


Article Figures & Data
Figures
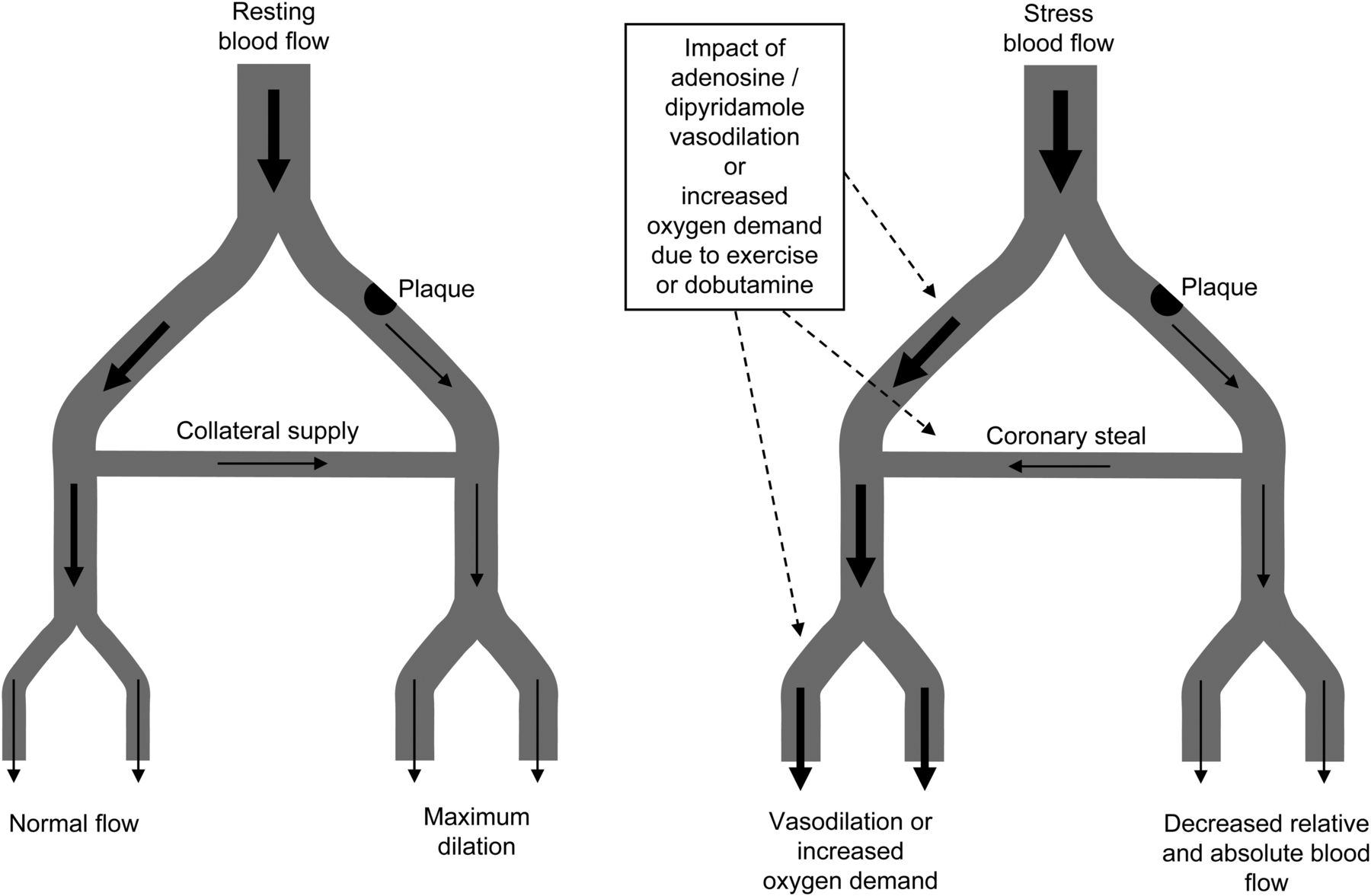
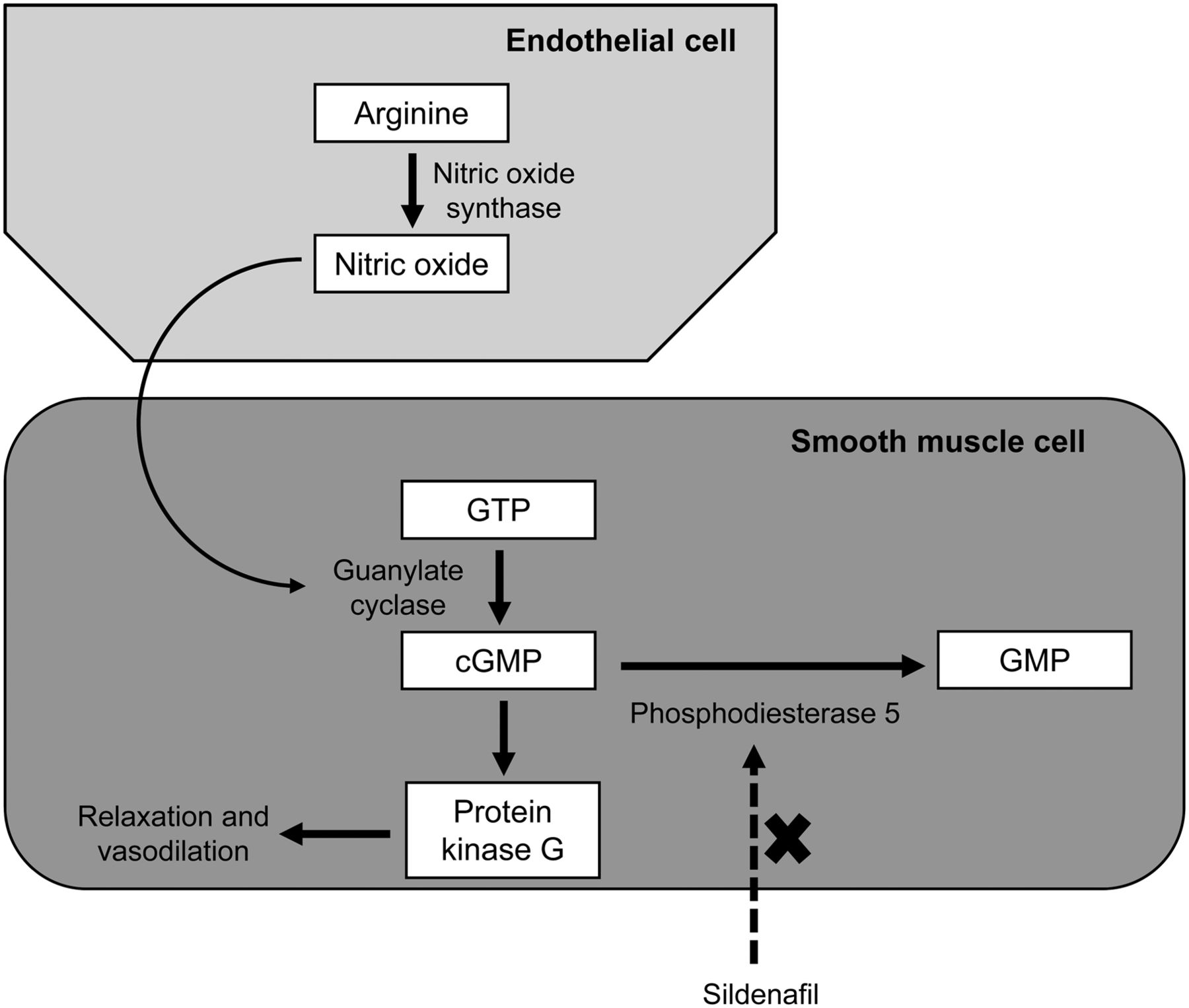
- FIGURE 1.
Schematic representation of general principle of pharmacologic stress in myocardial perfusion imaging. Ischemic myocardium