


Abstract
This study investigated differences in cardiac displacement during adenosine stress versus regadenoson stress in 13N-ammonia (13NH3) MP PET/CT scans. Methods: In total, 61 myocardial perfusion PET/CT scans were acquired using either adenosine (n = 30) or regadenoson (n = 31) as a stressor. For both groups, cardiac displacement during rest and stress was measured 3-dimensionally, relative to either a fixed reference frame or the previous frame, in each 1-min frame of a list-mode PET acquisition of 25 min. All stress scans were additionally evaluated for the presence of motion artifacts. Also, the tolerability of the agents and the occurrence of side effects were compared between groups. Results: Significantly larger cardiac displacement during stress was detected in the adenosine group than in the regadenoson group, reflected by both maximal cardiac displacement (P = 0.022) and mean cardiac displacement (P = 0.001). The duration of the movement was typically shorter in the regadenoson group. Frames with cardiac displacement of at least 5 mm were observed nearly twice as frequently when adenosine was used instead of regadenoson. Conclusion: The displacement during regadenoson stress is of lower amplitude and shorter duration than that during adenosine stress and may therefore contribute to a lower incidence of motion artifacts on PET/CT scans.
In the past decade, increased availability of PET/CT has led to a gradual shift from conventional myocardial perfusion (MP) SPECT toward MP PET/CT, using a variety of tracers such as 13N-ammonia (13NH3), H215O, and 82Rb. Apart from superior image resolution and decreased radiation burden for patients, the advantages of MP PET/CT over conventional SPECT are the ability to measure dynamic myocardial blood flow (MBF) and cardiac flow reserve during stress and rest (1–3). Not only can this strengthen a diagnosis of focal ischemia but it also assists detection of global ischemia in balanced significant 3-vessel coronary artery stenosis, an important pitfall in conventional MP SPECT (4). On the other hand, MP PET/CT is vulnerable to patient motion, which may result in artifacts or problems in attenuation correction (AC) algorithms (5,6) that can lead to false image interpretation and false-positive test results. Because MBF measurements and static images of MP are acquired during stress, physical exercise tests are seldom performed in this type of imaging. Instead, pharmacologic stress protocols use stressors such as adenosine, regadenoson, dipyridamole, or dobutamine, which are Food and Drug Administration–approved for this purpose.
Adenosine is the most commonly used coronary vasodilator in MP imaging, has a short half-life of less than 10 s, and nonselectively activates all adenosine receptor subtypes. A variety of side effects, including bronchoconstriction, can be triggered, which may lead to anxiety and undesirable movement in patients during the pharmacologic stress (7,8). A recent study by Hunter et al. has demonstrated that mild to moderate patient motion occurs in over 60% of all MP PET/CT scans using adenosine and that patient motion and resulting cardiac displacement have highly detrimental effects on MBF calculations. Computer phantom simulations have also demonstrated that voxel-based errors can approach up to 500% in extreme scenarios, and larger MBF measurement errors have been shown to occur with larger magnitudes of patient motion (9).
A relatively new addition to the pharmacologic testing arsenal is the adenosine receptor agonist regadenoson (Lexiscan [Astellas Pharma] or Rapiscan [GE Healthcare]), which has a higher affinity for the A2a receptor but much lower affinity for the other adenosine receptor subtypes (10). As a consequence, effects on the airways are less than with adenosine, especially in patients with chronic obstructive pulmonary disease (11), who are prone to develop severe adverse reactions to adenosine. The biologic half-life of regadenoson is 2–3 min and thus substantially longer than that of adenosine. However, regadenoson could be a more patient-friendly option given its favorable binding characteristics and ease of administration (12).
A reduction of cardiac displacement during 13NH3 PET/CT studies would improve the accuracy of the diagnosis. Because regadenoson is known to produce fewer side effects than adenosine during pharmacologic stress tests, it can be hypothesized that less patient motion would be observed with regadenoson during MP PET/CT procedures. A recent retrospective study by Memmott et al. demonstrated this reduction in side effects using 82Rb MP PET/CT (13).
In the present prospective study, patient motion during dynamic 13NH3 PET/CT acquisitions was compared between 2 clinical age- and sex-matched cohorts of patients subjected to either adenosine or regadenoson stress. Also, the occurrence of motion artifacts in the AC 13NH3 PET/CT scans and the experienced side effects of the pharmacologic stressors were compared.
MATERIALS AND METHODS
Patient Inclusion and Preparation
From January 2016 until February 2016, 61 patients, all referred for 13NH3 MP PET/CT, were prospectively included in the study. Thirty patients received adenosine as the pharmacologic stressor, and 31 patients received regadenoson. All patients gave written informed consent for use of their anonymous data for scientific purposes. Because both pharmaceutics are Food and Drug Administration–approved and commonly used as stress test agents with comparable efficacy, the examination was covered by standard care. Besides the standard imaging protocol and clinical management, no additional measurements or actions affecting the patient were performed. The study was approved by the institutional research board; approval of the local ethical committee was not necessary since the study does not fall within the scope of the Dutch Medical Research Involving Human Subjects Act (section 1.b, wet medisch-wetenschappelijk onderzoek [WMO], February 26, 1998).
