


Abstract
A modular radiation detector device that was developed by Lucerno Dynamics, LLC, collects data during the entire uptake period of a molecular imaging study and then retrospectively assesses these data for signs of dose infiltration. The objective of this study was to test the feasibility of using this device for real-time, rather than retrospective, assessment of the injected dose. Methods: For 20 patients undergoing a clinical PET scan, we manually collected real-time counts from the device for 60 s and then compared the resultant time–activity curves with those generated from automated 60-min counts collected by the device. Results: The R2 value calculated for the averages across the 2 curves was 0.93 (93%), meaning the 2 curves matched statistically. Conclusion: The external detector device may be used to ascertain, within only 60 s, whether an injection is sufficient.
The Lara detector (Lucerno Dynamics, LLC) is a class 1 exempt medical device listed with the Food and Drug Administration. It was originally intended to dynamically measure the presence of a radiopharmaceutical in an organ or body region during uptake as part of a nuclear medicine procedure. It is now indicated for use as a tool to help assess whether a radiopharmaceutical remains near the injection site rather than circulating in the vascular system.
Since the beginning of molecular imaging, infiltration of the radiotracer has been known to cause false-positive lymph node uptake (1). The Lara detector can play a role in observing infiltration. The current version of this device offers 4 detectors and a digital screen to display step-by-step instructions for setup and collection of data (Fig. 1). During the injection and uptake time, data are collected and then uploaded to a server, where they can be visualized and assessed for signs of infiltration. Once the data are uploaded, the device gives the injection a score and displays time–activity curves that have been corrected for radioactive decay, temperature, and other specific detector effects. A score less than 200 suggests a negligible presence or no presence of radiotracer was left near the injection site. Scores over 200 indicate the possibility that radiotracer remained near the injection site, allowing clinicians to decide if the patient should be rescheduled. If a significant infiltration were indicated, the patient could be rescheduled prior to undergoing imaging. The objective of this study was to test the feasibility of using this device for real-time assessment of the injected dose, as opposed to the current mechanism, which allows only retrospective analysis of the acquired data.

