


Abstract
Our objective was to test the hypothesis that variability in SUV normalized by skeletal volume (SV) in 18F-fluoride (18F-NaF) PET/CT studies is lower than variability in SUV normalized by body weight (BW). Methods: The mean SUV (SUVmean) was obtained for whole skeletal volume of interest (wsVOI) in 163 selected 18F-NaF PET/CT studies. These studies were performed to investigate bone metastases and were considered to have normal results. SUVmean was calculated with normalization by BW (BW SUVmean), with normalization by SV (SV SUVmean), and without normalization (WN SUVmean). The total SV for each patient was also estimated on the basis of the wsVOI defined on the CT component of the PET/CT study. SUVmean variability for each patient was estimated as the absolute value of the difference between the SUVmean for the patient and the mean of the SUVmean for the whole group of patients, divided by the mean of the SUVmean for the whole group of patients. The variabilities of SUVmean calculated by the 3 methods were compared using a paired 1-tailed Wilcoxon test. Results: The mean variability for the BW, SV, and WN SUVmean was 0.16, 0.13, and 0.16, respectively. There were statistically significant differences between SV and BW SUVmean variability (P = 0.03) and between SV and WN SUVmean variability (P < 0.01). There was no statistically significant difference between BW and WN SUVmean variability (P = 0.4). Conclusion: In patients with normal 18F-NaF PET/CT results, SV SUVmean presents lower variability than BW SUVmean.
The SUV is often used in PET imaging for semiquantitative analysis (1). SUV is defined as the tissue concentration of tracer as measured by a PET scanner, divided by the activity injected per unit volume of distribution, frequently the body weight (BW) (2).
Although SUV has been used predominantly for 18F-FDG PET/CT imaging quantification, it can also be used with other PET tracers. The use of SUV in 18F-fluoride (18F-NaF) PET/CT studies has been described (3,4). There are reports demonstrating that SUV can detect significant metabolic alterations in individual metastatic lesions on 18F-NaF PET/CT images, even when visual evaluation reveals little, if any, difference (5). Moreover, SUV measurement may provide additional information in assessing treatment response using 18F-NaF PET/CT studies (5,6).
However, to properly use SUV in clinical practice, it is important to be aware of factors that can alter these values. For calculating SUV in 18F-FDG PET/CT studies, some authors prefer to use lean body mass (7) or body surface area (8) as a measure of the distribution of the radiopharmaceutical, instead of the more frequently used BW. Zasadny and Wahl (7) stated that if there is no significant uptake of 18F-FDG in fat tissue, lean body mass instead of total BW should be used as a measure of the volume of radiopharmaceutical distribution. There are articles proposing that lean body mass SUV is independent of BW (7,9), and this methodology has also been advocated as preferable for quantifying metabolic activity when assessing treatment response in clinical trials (10). There are also articles discussing the best methods to estimate lean body mass in 18F-FDG PET/CT studies. Although predictive equations are adequate for lean body mass estimation (11), methods based on CT images are more accurate (12,13).
Because 18F-NaF has a nonhomogeneous distribution in the body, with predominant bone uptake and minimal soft-tissue uptake, we hypothesized that SUV normalization by skeletal volume (SV) may be more appropriate than normalization by BW for this radiopharmaceutical and may provide less variable results.
Our objective was to test the hypothesis that in 18F-NaF studies, variability is lower for SUV normalized by SV than for SUV normalized by BW.
MATERIALS AND METHODS
Patient Population
The institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived.
We analyzed 18F-NaF PET/CT studies performed on 163 patients. These studies were retrospectively selected from a database of more than 2,000 18F-NaF PET/CT studies performed in our institution to investigate bone metastasis in patients with oncologic diseases. The selection criterion was visually normal or near-normal radiopharmaceutical uptake in the skeleton on PET and CT images. Patients with chronic renal failure were also excluded. The patient characteristics are presented in Table 1.
Characteristics of Patients
PET/CT Image Acquisition
The patients were injected with around 185 MBq of 18F-NaF and, about 60 min afterward, underwent whole-body (vertex to toes) 3-dimensional PET/CT. Images were acquired on a Discovery 690 time-of-flight PET/CT scanner (GE Healthcare) with a 64-slice CT component. Emission PET images were obtained at 1 min per bed position (15-cm axial field of view with 3 cm of overlap), with 13–15 bed positions per study. CT transmission scans (30 mAs) were obtained for attenuation correction. Other CT acquisition parameters were 120 kVp, 0.5-s rotation time, 1.375 pitch, and 3.75-mm axial slice thickness. PET images were reconstructed using ordered-subsets expectation maximization with 2 iterations and 24 subsets. CT image reconstruction was based on conventional filtered backprojection with the GE Healthcare Bone Plus filter.