Patients were asked to remain fasting (except for water) for 6 h before the examination. Patients with diabetes mellitus, however, were allowed to eat, drink, and use insulin as usual. Caffeine-containing beverages were not allowed for 24 h for all patients. Also, patients were not allowed to use dipyridamole or methotrexate derivatives for 12 h (regadenoson) or 24 h (adenosine) before the procedure. Calcium channel and β-blockers could be taken as prescribed by the cardiologist. An intravenous line was inserted in one arm for injection of either adenosine or regadenoson; in patients receiving adenosine, an additional intravenous line was inserted in the contralateral arm for the 13NH3 injection when possible. None of the patients was known to have chronic obstructive pulmonary disease.
Image Acquisition
All images were acquired using a Biograph 16 TruePoint PET/CT system (Siemens Medical Solutions) equipped with a 16-slice CT component and a PET component with 4 rings of lutetium oxyorthosilicate detectors.
A low-dose CT scan (130 kVp, 25 reference mAs, pitch of 0.95) was acquired without a breath-holding command before a 25-min list-mode PET acquisition. Simultaneously with the initiation of the PET acquisition (t = 0 min), 305 ± 4 MBq of 13NH3 were rapidly injected intravenously to obtain PET images at rest. This scan was followed by the administration of the stressor using the second intravenous line, when available. In the case of adenosine, this was done after t = 12 min with a dose of 140 μg/kg/min during 6 min. In the case of regadenoson, this was done after t = 14:20 min using a single bolus of 400 μg (5 mL in 10 s) followed by a 10-mL saline flush (in 10 s). At t = 15 min, a second dose of 394 ± 3 MBq of 13NH3 was administered. Blood pressure was automatically measured twice during the procedure at 1 min after each 13NH3 administration.
Image Reconstruction
Standard static, dynamic, and 16-bin electrocardiography-gated reconstructions were obtained, as well as 25 additional dynamic reconstructions (60 s per frame, TrueX reconstruction algorithm including a point-spread function correction) for analysis of cardiac movement during the PET acquisition. These frames were generated with a 168 × 168 matrix, 3-mm slice thickness, zoom of 2, gaussian filter of 5 mm in full width at half maximum, 4 iterations, and 8 subsets. Series of frames were assigned as the various acquisition components, which are displayed in Figure 1.
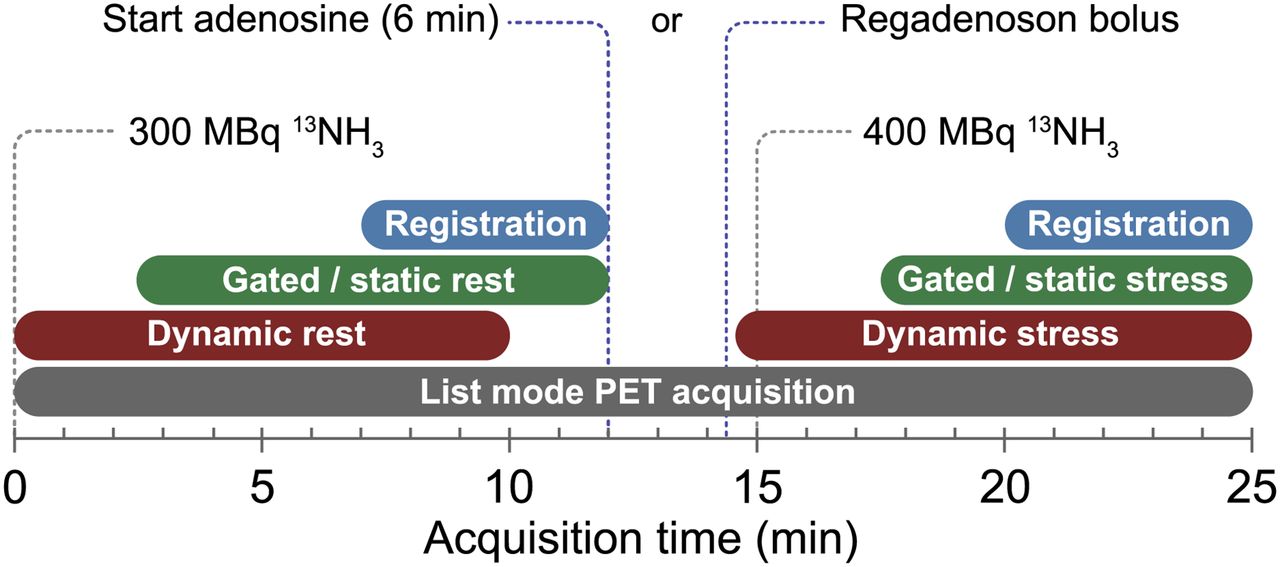
Components of rest and stress acquisitions (adenosine or regadenoson).
