conditions and patient populations than were present in the research studies, this phenomenon is now seen to a greater degree in clinical patients, but this would require further study.
Though the mechanism of early 18F-fluciclovine bladder activity is not fully understood, there is a need to investigate different methods to minimize bladder visualization, since higher bladder activity may interfere with interpretation in some instances. Therefore, we examined a tailored protocol to address these findings. Our proposed protocol of not asking patients to void before 18F-fluciclovine injection significantly decreased bladder activity and helped to maintain an acceptable target-to-background ratio within the pelvis, allowing better evaluation of local prostate cancer recurrence. Scans obtained with the nonvoiding protocol demonstrated lower bladder activity and a negative correlation with bladder volume. As a result, we have adopted the new protocol in our routine clinical practice (14,15). Although we do not suggest that refraining from voiding changes the mechanism of 18F-fluciclovine urinary excretion, we hypothesize that bladder distension might mitigate the effect of urinary radiotracer excretion into the bladder by a combination of 2 hypothesized mechanisms. The first hypothesis is that in men who do not void before 18F-fluciclovine administration, the resultant higher volume of urine in the bladder results in a lower concentration of radioactivity in the bladder. This possibility is consistent with a reported lower concentration of 18F-FDG in the urine of rats and humans when the bladder was distended by the use of hydrochlorothiazide and furosemide diuretics, retrospectively (16,17). The second hypothesis is that elevated pressure in the urinary collecting system secondary to a full bladder may result in slower 18F-fluciclovine urinary excretion. This theory derives from the known effects of mechanical obstruction on renal function, such as reduced glomerular filtration rate, decreased renal plasma flow, and profound changes in renal tubular cell function (18).
Two major limitations of this study are the lack of prospective controls randomized to voiding or not voiding and the lack of urinalysis data. This protocol was devised not as a prospective study but as part of our clinical practice quality control efforts to limit the visualized bladder activity. Therefore, we did not collect urine from each patient to evaluate the percentage of urinary excreted 18F-fluciclovine or its urine concentration. The use of diuretics in each patient was also not known. Unlike the research studies, we do not obtain dual- or triple-time-point imaging, which would help in analysis of bladder activity over time. Also, in our department, a restroom is available in the patient waiting area; we therefore cannot be certain that patients on the nonvoiding protocol did not void just before the scan. For the group with intense bladder activity, we found statistically lower bladder volumes, overall, than in the groups with other levels of bladder activity. However, no significant volume differences in the intense-activity classification were found between the voiding and nonvoiding groups. In fact, all 6 patients with intense bladder activity in the nonvoiding group had a contracted bladder, with only minimal urine volume (measured volume ± SD averaged 23 mL ± 7.6, with a median of 24.4 mL [IQR, 17.7–27.2 mL]). This finding suggests these patients may have voided before the scan without our knowledge, thus affecting our final analysis.
CONCLUSION
In our clinical practice, 18F-fluciclovine urinary excretion was higher than what was expected from the reported research studies. Voiding just before the injection of 18F-fluciclovine may increase the potential for visualized bladder activity. Refraining from voiding before the 18F-fluciclovine injection and scan may result in a significant decrease in bladder activity. The resulting decrease in the number of scans with intense bladder activity makes image interpretation more convenient and improves evaluation of the prostate and prostate bed. Hence, we have adopted the new nonvoiding protocol in our routine clinical practice. Mechanisms underlying this phenomenon should be further investigated.
DISCLOSURE
David Schuster is a consultant for Syncona and for AIM Specialty Health and participates through the Emory Office of Sponsored Projects in sponsored grants, including those funded or partially funded by Blue Earth Diagnostics, Ltd., Nihon MediPhysics Co, Ltd., Telix Pharmaceuticals (U.S.) Inc., and Advanced Accelerator Applications. Bital Savir-Baruch has received a grant sponsored by Blue Earth Diagnostics and is lecturer for Philips. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 11, 2019.
REFERENCES
- Received for publication May 2, 2019.
- Accepted for publication August 8, 2019.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.