may maintain resting blood supply with collateral vessels and resting vasodilation. Under pharmacologic vasodilation or increased oxygen demand (exercise or inotropic), blood flow difference between normal and stenosed vessels will exaggerate blood flow difference and expose coronary flow reserve (difference between maximum and resting flow rates). This may be further influenced by coronary steal.
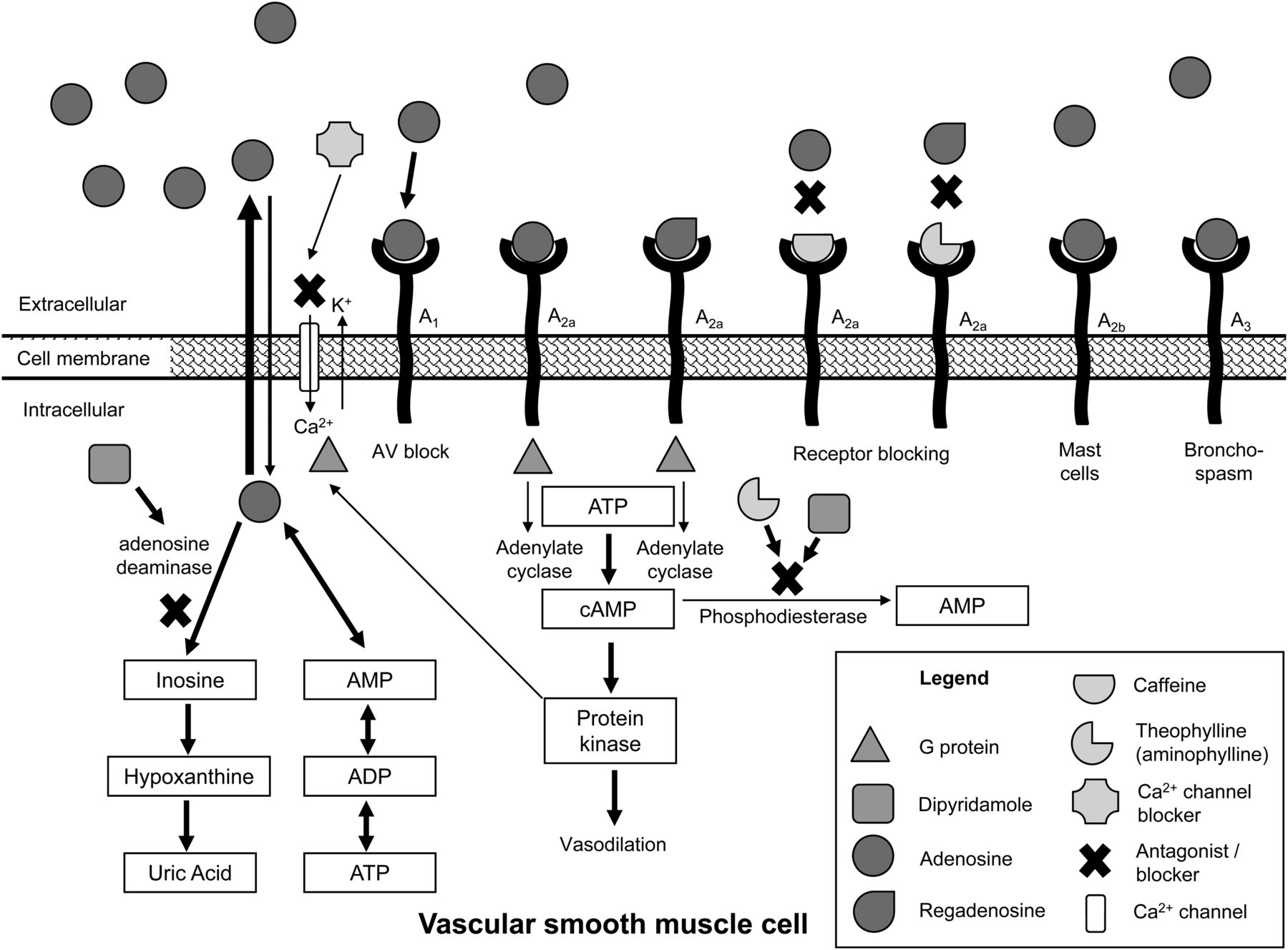
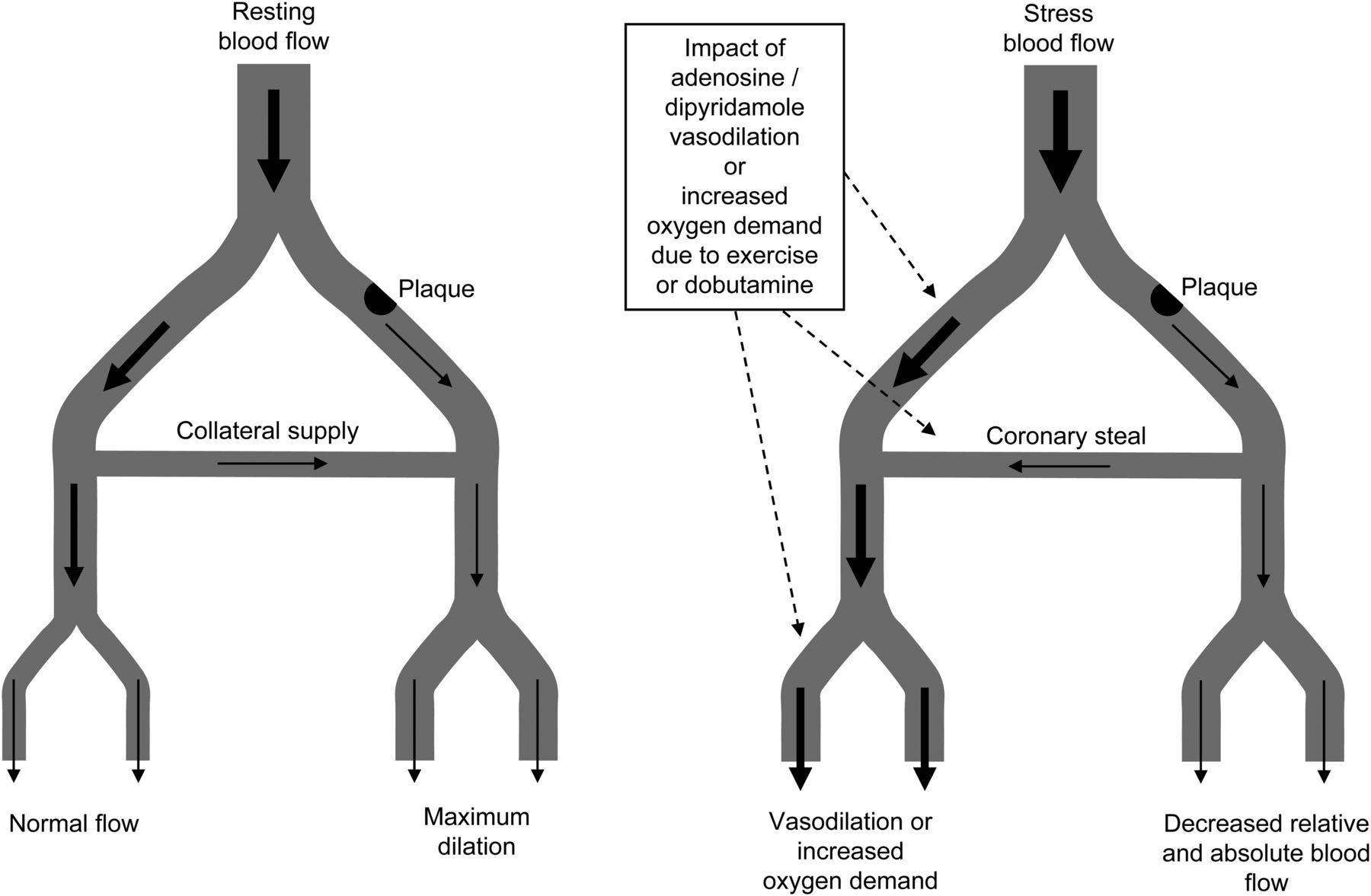
- FIGURE 2.