Modular detector device. Digital screen and 2 of 4 detectors are shown.
MATERIALS AND METHODS
Our institutional review board determined that this research activity did not meet the definition of human research found in title 45 of the Code of Federal Regulations, part 46, and the need for informed consent was therefore waived.
Twenty PET/CT patients were connected to the detector device before their 18F-FDG injection. Two small detectors were placed on each patient: one detector on the injection arm proximal to the injection site and the other in the same area on the opposite arm to serve as a control (Fig. 2). Standard automated data collection using the device was performed from the time of injection until the end of the uptake time (∼60 min). Manual real-time data collection from the device was performed at 7 time points during tracer injection: 5, 10, 20, 30, 40, 50, and 60 s. The data were then uploaded to the device server to obtain the complete time–activity curve and associated score. These data allowed for prediction of whether activity would remain at the injection site and of how rapidly the counts would decrease to the typical baseline value that was given by the control arm sensor.

Modular detector device in use on patient.
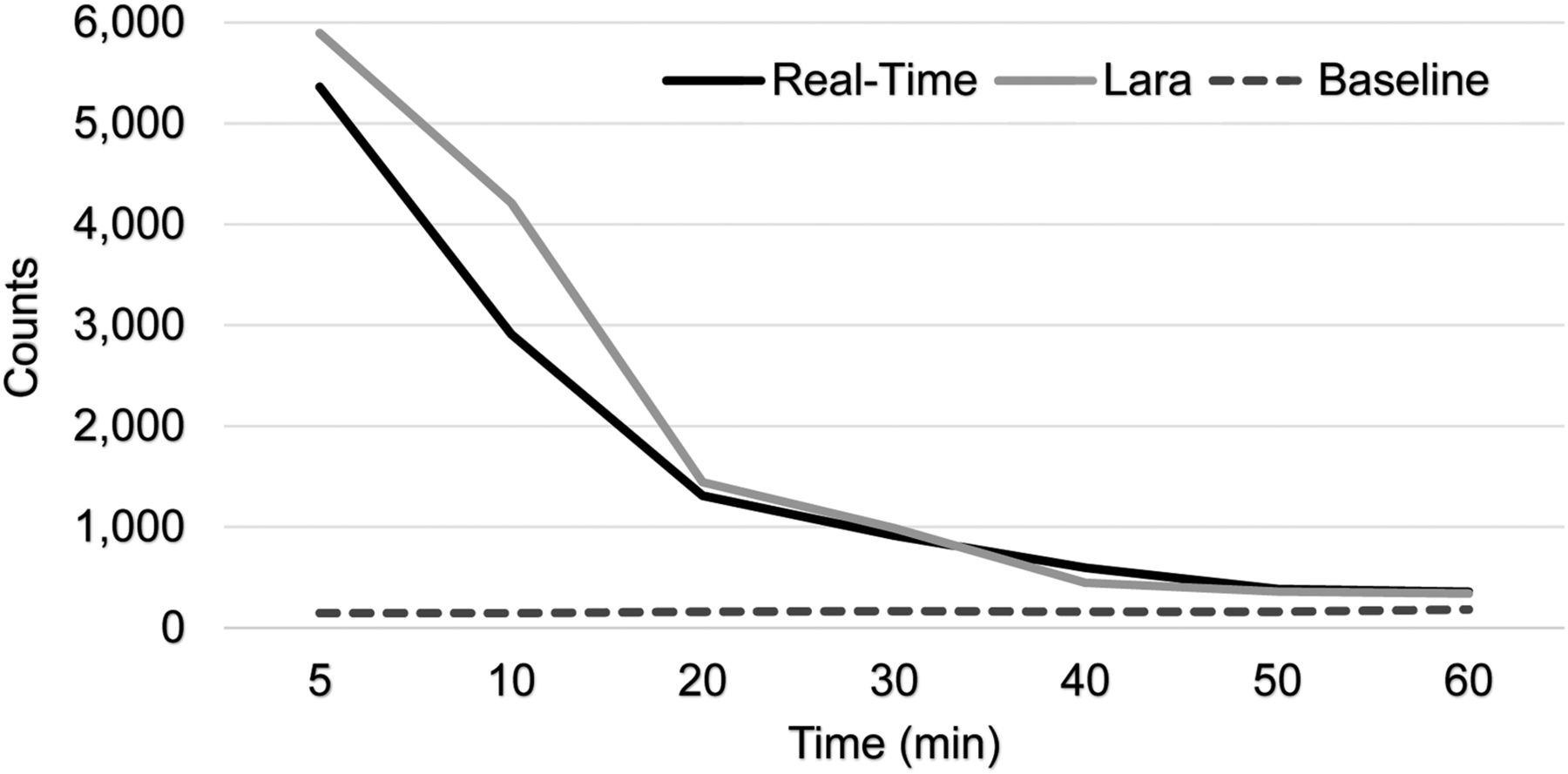
The manually real-time collected curves were compared with the device-collected curves to assess whether the data converged, and if so, how rapidly (Fig. 3). Convergence rates were compared between standard system time–activity curves and real-time data collection to determine if infiltration predictions matched between methods. The data points for the automated and manual assessments were averaged across all 20 patients, and R2 values were calculated for the comparison of the automated and manual data collection methods to see whether the time–activity curves for the two techniques matched.
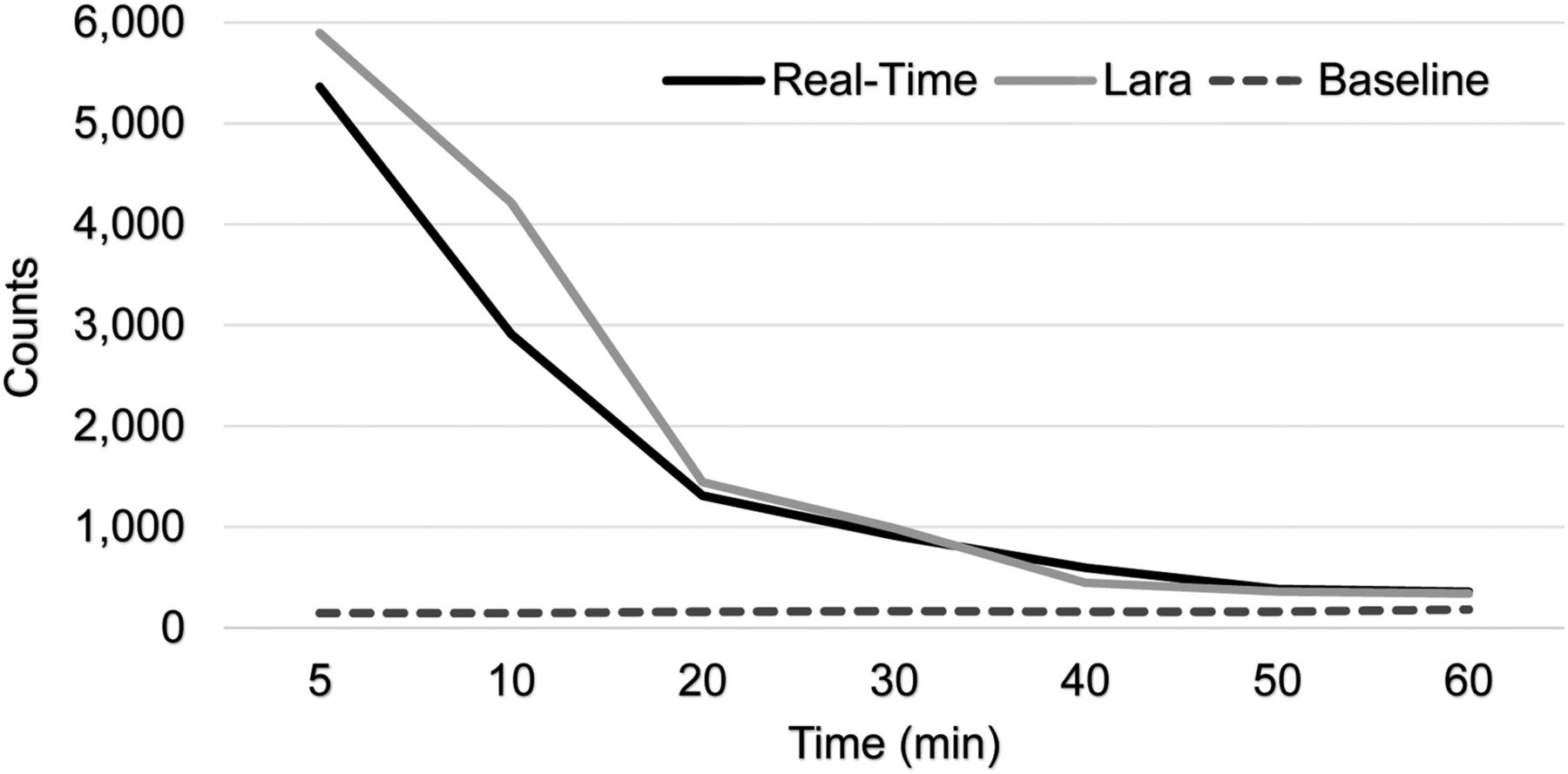
Manually collected (real-time) curve compared with device-collected curve and baseline curve to assess whether data converged.
RESULTS
In all 20 patients, the Lara device scored the injection at less than 200, indicating little to no radiotracer left near the injection site. After each scan, the images were visually reviewed, and none showed evidence of activity at the injection site or infiltration. Based on manual, real-time data collection, baseline threshold values were reached within approximately 60 s for each patient. Within this time frame, it was possible to