Image Analysis
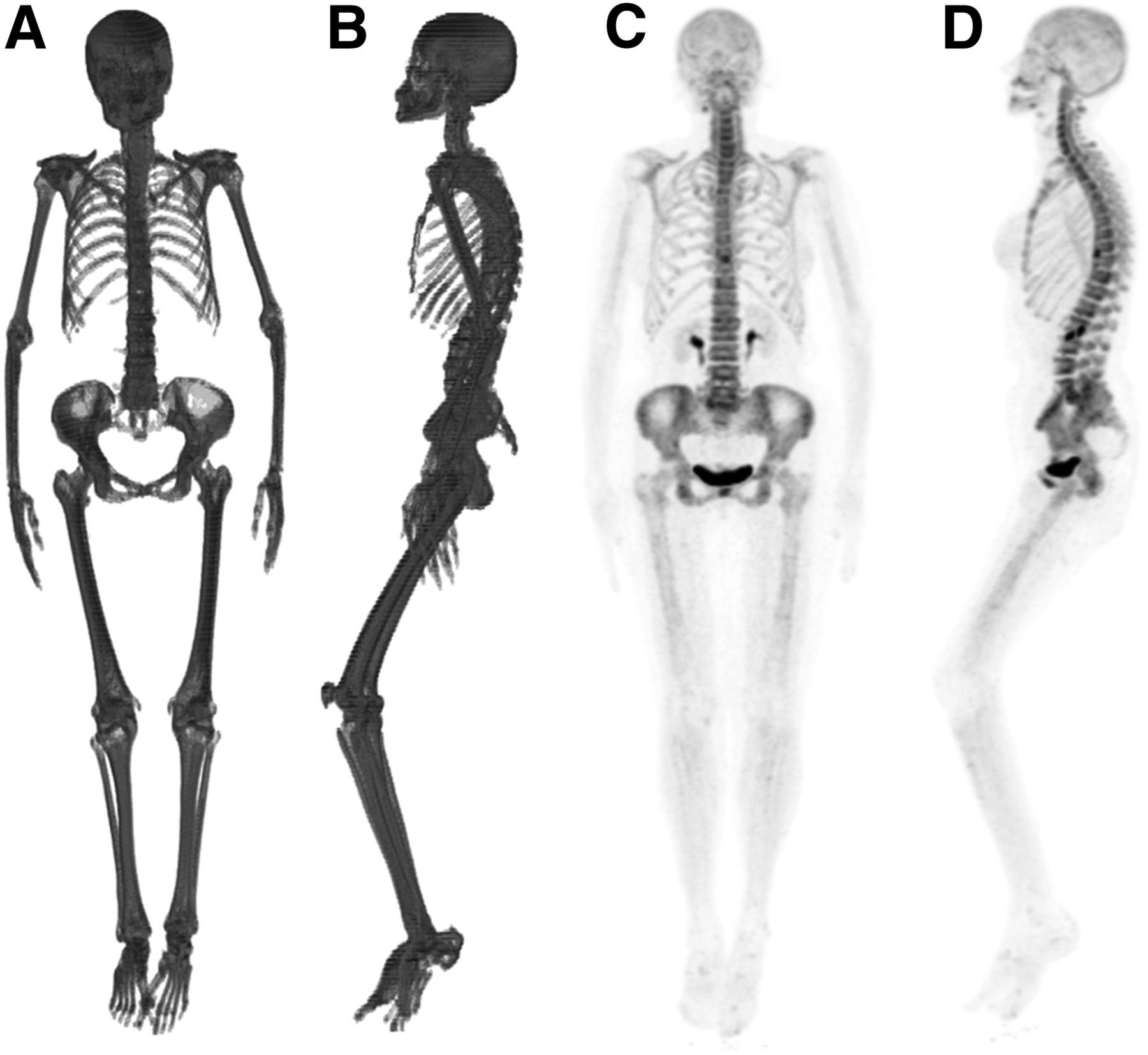
SUVmean normalized by BW (BW SUVmean) was obtained in whole skeletal volume of interest (wsVOI) for the 163 selected 18F-NaF PET/CT studies. The wsVOI was automatically defined on the CT component of the PET/CT studies, using AMIDE software (14). A threshold of 120 HU was used to separate bone from soft tissues. The BW SUVmean in the wsVOI was automatically calculated by the software. The total SV for each patient was also automatically estimated by the software based on the whole SV of interest (Table 1). Therefore, the wsVOI was used to estimate the BW SUVmean in the whole skeleton and the total volume of the skeleton. An example of a wsVOI is presented in Figure 1.
