


Abstract
The main objective of this study was to check the validity of using a γ-camera as an alternative to a thyroid uptake probe for measuring the γ-count from 0.925-MBq (25 μCi) and 1.85-MBq (50 μCi) 131I capsules before administration to patients. Methods: Ten sets each of 0.925- and 1.85-MBq 131I capsules received from the Board of Radiation and Isotope Technology, Department of Atomic Energy, India, were counted individually using a thyroid uptake probe for 10 s following institutional protocol, keeping an 8-cm gap between capsules. Each set was also scanned by a scintillation γ-camera for 100 s. The scans were analyzed by drawing identical regions of interest around each set of 0.925- and 1.85-MBq 131I capsules, and the correlation between the camera-based and probe-based methods was determined. By either method, capsules having counts within 2 SDs of the mean were considered acceptable for administration to patients. Results: The correlation between the two methods was good (r > 0.95). Conclusion: The camera-based method of counting 131I capsules is easy and saves time, compared with the probe-based method, as an entire set of capsules can be scanned in a single acquisition. The camera-based method can show whether a batch of 131I capsules is uniform and therefore eliminate the time-consuming counting of individual capsules with a thyroid uptake probe.
The use of nuclear medicine for the diagnosis and treatment of thyroid-related disorders is well known. Measurement of radioiodine uptake by the thyroid was one of the earliest clinically useful procedures in diagnostic nuclear medicine. Despite its success, several sources of inaccuracy and inconsistency have been recognized over the years (1). Construction of a thyroid neck phantom to simulate the absorption and scatter characteristics of the human neck was one of the first steps toward standardization of the thyroid uptake test. Differences in neck-phantom characteristics and high-voltage fluctuations obviously may introduce significant errors into any thyroid uptake measurement, but even today the test is performed in most laboratories with little attention to these factors (2).
Although 99mTcO4− can also be used for thyroid imaging, it is not organified by the thyroid gland. High background activity and low neck uptake make 131I a better agent, mainly for evaluations before 131I therapy (3). 123I is a better diagnostic agent, but 131I continues to be used in several developing countries where 123I is not readily available. It is normal practice to give a dose in the range of a few microcuries of 131I to assess benign thyroid disorders or to assess remnant thyroid tissue in order to determine the dose required to ablate it. A dose in the range of a few millicuries is normally given to evaluate for metastasis through whole-body scanning (4).
Quantitative evaluation of 131I uptake is important in distinguishing among various functional states of the thyroid, because qualitative information obtained by γ-camera alone may not be adequate in many clinical conditions (4). At our center, a 0.925-MBq (25 μCi) dose of 131I is administered for evaluation of conditions such as hyperthyroidism, hypothyroidism, and multinodular goiter, whereas a comparatively higher dose (i.e., 3.7 MBq [100 μCi]) is administered for evaluation of the postthyroidectomy status of remnant tissue in thyroid cancer patients, and a 111- to 185-MBq (3–5 mCi) dose is administered for follow-up whole-body and neck scanning after 131I treatment.
Before administering radioactive iodine, our center confirms that the patient has followed the iodine restriction requirements, is not taking any interfering drugs, and is not pregnant or lactating. After the 131I dose has been administered, neck counts are taken at 2 and 24 h using a thyroid uptake probe that has a NaI(Tl) crystal fitted with a flat-field collimator and the associated electronics (1,5). The patient is positioned supine with the neck extended, and the probe is placed 30 cm away. Two sets of neck counts are obtained for 100 s each, and the neck background count is then obtained by placing a lead shield over the thyroid area. The ratio of the background-corrected neck count to the background-corrected phantom count is calculated to get the percentage neck uptake, or [(neck count − neck background count)/(phantom count − phantom background count)] ×100 (6). An alternative, camera-based, method has also been found to be a good option (5).
At our center, 20 capsules of 0.925-MBq 131I and 40 capsules of 1.85-MBq (50 μCi) 131I are procured each week from the Board of Radiation and Isotope Technology, Department of Atomic Energy, India. We measure the γ-count from each of these capsules individually using a thyroid uptake probe. The aim of this study was to determine whether γ-camera imaging of sets of capsules can be substituted as an easier, quicker method of counting.