Schematic representation of action of vasodilating agents in vascular smooth muscle cell. Endogenous adenosine is produced in vascular smooth muscle cells and leaves cell. In extracellular space, endogenous and exogenous adenosine can couple with 4 types of adenosine receptors. Receptor A1 couples with adenylate cyclase inhibitory G protein to produce atrioventricular (AV) block and some bronchoconstriction. Receptor A3 couples with adenylate cyclase inhibitory G protein to produce bronchoconstriction. Receptor A2b couples with adenylate cyclase, stimulating G protein to produce mast cell degranulation, peripheral vasodilation, and antiplatelet activity. Receptor A2a couples with adenylate cyclase, stimulating G protein to convert adenosine triphosphate (ATP) to cyclic adenosine monophosphate (cAMP) and produce coronary and peripheral vasodilation. Regadenoson is selective for receptor A2a to produce vasodilation. Caffeine has greater selectivity for receptors A1 and A2a to antagonize those actions. Theophylline (aminophylline and tea) has 3–5 times higher potency than caffeine in antagonizing receptors A1 and A2a, whereas theobromine (typical of chocolate) has lower potency than caffeine. Dipyridamole antagonizes adenosine deaminase, which reduces adenosine metabolism and thus increases availability of adenosine in extracellular space. Dipyridamole is also phosphodiesterase inhibitor so blocks conversion of cyclic adenosine monophosphate to adenosine monophosphate, further increasing vasodilation. Calcium channel blockers act to antagonize voltage-dependent calcium channel to block vasodilation. ADP = adenosine diphosphate.
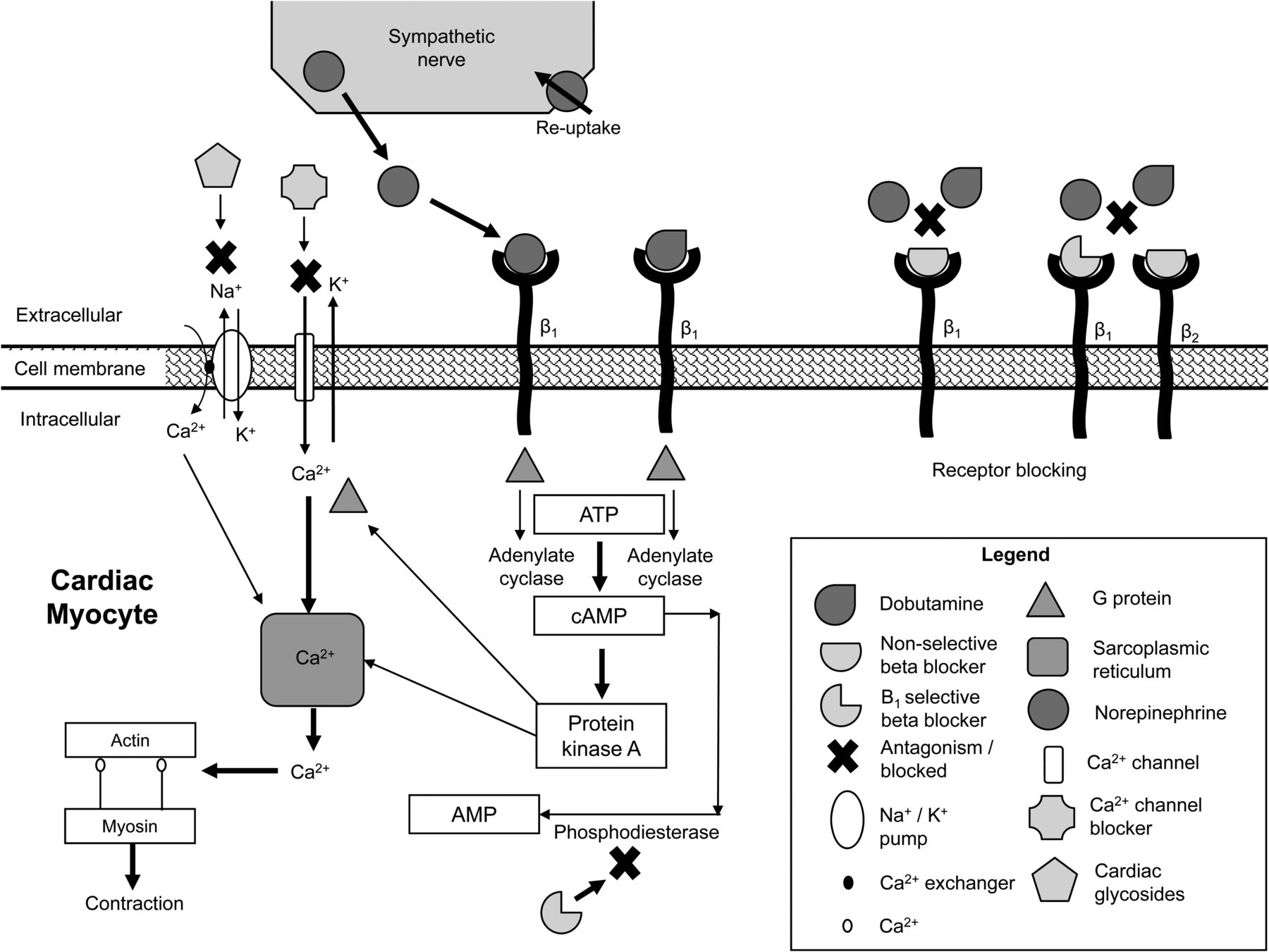
- FIGURE 3.