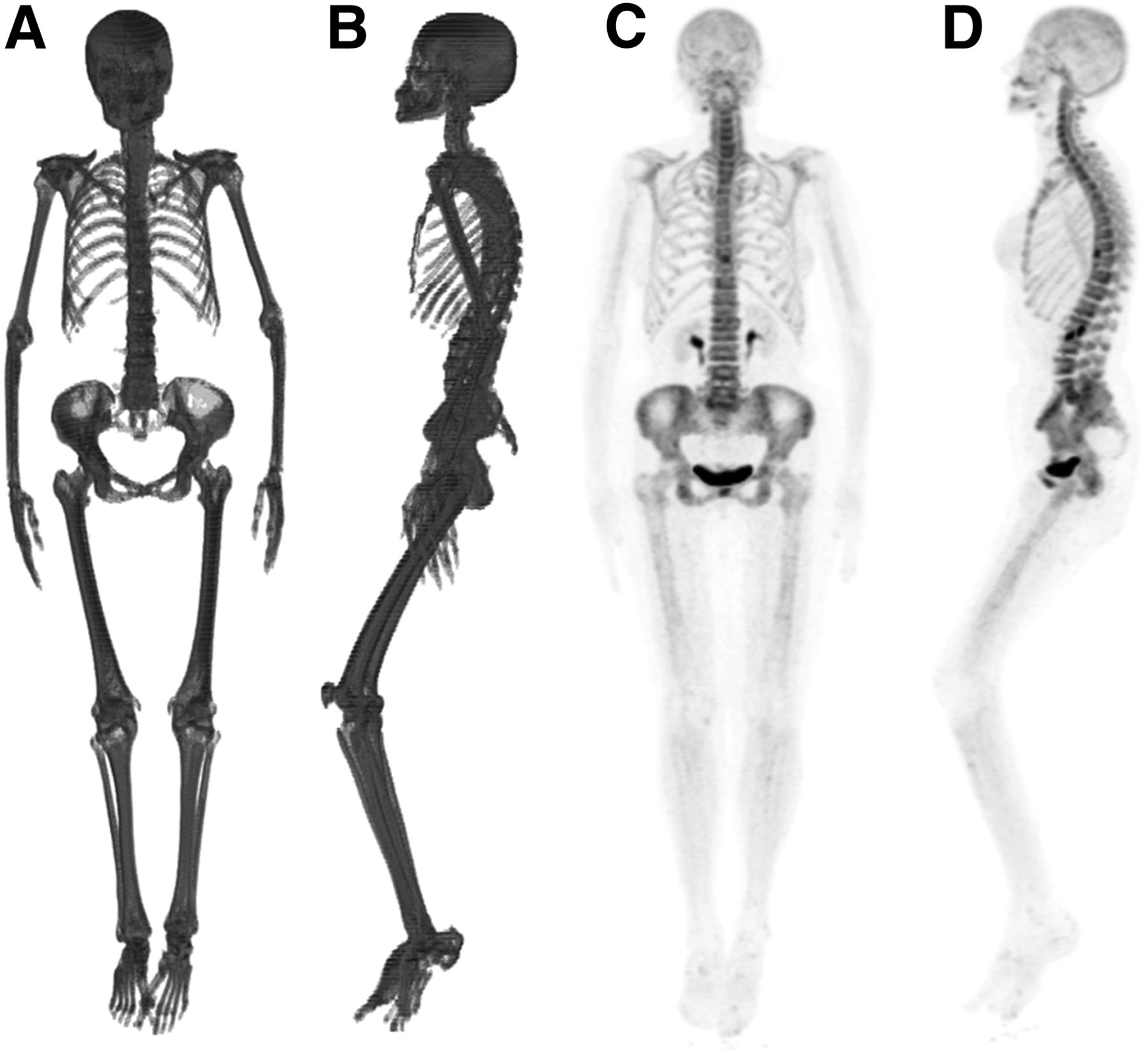
Coronal (A) and sagittal (B) 3-dimensional volume-rendered projections of wsVOI and corresponding coronal (C) and sagittal (D) maximum-intensity projections of near-normal 18F-NaF PET study (BW SUVmean, 2.65; SV SUVmean, 0.25; WN SUVmean, 0.05; SV, 5.3 L).