MATERIALS AND METHODS
This experiment used 10 sets of 0.925-MBq capsules (n = 15 per set) and 10 sets of 1.85-MBq capsules (n = 20 per set). The same capsules were used for both the probe-based and the camera-based methods. Institutional approval was obtained to conduct the experiment, which did not involve any patients or animals.
Probe-Based Counting Method
A thyroid uptake probe (Nuclear Chicago) fitted with a flat-field collimator, the associated electronics, and a single-channel analyzer was used to count individual capsules and determine thyroid uptake in referred patients. The probe was calibrated daily using an 131I source before routine use, and it was tested monthly for absolute sensitivity using 137Cs (7). Baseline energy was kept at 310 keV, with a 100-keV window. Sealed gelatin capsules containing 131I were kept individually in serially numbered test tubes. In the probe-based counting method, each capsule was placed in an acrylic glass thyroid phantom 30 cm from the face of the probe’s detector (iso-response region) and counted for 10 s (5). The background count was also measured for 10 s and then subtracted from the capsule count, and the mean and SD were calculated for the 0.925-MBq capsule sets and the 1.85-MBq capsule sets separately. Capsules with counts that fell within 2 SDs of the mean were considered identical and acceptable for administration to the patient. One of these capsules was chosen randomly for use as a standard for the patient’s neck uptake calculation for the entire week (Fig. 1).

Thyroid uptake probe (131I capsule in acrylic glass phantom).
Camera-Based Counting Method
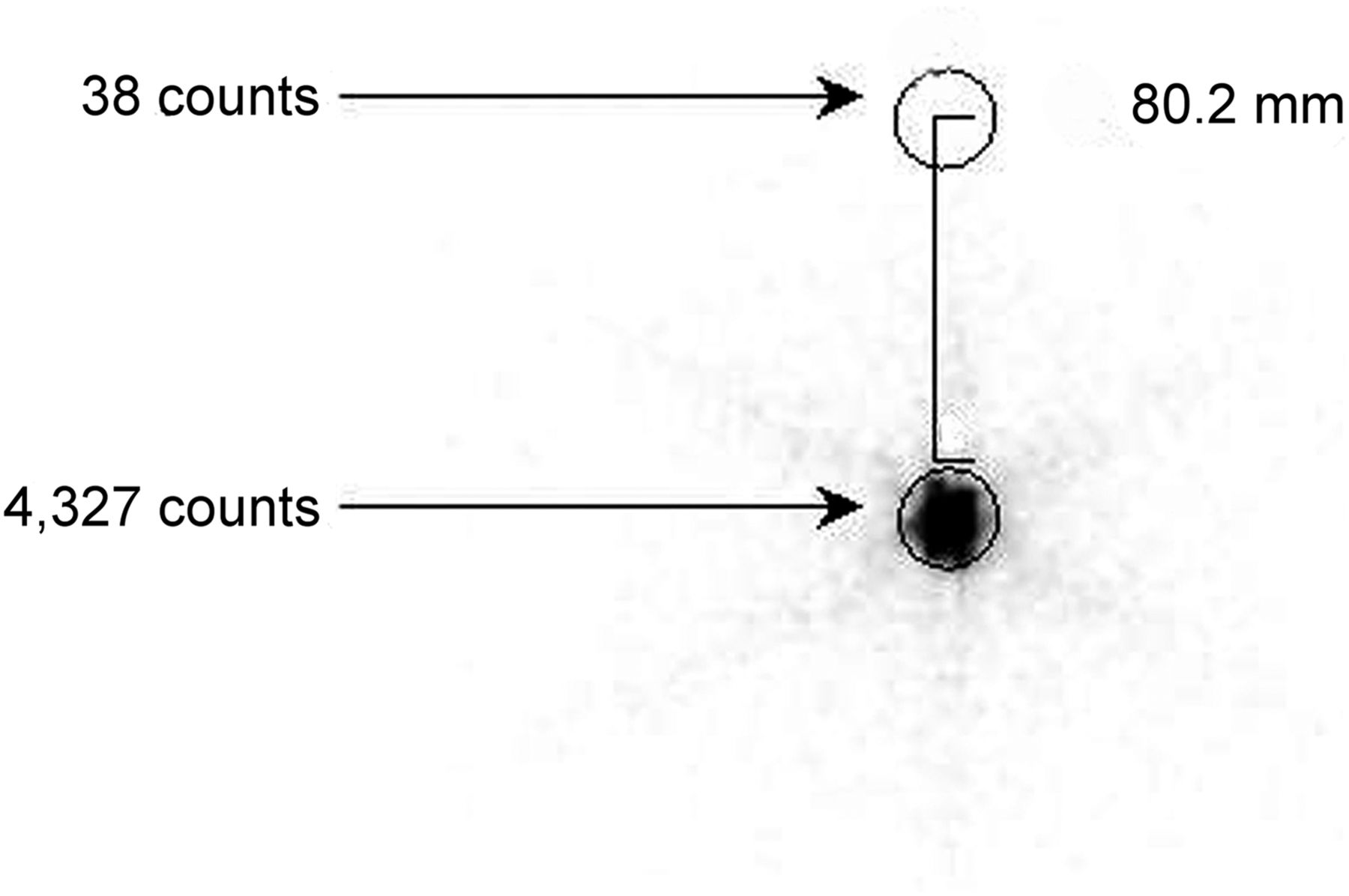
A Symbia γ-camera (Siemens) with a ⅝-inch-thick (1.5875 cm) NaI(Tl) crystal and a high-energy collimator was used for imaging. The optimum distance required between adjacent capsules