Schematic representation of action of inotropic/chronotropic agents in cardiac myocyte. Endogenous norepinephrine is released from sympathetic nerve. In reuptake mechanism failure (e.g., heart failure), excess norepinephrine is available for β1 activation. In extracellular space, endogenous norepinephrine and exogenous dobutamine can couple with β1-receptors. Receptor β1 couples with adenylate cyclase, stimulating G protein to drive increased intracellular calcium, which facilitates formation of actin–myosin cross bridges and produces increased force and rate of contraction. This response can be antagonized by β-blocker either nonselective (e.g., propranolol) or selective (e.g., atenolol) for β1. Calcium channel blockers act to antagonize voltage-dependent calcium channel to block inotropic and chronotropic contraction response. Likewise, cardiac glycosides such as digoxin antagonize sodium/potassium pump to increase intracellular calcium via calcium exchanger, increasing force of contraction. cAMP = cyclic adenosine monophosphate; ATP = adenosine triphosphate.
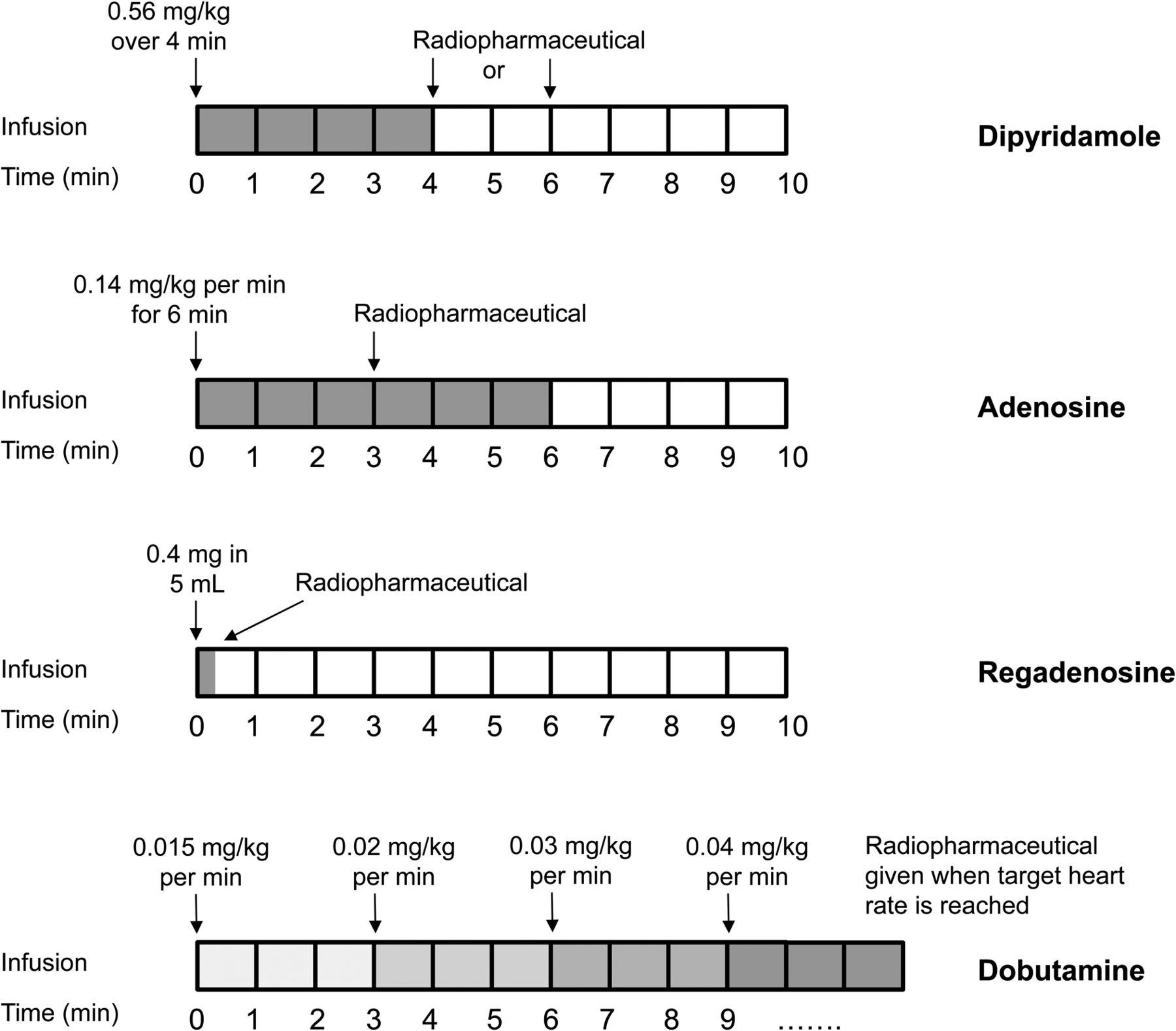
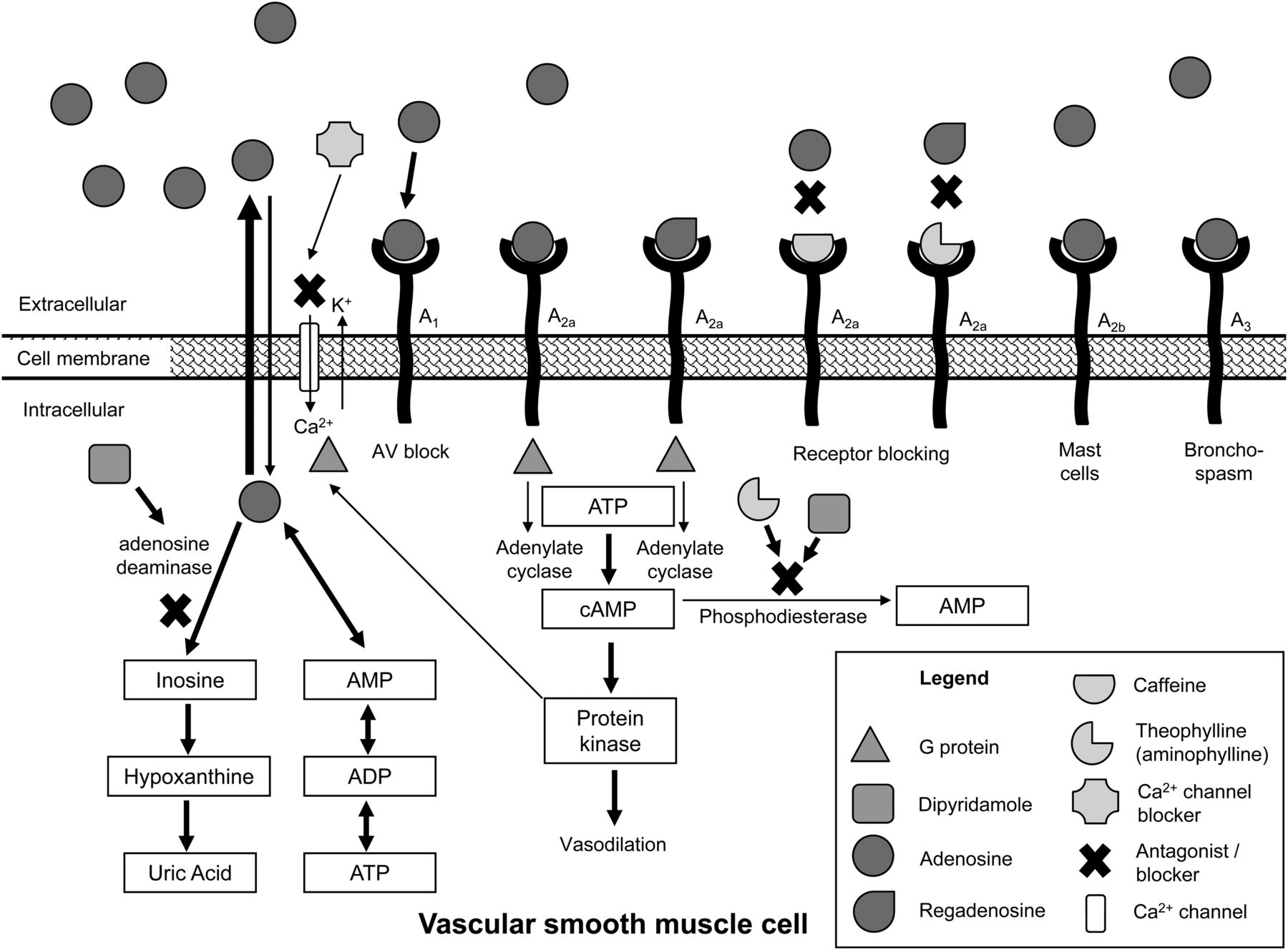
- FIGURE 4.
Comparison of infusion techniques for main pharmacologic stress agents.
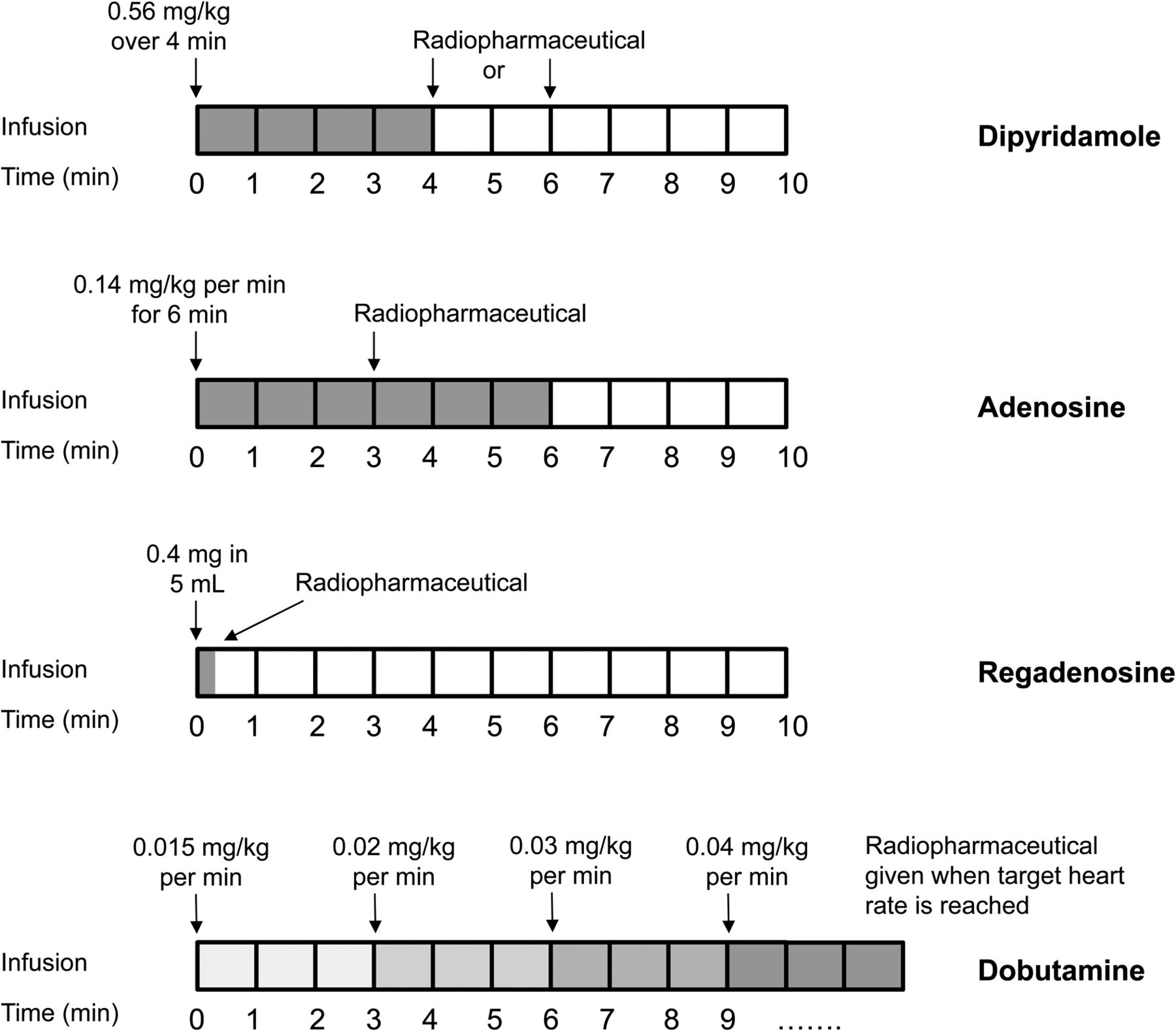
- FIGURE 5.
Schematic representation of production of nitric oxide in endothelial cells with subsequent activation of guanylate cyclase in smooth muscle cells. This facilitates conversion of guanine triphosphate (GTP) to cyclic guanosine monophosphate (cGMP), activating protein kinase G, which leads to smooth muscle relaxation and vasodilation. Cyclic guanosine monophosphate is converted to guanosine monophosphate by phosphodiesterase 5. Thus, use of phosphodiesterase inhibitors such as sildenafil blocks this conversion, potentiating effects of cyclic guanosine monophosphate. It is essential, therefore, to be aware of potential sildenafil use in patients who may receive cardiac medications and, in particular, nitroglycerin.