SUVmean normalized by SV (SV SUVmean) for each patient was calculated on the basis of the BW SUVmean and on SV using the following equation: Eq. 1
Eq. 1
The SUVmean without normalization (WN SUVmean) was also calculated. This calculation was performed to assess whether the 2 analyzed normalization methods (BW and SV) have any impact on the variability in SUVmean when compared with SUVmean calculated without normalization (WN).
WN SUVmean for the whole skeleton was calculated using the following equation: Eq. 2
Eq. 2
Statistical Analysis
The variability in whole-skeleton SUVmean is defined as follows: Eq. 3
Eq. 3
where ABS is absolute value of SUV variability for each patient, SUVmean is the mean SUV in the wsVOI for each patient, and the mean SUVmean is the mean value of SUVmean for the whole group of patients.
The means, SD, and maximal values of variability obtained using the 3 SUV normalization methodologies were calculated and then compared using a paired 1-tailed Wilcoxon test.
Statistical analysis was performed using Excel 2007 (Microsoft Inc.) and SPSS statistics 20 (IBM Corp.).
RESULTS
The means, SD, minimum, and maximum values of the SUVmean normalized by the 3 methodologies are presented in Table 2.
Whole-Skeleton SUVmean Normalized by BW, SV, and WN for 163 Studies Analyzed
The means, SD, minimum, and maximum values of variability obtained using the 3 methodologies are also presented in Table 2. The mean variability for BW, SV, and WN SUVmean was 0.16, 0.13, and 0.16, respectively (Table 2). The maximum variability for BW, SV, and WN SUVmean was 0.62, 0.47, and 0.67, respectively (Table 2).
The paired 1-tailed Wilcoxon test showed statistically significant differences between the variabilities of SV and BW SUVmean (P = 0.03) and between the variabilities of SV and WN SUVmean (P < 0.01). There was no statistically significant difference between the variabilities of BW and WN SUVmean (P = 0.4).
DISCUSSION
In the last few years, there has been a renewed clinical interest in the use of 18F-NaF as a bone scanning agent (15). Reasons for this resurgence include periodic worldwide shortages of 99mTc, which is needed to label radiopharmaceuticals for bone scanning (16), and the improved sensitivity (17–19) and quantitative potential (5,6) of 18F-NaF PET/CT over technetium-based conventional bone scans.
Despite this quantitative potential, the main form of analysis for 18F-NaF PET/CT studies has been visual interpretation. However, the scientific literature shows that SUV could be useful in some situations. Kubota et al. (20) investigated the usefulness of 18F-NaF PET as a predictor of femoral head collapse in patients with osteonecrosis before radiographic changes occur. They concluded that quantitative assessment of SUVmax in 18F-NaF PET was useful in predicting collapse. Waterval et al. (21) assessed uptake of 18F-NaF in patients with otosclerosis and evaluated its use as a complementary diagnostic tool. They concluded that 18F-NaF PET using SUV measurements has the potential to be a diagnostic tool in otosclerosis. Cook et al. (5) evaluated the use of 18F-NaF PET with SUV analysis as an alternative biomarker of bone metastasis response to 223Ra-chloride treatment. They concluded that SUV is more accurate than qualitative comparison of scans in assessing response. In more recent papers, techniques to measure the burden of bone disease have been demonstrated (22), and such measurements have been associated with prognosis (23). In those articles, the volumes of interest were based on metabolic uptake and SUV thresholds. Therefore, the adequate use of SUV is fundamental in some clinical situations. However, to properly use SUV in clinical practice, it is important to establish factors that can impact the values.