Image Analysis
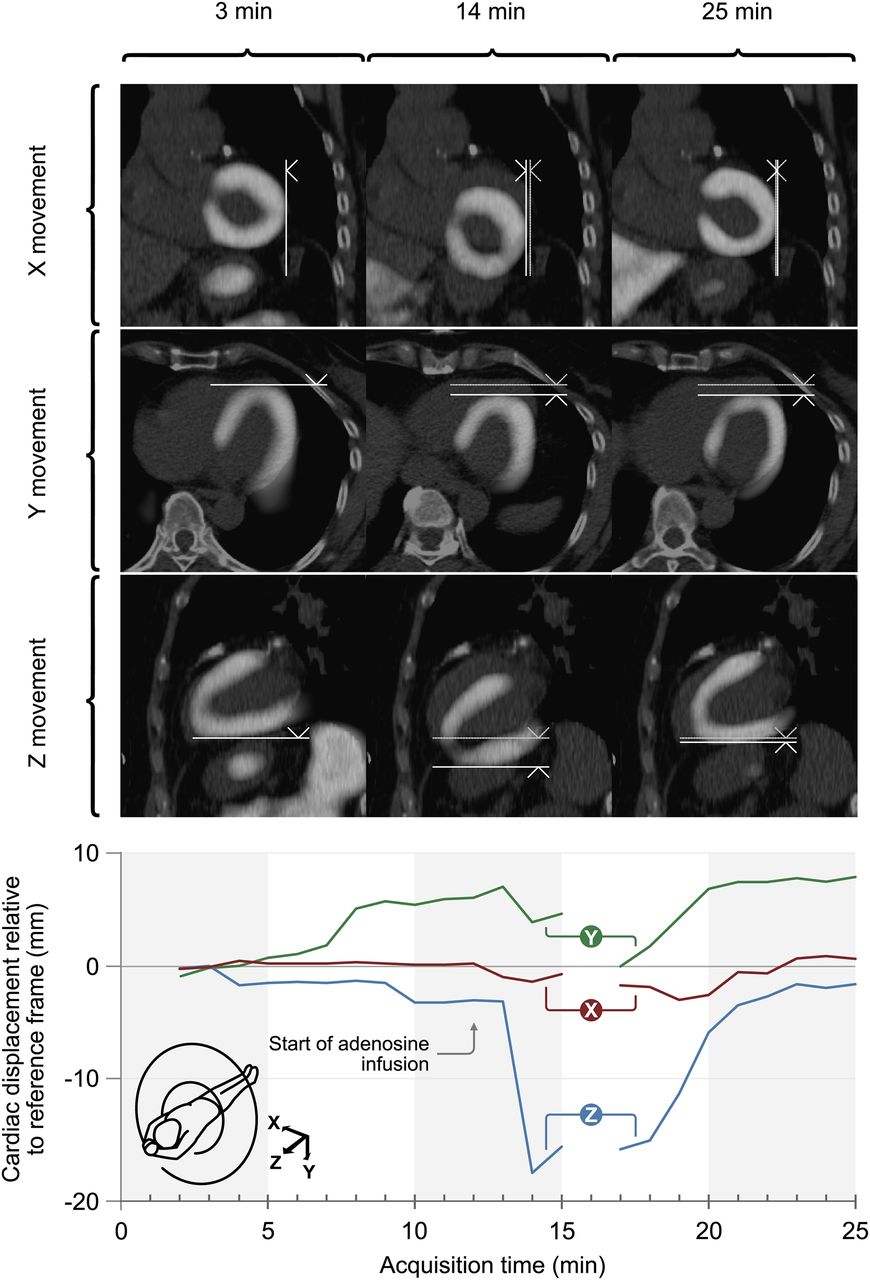
A heart-specific motion correction algorithm developed by Siemens Molecular Imaging was used to automatically detect displacement of the myocardium between dynamic frames. Cardiac displacement was determined by rigid image registration between each of the frames and a reference frame. Frame 3 (the first available PET image after the AC CT scan) was used as the reference frame to determine cardiac movement by the automatic motion-correction software, since myocardial activity was still absent from frames 1 and 2 and obscured by blood-pool activity. Myocardial visualization was also hampered by blood-pool activity in frame 16, which was therefore excluded from analysis. Both rotation and translation of the registration matrix were evaluated visually by overlaying the motion-corrected target image on the source image and comparing with the non–motion-corrected image pairs. Cardiac displacement between frames was measured in millimeters in 3 dimensions, either positive or negative, using the automatic motion-correction algorithm. Positive cardiac displacement along the x-axis was defined as movement of the patient from right to left; positive displacement along the y-axis, from ventral to dorsal; and positive displacement along the z-axis, from caudal to cranial (Fig. 2, bottom). The length of a single displacement vector in 3-dimensional space was then calculated from the cardiac displacement obtained in 3 directions and verified visually. As an internal validation of the algorithm, displacement of the reference frame against itself was determined for all datasets and was below 0.3 mm on average in all axes. Occasionally, frame 2 or 4 was used as the reference frame when automated myocardial contour detection was suboptimal in frame 3. Additionally, cardiac displacement was calculated relative to the previous available frame to obtain a more detailed description of the displacement pattern.