was measured by calculating the percentage scatter contribution at various distances from a capsule centered in a polystyrene foam sheet. To calculate scatter contribution around a capsule, circular regions of interest were drawn at 2, 4, 6, and 8 cm away from the capsule position, and the scatter count for each region was determined. The ratio of each scatter count to the capsule count after background subtraction was then calculated (Tables 1 and 2). A distance of 8 cm was chosen as optimal because its scatter contribution was less than 1% (Fig. 2).
Scatter Count and Percentage Scatter Contribution at Different Distances in y Direction from Centered 0.925-MBq Capsule
Counts and Count Ratios for Capsules Surrounding Central Capsule
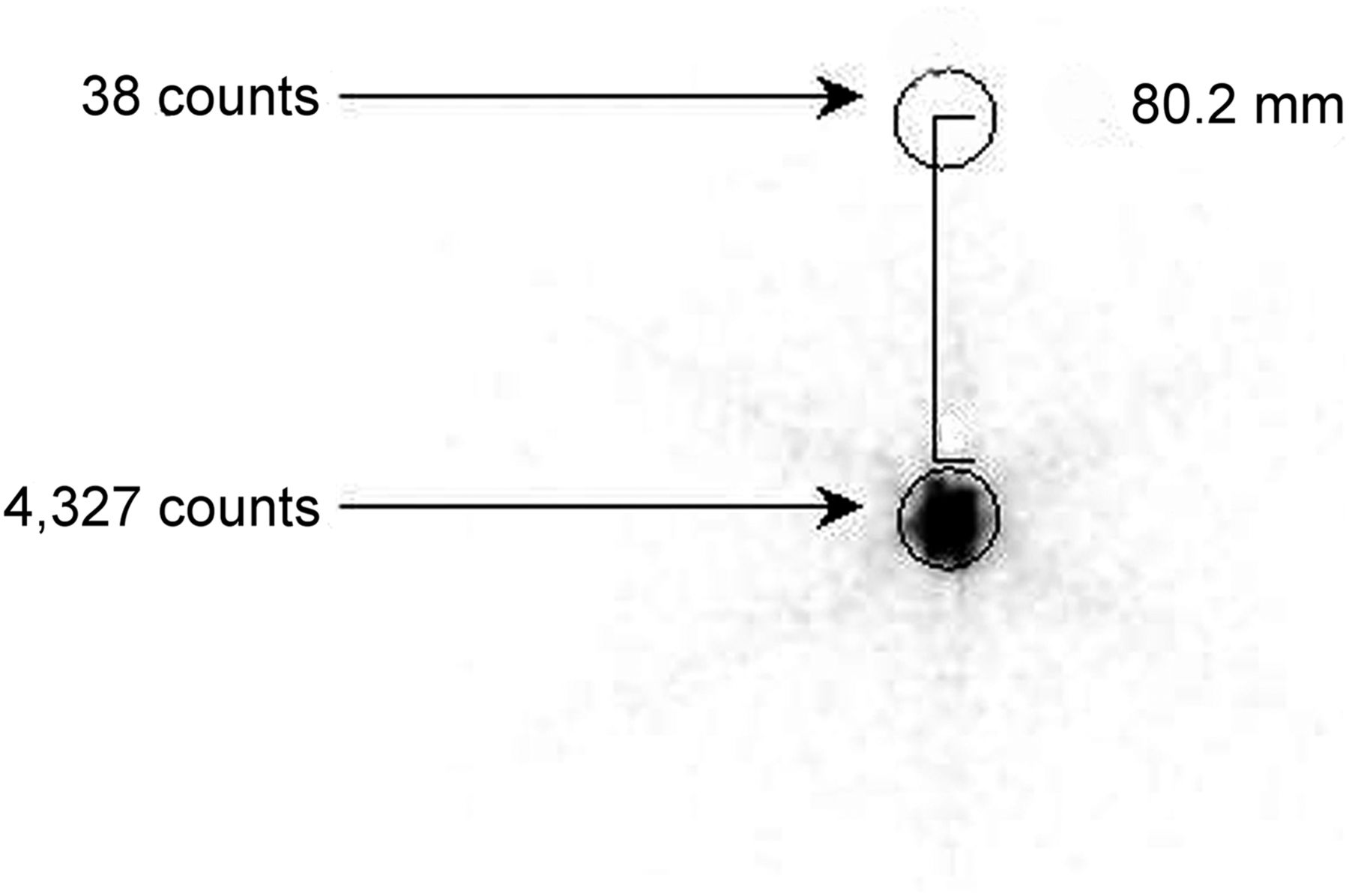
Scatter counts 8 cm away from 0.925-MBq 131I capsule.
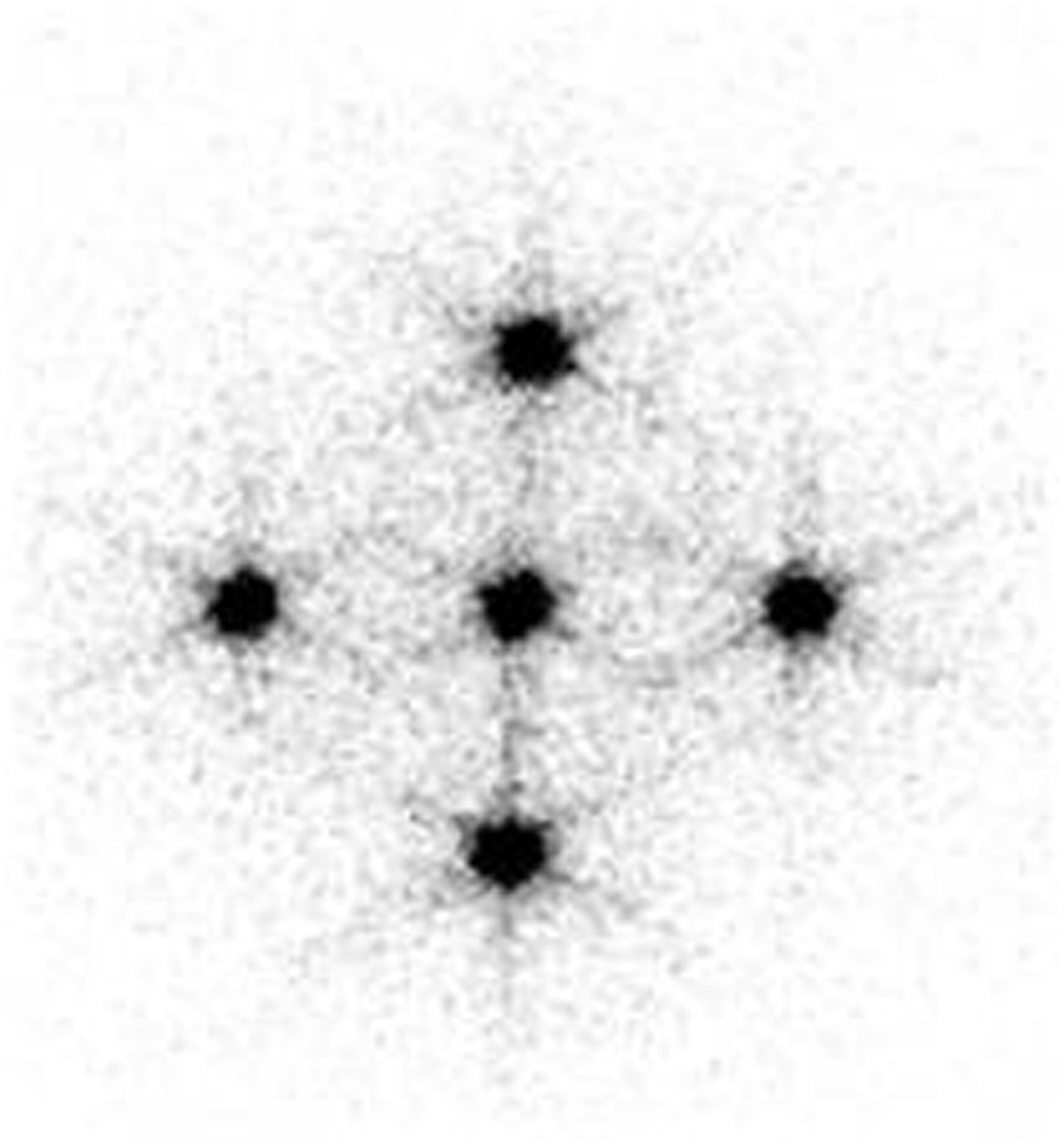