- FIGURE 6.
Schematic representation of action of β-agonism in bronchial smooth muscle. Endogenous norepinephrine is released from sympathetic nerve. In extracellular space, endogenous norepinephrine and exogenous salbutamol can couple with β2-receptors. Receptor β2 couples with adenylate cyclase, stimulating G protein to produce decreased intracellular calcium through calcium efflux and uptake in sarcoplasmic reticulum, leading to reduction in actin–myosin bridge formation, producing smooth muscle relaxation and bronchodilation. Inhibition of phosphodiesterase conversion of cyclic adenosine monophosphate (cAMP) to adenosine monophosphate by methylxanthines (e.g., caffeine, theobromine, and theophylline) further decreases intracellular calcium. This response can be antagonized by β-blocker either nonselective (e.g., labetalol) or selective (e.g., butoxamine) for β2. ATP = adenosine triphosphate.

Tables
Drug Indication Dose Pharmacokinetics Mechanism of action Contraindications/cautions Adverse effects/interactions Adenosine Vasodilator stress Alternative approaches are 140 μg/kg/min for 6 or 4 min with radiopharmaceutical administered at 3 or 2 min, respectively Rapid onset, peak < 1 min; half-life < 10 s; duration < 5 min constant infusion; no plasma protein bound Vasodilation through activation of adenosine receptor A2a Contraindicated in atrioventricular block, severe bronchospasm or asthma, known hypersensitivity; use with caution in hypotension, unstable angina, oral dipyridamole therapy, and medications that suppress sinoatrial or atrioventricular nodes; long-standing methylxanthines need cessation for 5 half-lives Adverse effects include chest, neck, jaw, or arm pain, headache, flushing, dyspnea and electrocardiogram changes; bronchospasm is possible, especially in asthmatics; adverse reactions reversed with cessation of infusion; interactions include caffeine/xanthine drugs or foods Dipyridamole