(Top) Example of cardiac displacement during adenosine stress. Displacement is depicted in coronal, transverse, and sagittal planes in x, y, and z directions, respectively. Images represent data obtained at 3 min after scan initiation (frame 3; reference frame), at 14 min (2 min after initiation of adenosine), and at 25 min (last frame of stress acquisition). Bolder vertical and horizontal lines in each tile of 14- and 25-min series represent displacement relative to initial position of heart (fainter lines). (Bottom) Displacement in x, y, and z directions in this patient during entire scan, relative to reference frame (at 3 min after initiation of scan).
Cardiac displacement during the rest acquisition was compared between the adenosine and regadenoson groups, and the maximum and mean of the cardiac displacement during the rest acquisitions were obtained within frames 2–12. Next, the cardiac displacement during pharmacologic stress was evaluated between those groups. The maximum and mean of the displacement during stress acquisitions were obtained within frames 13–25 for adenosine and frames 15–25 for regadenoson. Additionally, cardiac displacement was compared between the rest acquisition and the pharmacologic stress acquisition of both the adenosine and the regadenoson groups. The maximal displacement during each acquisition was categorized as minor (<5 mm), medium (5–10 mm), or large (>10 mm) relative to the reference and previous frames. The number of patients displaying medium and large cardiac displacement during pharmacologic stress was compared between the adenosine and regadenoson groups. Also, the total number of frames that showed medium or large cardiac displacement was counted in all PET/CT procedures for both study groups as a measure of duration of cardiac displacement during pharmacologic stress.
Visual Appraisal of Motion Artifacts on PET/CT Scans
All anonymized 13NH3 myocardial PET/CT stress scans were reviewed visually by 2 experienced nuclear medicine physicians, masked to the used protocol, for the presence of motion artifacts on static images. For this analysis, AC and non-AC static images were compared, and dynamic series were reviewed when necessary. Detected artifacts were categorized in consensus as small, intermediate, or large.
Survey of Side Effects
Patients were interviewed by a physician assistant after completion of the procedure, using a standard questionnaire. The symptoms were categorized as none, typical chest pain, respiratory, gastrointestinal, vasodilator, or other. Also, the general degree of discomfort of the procedure was categorized as very inconvenient, inconvenient, tolerable with little discomfort, or no discomfort at all.
Statistical Analysis
SPSS, version 20.0 (IBM Corp.), was used for statistical analysis. The Kolmogorov–Smirnov test was used to evaluate for a normal distribution of data. Continuous variables with a normal distribution are presented as mean ± SD, and categoric variables, as frequencies with percentages. Student t tests were used to compare variables with a normal distribution. Mann–Whitney tests were performed to detect differences in nonnormally distributed cardiac movement during the various acquisitions, and data were additionally expressed as median and interquartile range. For analysis of the relationship between categoric variables, Pearson χ2 tests were performed. When appropriate, tests were 2-sided, and in all tests, P values of 0.05 or less were considered significant.
RESULTS
Patient Population
In total, 61 patients referred for MP PET/CT were included. Baseline characteristics are detailed in Table 1. There were no significant differences between mean age, sex, average body mass index, or Duke Clinical Score (14–16) between the adenosine and regadenoson groups.
Baseline Characteristics, Known Risk Factors, Stress Test Parameters, and Clinical PET/CT Diagnosis
Cardiac Movement During Stress Acquisition
An example of cardiac movement in the x, y, and z directions relative to the reference frame at various time points during an adenosine stress test is displayed in Figure 2.