observe the peak in counts detected from the bolus injection passing over the sensor and watch this drop back to the typical baseline value—200–400 counts—that was given by the control arm sensor (Table 1; the table also shows data for a low-quality injection, for comparison.) An R2 value of 0.93 (93%) was calculated between the real-time data time–activity curve and the automated data time–activity curve, meaning the 2 curves matched statistically.
Real-Time Counts from High-Quality Injection (Score of −223) and Low-Quality Injection (Score of +3,795)
DISCUSSION
Current methods for monitoring injections and potential infiltration require injecting the entire patient dose and then assessing the injection site after the 60-min uptake time using either the PET/CT system or the external detector device. The problem with these methods is that the patient has already been present for the entire uptake period and, if the injection quality is poor, will have to return on another day to repeat the imaging study. If the injection site activity were monitored in real-time and the presence of lingering activity detected within the first 60 s, the patient could be rescheduled immediately, without having to wait until the end of the entire uptake period. No infiltrations were suspected based on real-time or standard assessment of data from the sensors.
CONCLUSION
An external detector device may be used to ascertain, within only 60 s, whether an injection is sufficient. Although this method is less accurate than analysis of a longer and more complete set of time–activity curves, a significant infiltration would take much longer to reach baseline than would a noninfiltrated injection. The standard method for using an external detector device is to inject the entire patient dose and then assess the injection quality after the full uptake time of 60 min. With real-time monitoring, injections with activity remaining at the injection site would be captured within the first 60 s, and the procedure could be rescheduled at that time. This advantage would result in time savings for the patient and imaging center.
DISCLOSURE
The University of Tennessee was engaged with Lucerno in a quality improvement study during the time this research was performed. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Chris Carr CNMT, RT(R), and Erica Carrol, CNMT, for their assistance with this project.
Footnotes
Published online Apr. 24, 2019.
REFERENCE
- 1.↵
- Received for publication December 11, 2018.
- Accepted for publication March 4, 2019.





{kind=link}
{kind=link}
{kind=link}