Vasodilator stress 0.56 mg/kg intravenously in 20–40 mL of saline over 4 min with radiopharmaceutical administered at end of 4-min infusion or 2 min after completion of infusion 1–2 min until onset; peak at 4 min; half-life of 10–12 h; duration can be prolonged without reversal; 90%–99% plasma protein bound Inhibition of cellular uptake of adenosine to increase availability of endogenous adenosine; vasodilation through activation of adenosine receptor A2a As for adenosine As for adenosine except adverse reactions reversed with aminophylline Regadenoson Vasodilator stress 0.4 mg in 5-mL intravenous bolus followed by 5-mL saline flush and immediate administration of radiopharmaceutical 0.5–2.3 min until onset; duration of 2.3 min; triphasic half-life, with 2–4, 30, and 120 min, respectively; 20%–30% plasma protein bound Vasodilation through selective activation of adenosine receptor A2a As for adenosine except potentially more flexible in mild to moderate airway disease As for adenosine except less bronchoconstriction but does have risk of seizures Dobutamine Stress testing through increasing oxygen demand 10 μg/kg/min intravenously, increasing to 20, 30, and 40 μg/kg/min every 3 min 1–2 min until onset; duration of 10 min; half-life of 2–3 min; 40% plasma protein bound Synthetic catecholamine β2-adrenoreceptor agonist that produces increased rate and force of contraction Contraindicated in hypertrophic cardiomyopathy, uncontrolled hypertension, unstable angina, atrial fibrillation, β-blocker use, and known hypersensitivity; use with caution in myocardial infarction and cardiogenic shock; β-blockers need cessation for 5 half-lives Adverse effects include angina, palpitations, headache, nausea, tachycardia; adverse reactions reversed with cessation of infusion or β-blockers; interactions include blood pressure medications, β-blockers, tricyclic antidepressants, MAOIs, CNS stimulants, potassium-depleting drugs MAOI = monoamine oxidase inhibitors.