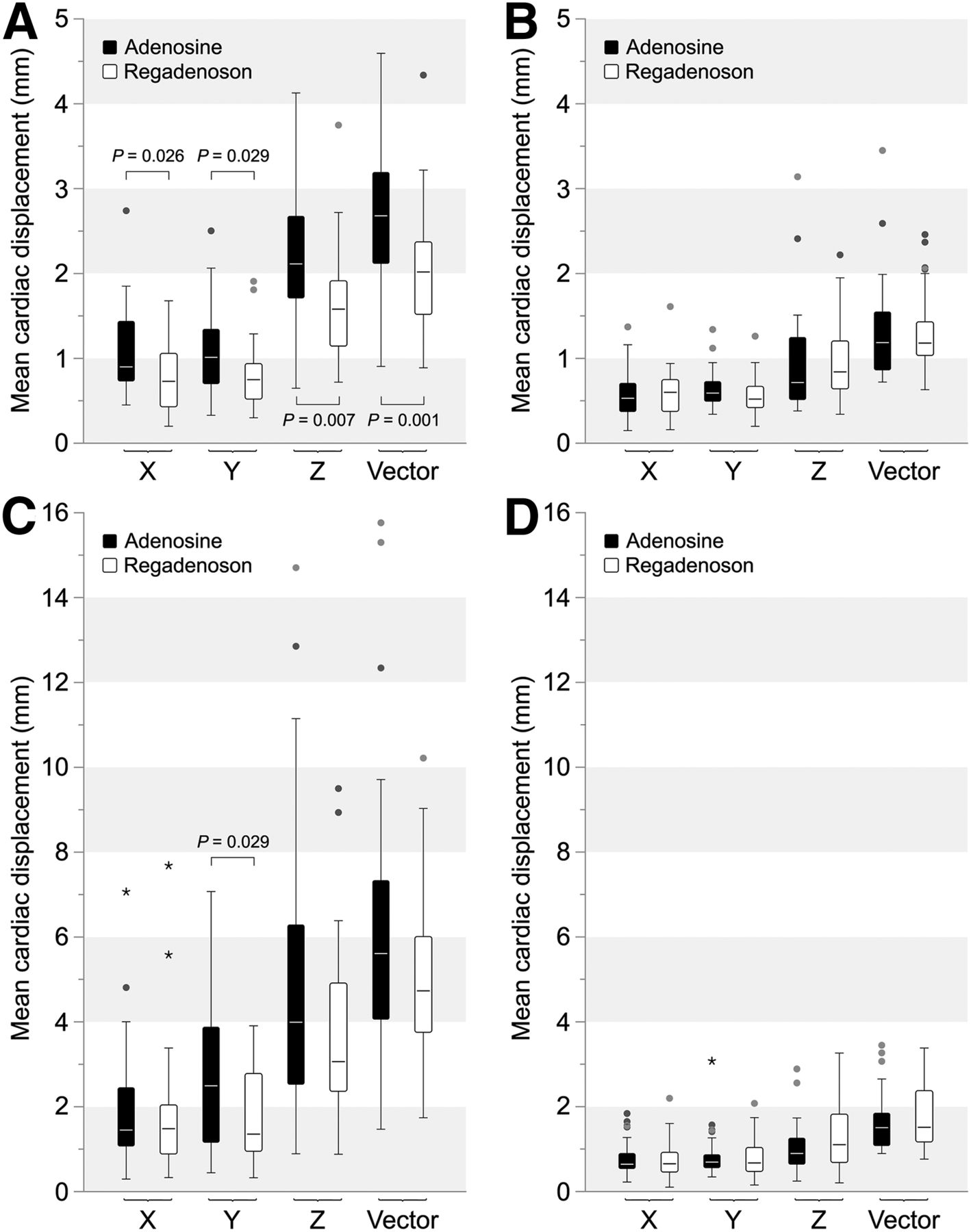
A significantly larger cardiac displacement relative to the previous available frame was detected in patients subjected to adenosine stress than in those receiving regadenoson. This difference was reflected in both maximal cardiac displacement (mean ± SD, 8.1 ± 3.7 vs. 6.1 ± 2.3 mm; P = 0.022) and mean cardiac displacement (median, 2.7 mm [interquartile range, 2.1–3.2 mm] vs. 2.0 mm [interquartile range, 1.5–2.4 mm]; P = 0.001), as represented by the total vector (Tables 2 and 3 [maximum cardiac displacement]; Fig. 3A [mean cardiac displacement]). There were no significant differences in maximum (mean ± SD, 3.8 ± 1.9 vs. 3.8 ± 1.5 mm; P = 0.593) or mean cardiac displacement (P = 0.155) between adenosine rest acquisitions and regadenoson rest acquisitions (Tables 2 and 3; Fig. 3B). A significantly larger mean cardiac displacement was detected during the stress than the rest acquisition for both the adenosine (P < 0.001) and the regadenoson (P < 0.001) groups.