We confirmed this choice by surrounding the centered capsule with capsules 8 cm away from it, one in each direction along the x- and y-axes (Fig. 3). A region of interest was drawn around the central capsule, and the count was measured after the addition of each of the 4 surrounding capsules, as shown in Table 2. The presence of the surrounding capsules did not make a significant scatter contribution (<1%) to the central capsule and vice versa.

Counts for capsules arranged around center capsule.
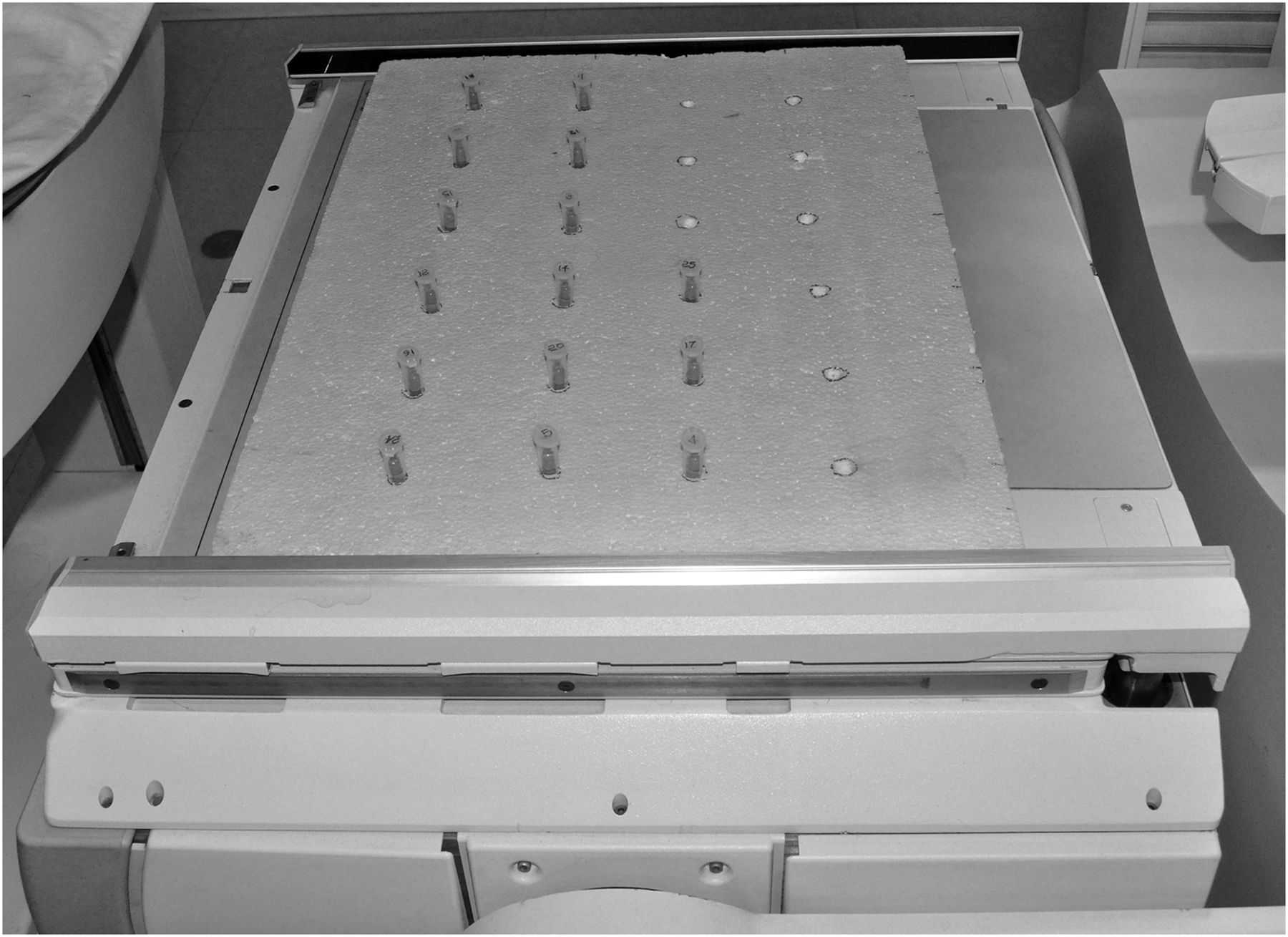
Accordingly, grooves 8 cm apart were made in a polystyrene foam sheet, each set of capsules in their individual test tubes was arranged in these grooves, and the foam sheet was placed directly on the head of the γ-camera. Data for each set of capsules were acquired for 100, 200, and 300 s using a 256 × 256 matrix, a zoom of 1, and an energy window peaked at 364 keV with a 15% window (Figs. 4 and 5). Identical circular regions of