Duration is period of significant or measurable effect. Some adverse effects are more likely when used therapeutically than in single interventional doses.
Drug/indication/dose Pharmacokinetics/mechanism of action Contraindications/cautions Adverse effects/interactions Aminophylline/reverse dipyridamole/125–250 mg by slow intravenous infusion Rapid onset and peak; half-life of 8 h; 50%–70% plasma protein bound; antagonizes all adenosine receptors No absolute contraindication; however, caution in patients with porphyria, hyperthyroidism, hypertension, arrhythmia, heart failure, and liver dysfunction Adverse effects include CNS stimulation, gut disturbances, headache, and palpitations; interactions include xanthine products and medications, medications altering liver metabolism, acyclovir, allopurinol, some antiarrhythmics, antidepressants, cimetidine, disulfiram, fluvoxamine, interferon-α, macrolide antibacterials and quinolones, oral contraceptives, tiabendazole, viloxazine, phenytoin and antiepileptics, phenobarbitone, ritonavir, rifampicin, sulfinpyrazone, lithium, macrolides, pancuronium, and phenytoin Nitroglycerin/relieve acute angina/300- to 600-μg sublingual tablet or 1–2 sprays of 400 μg each onto or under tongue or 2- to 3-mg buccal tablet 1–3 min until onset; half-life of 2–3 min; duration of 30–60 min; facilitates nitric oxide metabolism, which causes vasodilation and reduced preload and afterload Contraindicated in hypotension, hypovolemia, and increased intracranial pressure; contraindicated with phenytoin, alteplase, levofloxacin, and sildenafil; caution in renal and liver dysfunction and hypothyroidism Adverse effects include flushing, dizziness, tachycardia and headache; interactions include alcohol, antihypertensives, and vasodilators Salbutamol/relieve dyspnea and bronchospasm/1–2 inhalations of 100 μg each, with third inhalation if necessary 1 min after second 5 min until onset; peak at 60 min; half-life of 4–6 h; duration of 3–6 h; direct-acting β2-agonist to dilate bronchi Contraindicated in hypotension; caution in hyperthyroidism, myocardial insufficiency, hypertension, arrhythmia, and diabetes mellitus Adverse reactions include tremor, palpitations, tachycardia, anxiety, headaches, peripheral vasodilation, muscle cramps, hyperglycemia, and hypersensitivity; interactions with other β2-agonists, corticosteroids, diuretics, xanthines, β-blockers, and antidepressants Some adverse effects are more likely when used therapeutically than in single adjunctive doses.
- TABLE 3
Cessation Medications Commonly Used in Nuclear Cardiology That, in Consultation with Primary Care Physician, Should Be Stopped for 5 Half-Lives of the Medication
Drug Cessation window Comments Nitrates 12–24 h for exercise, vasodilator, and dobutamine stress testing 24 h of cessation should be used for long-acting nitrates; 1 h of cessation can be used for short-acting nitrates delivered in sublingual forms. For patches, cessation commences at time patch is removed β-blockers 48 h for exercise and dobutamine stress testing 24 h is sufficient for those with shorter half-lives, but longer than 48 h may be required for longer half-lives; refer to specific half-life of β-blocker in use for potential variations Calcium channel antagonists 48 h for exercise, vasodilator, and dobutamine stress testing 24 h is sufficient for those with shorter half-lives, but longer than 48 h may be required for longer half-lives; refer to specific half-life of calcium channel blocker in use for potential variations Methylxanthine foods and caffeinated drinks 12–24 h for vasodilator stress testing There is unlikely to be marginal benefit beyond a 24-h cessation; however, 6 h may be sufficient for those with mild consumption; caffeine and theophylline products (coffee, tea) are of importance, but theobromine (chocolate) is less likely to have benefits from cessation Methylxanthine medications 1–5 d for vasodilator stress testing, depending on formulation Refer to specific half-life of medication to determine appropriate cessation period; most medications are theophylline-based or caffeine-containing; thus, 24 h is adequate for most (unless in controlled-release form) Dipyridamole 12–24 h for vasodilator stress testing Half clearance time for dipyridamole should allow cessation period of 12 h to be used if urgent Digoxin 2 wk for exercise and dobutamine stress testing Longer time should be considered in known renal dysfunction





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}