In the present article, we proposed a technique to normalize SUVs by SV instead of by BW when evaluating 18F-NaF PET bone images. In this technique, the SV is based on bone boundaries defined on the CT component of the PET/CT study using AMIDE software, a free tool for analyzing medical imaging (14). The rationale behind this normalization is the high specific uptake of 18F-NaF by bone and the minimal uptake by soft tissues. Our analyses demonstrated that whole-skeleton BW SUVmean is more variable than whole-skeleton SV SUVmean. This phenomenon could be explained by the fact that when SUV is measured in a wsVOI and normalized by BW, the numerator of the ratio will be similar in patients with similar bone metabolism. However, if patients have an extremely high or low weight, the denominator will be lower in patients with higher weight, increasing the SUV results, and higher in patients with lower weight, decreasing the SUV results. On the other hand, for SV SUVmean, the denominator will not change expressively with the variation in bone volume, and if it changes, this variation should also be reflected in the numerator value, since distribution of the radiopharmaceutical is the same in both. The results also demonstrated that the variability in BW SUVmean is similar to that in WN SUVmean, as corroborates the hypothesis that normalization by BW is not an adequate methodology in 18F-NaF PET/CT studies.
The use of routinely collected CT data from PET/CT studies to estimate body tissue composition, and the application of that information to normalize SUV, is not a new idea. Hamill et al. (24) proposed models to estimate lean mass from CT HUs and used that to normalize SUV in 18F-FDG PET/CT studies. They concluded that the methods based on CT were less variable than the BW method and were comparable to the lean body mass method calculated using an empiric formula. Kim et al. (25) compared SUV normalized by lean body mass as determined by CT in 18F-FDG PET/CT with SUV determined by predictive equations. They concluded that normalization of SUV by lean body mass as determined by CT, rather than normalization by predictive equations, may be a useful approach to reduce errors. However, as far as we know, our study is the first to use CT information from 18F-NaF PET/CT to estimate SV and to use this volume to normalize the SUV.
In a previous article (26), SV SUV technique was proposed instead of BW SUV. In that article, SUV in normal regions was analyzed in 2 groups of patients with extremes of weight. The results demonstrated that the maximum BW SUV was statistically significantly higher in the subgroup of heavier patients, whereas the maximum SV SUV did not significantly differ in either group of patients. This finding suggested the superiority of normalization by SV since there is no reason for the difference between SUV in heavy and light patients. However, that analysis was performed on a restricted group of 12 patients with extremes of weight and not on a larger group of patients with the whole spectrum of weight. Therefore, our study corroborates the finding of this previous study that SV normalization is superior to BW normalization in 18F-NaF PET/CT studies, but our study generalizes the results to a large group of patients with a wide range of weights.
Regarding the statistical analyses, we used a 1-tailed test because our initial hypothesis was that the variability in the results for whole-skeleton SV SUV was lower than that for BW SUV and not that SV SUV differed from BW SUV. Therefore, the use of a 1-tailed test should be more adequate in this situation. We also used a nonparametric test for the reason that variability was defined as the absolute difference between one value and the mean of all values (Eq. 3). Therefore, the variabilities are not normally distributed, and it is necessary to use a nonparametric test to perform the statistical analysis. Lastly, because we analyzed paired samples, we used the Wilcoxon signed-rank test, a nonparametric paired-samples test that is equivalent to the parametric paired-samples t test (27).
The reason we used whole-skeleton SUV instead of segmental bone SUV to analyze bone metabolism is that we believe the former, being less susceptible to regional aspects such as mechanical stress, is a more representative measure of the entire skeletal metabolism (28). In addition, the whole-skeleton SUV could be a useful parameter to follow up patients with benign or malignant diffuse bone disease. Therefore, knowing the best normalization method for this parameter could be useful to properly perform whole-skeleton metabolism analysis.
The reason we used 18F-NaF PET/CT studies showing normal results instead of pathologic results is that pathologic results would show much more variable uptake, ranging from faint focal uptake in a specific bone region to diffuse and intense skeletal uptake. Such biologic variability could mask the analysis of variability caused by differences in normalization methods.
CONCLUSION
In patients with normal 18F-NaF PET/CT results, SV SUVmean presents lower variability than BW SUVmean. Therefore, the use of SV normalization seems more precise than normalization by BW to semiquantitatively analyze 18F-NaF PET/CT studies.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 23, 2018.
REFERENCES
- Received for publication May 25, 2018.
- Accepted for publication August 6, 2018.





{kind=link}