interest were drawn around each capsule in the single image. The count in each region of interest was measured, and the mean count and SD were calculated. Capsules having counts falling within 2 SDs of the mean were considered as within acceptable limits and were used for administration to patients and as a standard for uptake calculation (Tables 3 and 4; Fig. 4). For both the 0.925-MBq and the 1.85-MBq capsules, the 100-s count obtained with the camera-based method was comparable to the 10-s count obtained with the probe-based method. The 100-s scanning time was considered optimal for data acquisition, as increasing the time to 200 or 300 s did not improve the result.
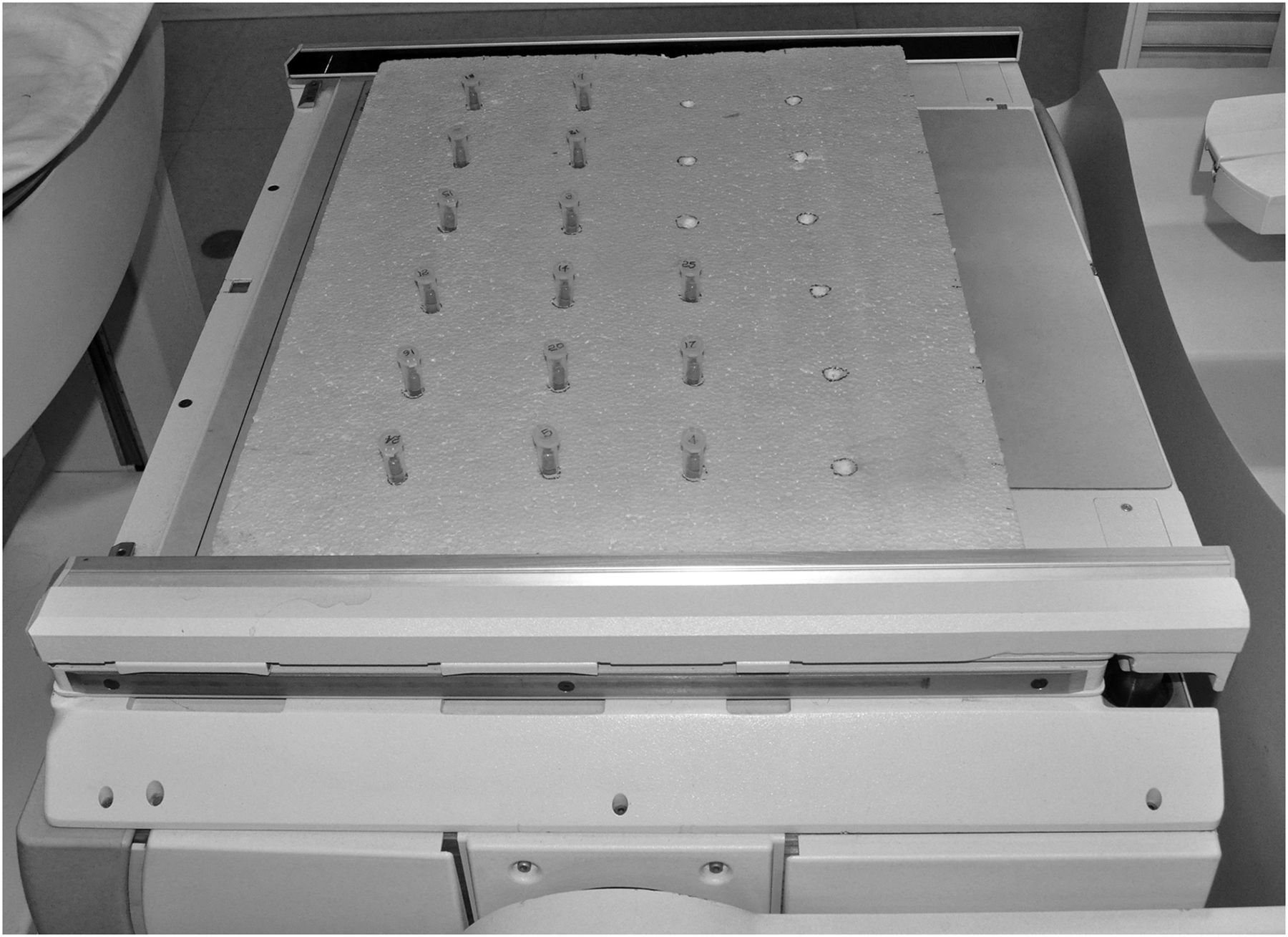
Capsule arrangement in camera-based 131I capsule counter.

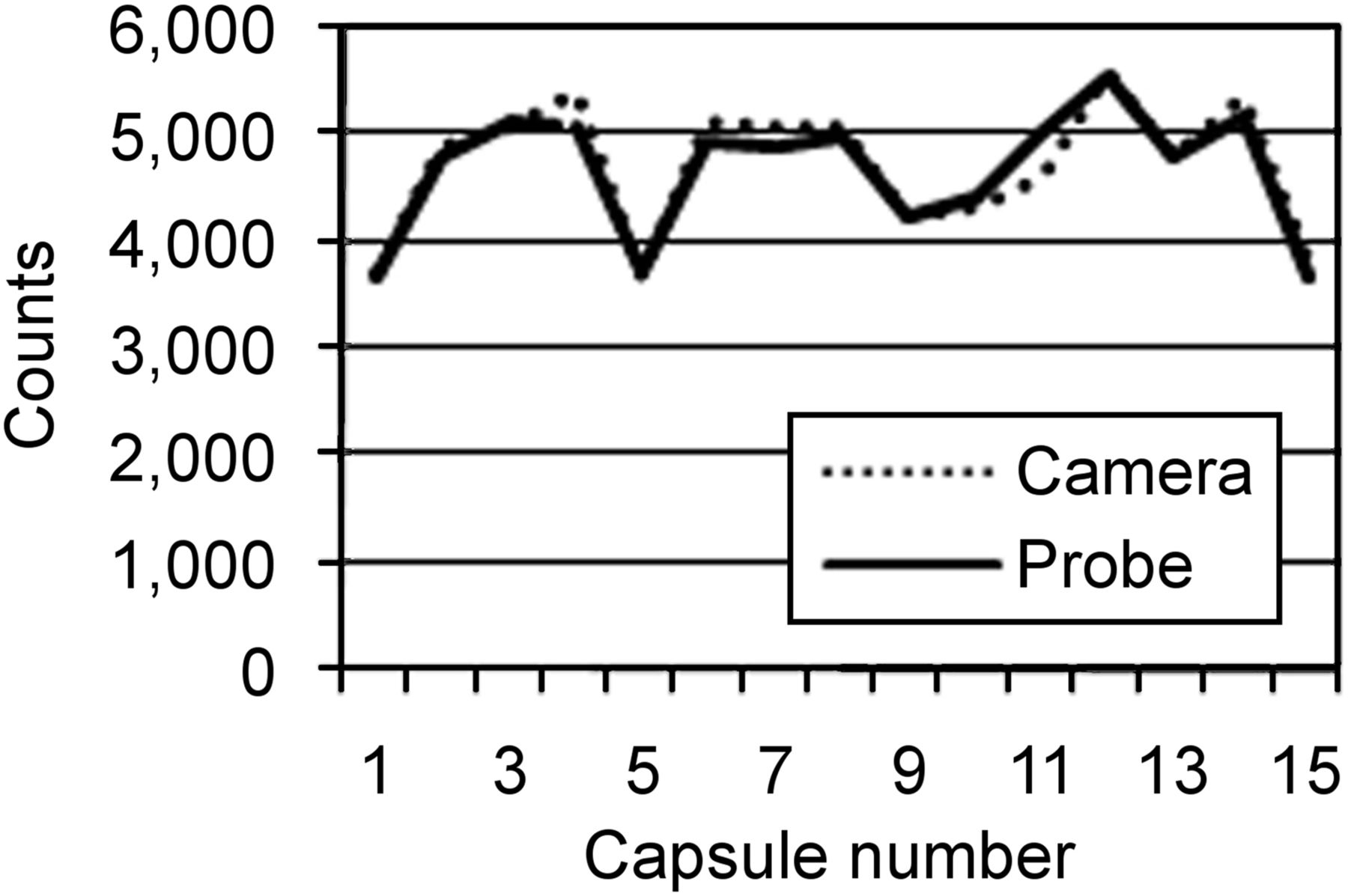
Counts vs. capsule number, by camera-based and probe-based methods.