Maximal Displacement in 3 Axes During Stress Acquisitions* Using Previous Frame or Frame 3 as Reference
Maximal Displacement as Vector Length During Rest and Stress Acquisitions Using Previous Frame or Frame 3 as Reference
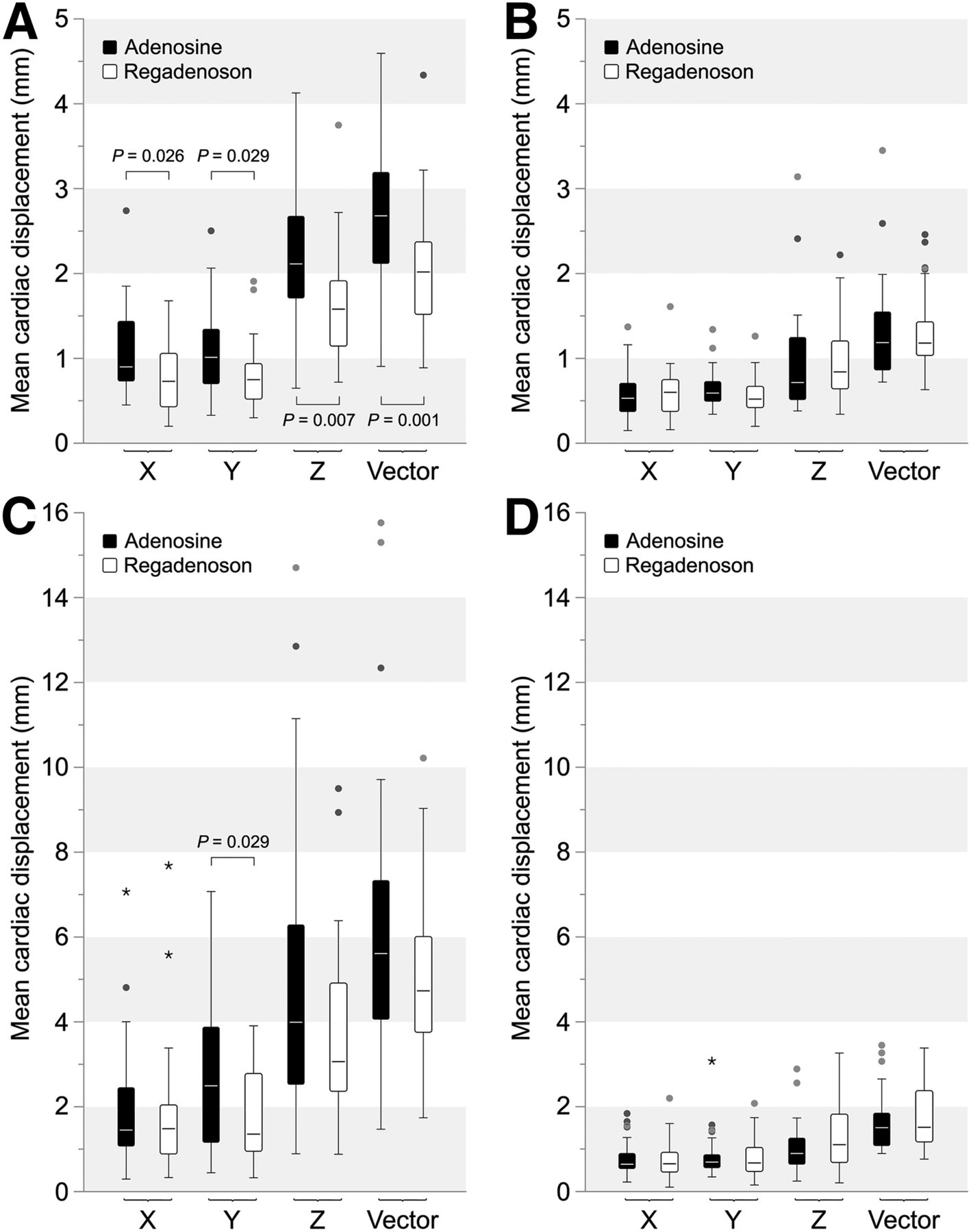
Median with interquartile ranges of mean cardiac displacement in x, y, and z directions and total displacement vector length for both adenosine and regadenoson. (A) Displacement during stress relative to previous available frame. (B) Displacement at rest. (C) Displacement relative to reference frame (frame 3) during stress. (D) Displacement relative to reference frame at rest. Statistical analysis was performed using Mann–Whitney tests.
Cardiac displacement relative to the reference frame is displayed in Tables 2 and 3 and Figures 3C and 3D. A significant difference in maximum cardiac displacement was detected between the 2 groups (mean ± SD, 11.6 ± 5.2 for adenosine vs. 8.6 ± 3.0 mm for regadenoson; P = 0.014). Although both the median and the interquartile range of mean cardiac displacement were higher for the adenosine stress datasets, a significant difference during stress was present only in the y direction (P = 0.029).
The mean vector of cardiac displacement during the entire acquisition and the absolute values of the mean displacement in 3 dimensions are plotted in Figure 4 for the adenosine (Figs. 4A and 4C) and regadenoson (Figs. 4B and 4D) groups. The plotted data clearly show increased displacement during administration of adenosine, compared with tests performed with regadenoson. The heart was displaced most in the z-axis, especially in the adenosine group, and to a lesser extent in the y-axis. The figure also shows that cardiac displacement relative to the reference frame persisted longer in the adenosine group than in the regadenoson group. Substantial cardiac displacement, when defined as displacement of at least 5 mm relative to the reference frame, was present during 8 consecutive minutes in the adenosine group versus 3 min in the regadenoson group.

Cardiac displacement during stress and rest acquisitions in x, y, and z directions and total displacement vector length (dotted line). Data represent mean of all patients relative to reference frame (frame 3) (A and B) or relative to previous frame (C and D). (A and C) Displacement during adenosine stress. (B and D) Displacement during regadenoson stress. Gaps in plots are result of exclusion of frames because of high blood-pool activity after injection of 13NH3.
Compared with the previous available frame, medium displacement (5–10 mm) was detected in more than half of the patients in both the adenosine and the regadenoson groups (Table 4). Large displacement (>10 mm) of the heart, relative to the reference frame, was more prevalent in the adenosine group. The total number of analyzed frames in the adenosine group, as opposed to the regadenoson group, yielded a small but higher fraction of frames with medium cardiac displacement relative to the previous frame. Large cardiac displacement compared with the previous frame was detected in only a few frames in the adenosine group and in only one frame in the regadenoson group (Table 4). Similar results were found when frame 3 was used as a reference, although relatively more patients in the adenosine group showed large cardiac displacement (Table 4). The number of frames displaying medium or large cardiac displacement relative to the reference frame, as a measure of the duration of that displacement, was higher during stress in the adenosine group than in the regadenoson group.
Total Number of Frames of All Patients with Minor, Medium, and Large Displacement During Stress Acquisition Using Previous Frame or Frame 3 as Reference
Both adenosine and regadenoson stress acquisitions demonstrated a peak in cardiac displacement after administration of the stressor. However, the cardiac displacement was generally larger during adenosine stress (Tables 2 and 3; Figs. 3A, 3C, and 4).
Visual Appraisal of Motion Artifacts on PET/CT Scans
Compared with the adenosine group, the regadenoson group showed fewer motion artifacts on stress 13NH3 PET/CT: 14 of 30 patients (46.7%) versus 9 of 31 patients (29.0%) (P = 0.192), respectively. No artifacts were graded as large. Medium-sized artifacts were found in 2 of 30 patients (6.7%) in the adenosine group, compared with none in the regadenoson group. The remainder of the patients displayed small artifacts: 12 of 30 patients (40.0%) in the adenosine group and 9 of 31 patients (29.0%) in the regadenoson group.
Tolerability of Adenosine and Regadenoson
The patient survey did not show differences in side effects between the adenosine and regadenoson groups (Table 5). Respiratory symptoms were reported by 16 patients (53.3%) in the adenosine group and 11 patients (35.5%) in the regadenoson group (P = 0.095). Typical chest pain, gastrointestinal side effects, vasodilatation-related side effects, and a variety of other side effects were reported by patients of both groups, and no significant differences were found. The overall patient experience with respect to the pharmacologic stressors was also similar between the adenosine and regadenoson groups (P = 0.428), as patients graded both test protocols as equally inconvenient.
Reported Symptoms During Stress Acquisition
DISCUSSION
Cardiac displacement during acquisition is the principal source of artifacts in MP PET/CT and may lead to erroneous interpretation. It is well known that CT-based AC can introduce artifacts in PET images due to misregistration (17). The present study points out that cardiac displacement occurs more frequently, and with higher amplitude and longer duration, when adenosine rather than regadenoson is used, possibly because of physical complaints, anxiety, or panic during the stress study. Motion artifacts were approximately 50% more prevalent in adenosine acquisitions than in regadenoson acquisitions and were present in almost 50% of the adenosine scans. Before MP PET/CT, each patient should be positioned comfortably and instructed thoroughly to reduce cardiac displacement due to patient movement. During the stress acquisition, the capability of communication between the nuclear medicine physician or a well-trained technician and the patient should be ensured, not only for safety reasons but also to reassure the patient and, thus, help avoid anxiety or panic. Despite such precautionary measures, artifacts arising from patient or cardiac movement cannot always be prevented. Another, more intrinsic, cause for cardiac displacement during pharmacologic stress may be the well-known urge to breathe deeply (18,19) during administration of the stress test agent, which may lead to a temporary alteration of the anatomic position of the heart due to diaphragm displacement. Although impossible to prove this cause for displacement with the present data, the observed displacement agrees with this possibility, especially but not exclusively in the adenosine group. Literature on motion artifacts in MP PET/CT imaging is scarce, particularly for 13NH3 MP PET/CT performed with adenosine or regadenoson. However, our study is in line with a recently published retrospective study by Memmott et al. in which data acquisition began 210–240 s after initiation of adenosine or 40 s after regadenoson injection (13). The present study reports cardiac movement in 3 dimensions in a wider time frame, that is, during and between the rest and stress acquisitions, yielding additional insight on the movement pattern at early stages of the stress procedure. We found the largest cardiac shift to be along the z-axis, directly after initiation of adenosine infusion and to a lesser extent after regadenoson administration, which could result from a change in breathing pattern. By the end of the adenosine infusion, we also observed a movement of the heart to its initial position.
When cardiac displacement occurs after CT acquisition but before PET acquisition, the AC map can usually be adjusted properly using the reconstruction software by applying a registration matrix between the PET and CT images. This matrix can be obtained by manual or automatic realignment of the non-AC PET images and CT images. However, if patient or solely cardiac movement occurs during the PET acquisition, it is impossible to apply proper CT AC to the entire acquired PET dataset. In such a case, one can consider reconstructing 2 datasets (before and after the displacement) for both static and gated images and applying a proper registration matrix for better AC. There are, however, disadvantages to this approach (e.g., fewer counts), and it does not apply to dynamic studies. It is also ineffective when multiple movements occur during PET acquisition. Detrimental misalignment effects have been described previously both for static PET acquisitions (AC-induced artifacts) (17) and for dynamic acquisitions (errors in MBF calculations) (20).