Camera-Based Counts at Various Acquisition Times vs. Probe-Based Counts for 0.925-MBq Capsules
Camera-Based Counts at Various Acquisition Times vs. Probe-Based Counts for 1.85-MBq Capsules
RESULTS
Both methods found that all 20 of the 1.85-MBq capsules in each of the 10 sets were within 2 SDs of the mean.
Data obtained from all 10 sets of 0.925-MBq capsules (also all within 2 SDs of the mean) and all 10 sets of 1.85-MBq capsules were compared between the probe- and camera-based methods, and a good correlation was found (r > 0.95).
Counts obtained from the 100-s images using the camera-based method correlated well with the thyroid-probe 10-s counts, which may vary for different instruments.
DISCUSSION
The camera-based method of counting is as accurate as the probe-based method and has several advantages over it. Because the probe-based method counts each capsule individually, each needs to be kept under identical conditions; this limitation does not exist in the camera-based method, which scans many capsules in single acquisition. Another advantage is an increase in patient throughput, as the counting of a large set of capsules takes less time than the counting of each individual capsule. In addition, information on the uniformity of an entire batch of 131I capsules can be obtained at once, avoiding the time-consuming counting of individual capsules using a thyroid uptake probe. As an alternative to the probe-based method, the camera-based method will be a better option when standard capsules are being counted.
CONCLUSION
The camera-based method of measuring the γ-count from 131I capsules is easy, takes less time than the probe-based method, and is just as accurate.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 10, 2017.
REFERENCES
- Received for publication July 10, 2017.
- Accepted for publication October 17, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.