Generation of frame-specific registration matrices could potentially solve the problem of misregistration due to cardiac movement for dynamic frames with AC. To date, such software is unavailable, at least for Siemens PET/CT systems. At present, only one registration matrix can be applied to all dynamic frames, therefore potentially leading to AC errors when applied to specific time points. Another problem for the accuracy of MBF calculations is the inability to correct for cardiac displacement during early dynamic frames, potentially leading to misplacement of myocardial and intraventricular regions of interest when movement occurs during this phase. Obviously, the measured time–activity curves and MBF calculations might be affected. Therefore, reducing cardiac displacement during a cardiac PET acquisition improves the accuracy of the diagnosis. PET/MRI scanners could also potentially solve the problem with misalignment. Simultaneous acquisition of MR and PET images can provide a frame-specific MR-based AC for each dynamic PET frame. This ability would avoid errors in MBF calculations introduced by incorrect AC. Currently, in the absence of proper AC for individual dynamic frames, a quantitative indication of the average and maximum cardiac displacement between reconstructed dynamic frames could give clinicians a way to assess scan quality in addition to visual appraisal of the blood input function. Datasets with large cardiac displacement could be considered less reliable. Such quantitative analysis could easily be incorporated in commercial MBF analysis software but is, to our knowledge, unavailable at present.
Other options for motion artifact reduction include replacement of both adenosine and regadenoson with other pharmacologic stressors, such as dobutamine or dipyridamole. Dobutamine is impractical for routine use in 13NH3 MP PET/CT since it is uncertain at what time point the required heart rate is achieved after initiation of the stressor. Also, in a study by Hunter et al. (9) using the indirect coronary vasodilator dipyridamole as a stressor, motion artifacts were reported (in ≤60% of all clinical scans) together with detrimental effects on MBF calculations. Although dipyridamole less frequently leads to side effects, especially less shortness of breath, these effects are generally less tolerated and last longer, because of the longer biologic half-life of the pharmaceutical (40 min vs. <10 s). Side effects may last for 15–25 min, with theophylline occasionally being required to terminate the effects, whereas the effects of adenosine resolve rapidly within minutes after the test (21). Besides, Vasu et al. found that in cardiovascular MRI, dipyridamole was less efficacious than either adenosine or regadenoson, yielding lower MBF and cardiac flow reserve values (22).
A limitation of the present study was the relatively small cohort of 61 patients: the statistical power appeared to be insufficient for us to draw solid conclusions on differences in patient symptoms or scan results (particularly by visual appraisal) between subgroups, and in our relatively small cohort a correlation between the degree of discomfort and the extent of cardiac displacement appeared nonexistent (r2 = 0.12 for adenosine and 0.01 for regadenoson). Also, heterogeneity within the cohorts existed because some patients were already known to have cardiovascular disease, although movement patterns appeared to be similar.
Another source of error could be the residual-activity-correction algorithm, which was based on a combination of background subtraction and modeling for estimation of rest and stress blood flow. The residual activity from the rest injection was quantified using the first frame of the stress study (acquired during 30 s before the stress injection). The blood input function and time–activity curves obtained from the stress acquisition were corrected by subtracting the residual activity from all frames of the decay-corrected time–activity curves and blood input function (23). In daily clinical practice, this step effectively eliminates interference from residual activity in our time-efficient MP PET/CT protocol.
Finally, despite extensive local experience with 13NH3 MP PET/CT in more than 2,500 studies thus far, response and observer bias cannot be ruled out completely. Nonetheless, the findings of the present study may be relevant and helpful to institutions that are designing stress protocols and are willing to perform this type of PET/CT examination.
Adenosine is an effective and inexpensive stress test agent and has been produced by large numbers of pharmacies for decades. After regadenoson was registered in 2008, it was added to the pharmacologic stressor inventory, and it has since been used frequently in patients with chronic obstructive pulmonary disease, with fewer side effects being observed than for adenosine (24). Unfortunately, regadenoson is considerably more expensive than adenosine. However, whether the benefits of fewer motion artifacts and better tolerability by patients could outweigh the substantially higher costs remains to be determined. Future studies on cost-effectiveness need to include factors such as savings from the need for fewer additional diagnostic procedures (e.g., coronary angiography) and from more accurate treatment (e.g., revascularization procedures).
CONCLUSION
Patients undergoing adenosine MP PET/CT demonstrate a cardiac displacement pattern significantly different from that of patients receiving regadenoson. The cardiac displacement pattern is of lower amplitude and shorter duration during regadenoson stress than during adenosine stress and may contribute to the lower incidence of motion artifacts on PET/CT scans.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Vivian Barten for performing the imaging studies, Tjeerd van der Ploeg for helping with statistics, and Evert-Jan Woudstra for providing technical support.
Footnotes
Published online Dec. 22, 2017.
REFERENCES
- Received for publication August 3, 2017.
- Accepted for publication November 28, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.