


Abstract
Glomerular filtration rate (GFR) measurements are critical in patients with hepatic cirrhosis but potentially erroneous when based on serum creatinine. New equations for estimated GFR (eGFR) have shown variable performance in cirrhotics, possibly because of inaccuracies in reference methods for measured GFR (mGFR). The primary objective was to compare the performance of 4 improved eGFR equations with a 1-compartment, 2-sample plasma slope intercept 99mTc-DTPA mGFR method to determine whether any of the eGFR calculations could replace plasma 99mTc-DTPA mGFR in patients with cirrhosis. The secondary objective was to test the hypothesis that mGFR using voluntary voided urine collections introduces error compared with plasma-only methods. Methods: Fifty-four patients with hepatic cirrhosis underwent mGFR determinations from 2 plasma samples at 1 and 3 h after intravenous administration of 185 MBq of 99mTc-DTPA. GFR was also generated by a UV/P calculation derived from blood and urine samples. These mGFRs were compared with the eGFRs generated by 4 estimating equations: MDRD (Modified Diet in Renal Disease), CKD-EPI (Chronic Kidney Disease-Epidemiology Collaboration) (serum creatinine [SCr]), CKD-EPI (cystatin [CysC]), and CKD-EPI (CysC+SCr). eGFRs were compared with mGFRs by Pearson correlation, precision, bias, percentage bias, and accuracy (eGFRs varying by <10% [p10], <20% [p20] or <30% [p30] from the corresponding mGFR). Results: All eGFRs showed poorer performance when the UV/P 99mTc-DTPA mGFR was used as the reference than when the plasma 99mTc-DTPA mGFR was used. When compared with the plasma 99mTc-DTPA mGFR method, the performance of all eGFR equations was superior to most published reports. There was a moderately good positive correlation between eGFRs and mGFRs. When compared with plasma 99mTc-DTPA mGFR, precision of eGFRs was in the range of 14–20 mL/min and showed a negligible bias. Compared with the plasma 99mTc-DTPA mGFR, CKD-EPI (CysC+SCr) showed the best overall performance and accuracy, at 85.19% (p30), 75.93% (p20), and 42.59% (p10). Conclusion: Estimating equations for measuring eGFR performed better than in most published reports, attributable to use of the plasma 99mTc-DTPA mGFR method as a reference. CKD-EPI (CysC+SCr) eGFR showed the best overall performance. However, more discriminating methods may be required when accurate GFR measurements are necessary. mGFR measurements using urine collections may introduce error compared with plasma-only methods.
Glomerular filtration rate (GFR) is an important parameter of renal function in patients with acute and chronic kidney disease. Patients with hepatic cirrhosis are susceptible to reversible as well as chronic kidney dysfunction because of altered hemodynamics, volume shifts, and comorbidities (1–3). Accurate measurements of GFR are critical in these patients and affect both management and outcome. Many drugs with kidney clearance and liver metabolism or clearance require adjustments in the face of renal and hepatic insufficiency. Renal insufficiency portends a poor prognosis in cirrhosis (4,5). Renal function, typically measured by serum creatinine (SCr), also plays an important component in the Model for End-Stage Liver Disease score, which is used in prioritizing patients being considered for liver transplantation.
The most common clinical estimates of GFR are based on SCr, often by the Cockcroft–Gault formula (6), and on 24-h urinary creatinine clearance. It is widely recognized that the use of these creatinine-based estimates may significantly overestimate GFR in patients with hepatic cirrhosis. This is due to decreased hepatic production of creatinine, decreased muscle mass, and malnutrition. These factors often coexist in patients with cirrhosis. Serum cystatin C (CysC) has been proposed as a novel biomarker of renal function. It is found in nearly all tissues and body fluids; it undergoes clearance by glomerular filtration; and its levels are unaffected by race, age, muscle mass, or liver disease (7). In recent years, improved equations have been developed for estimating GFR. These include MDRD (from the Modified Diet in Renal Disease Study) and 3 formulas developed by the Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) that use both SCr and CysC. These include CKD-EPI (SCr), CKD-EPI (CysC), and CKD-EPI (CysC+SCr) (8,9). These improved equations for determining estimated GFR (eGFR) have gained popularity and acceptance in the general population (10). In a limited number of studies in patients with cirrhosis, the CysC equations tend to show better results than methods based solely on SCr. However, the published performance of the equations is variable, creating uncertainty as to whether these equations may obviate the need for more accurate methods for measuring GFR in cirrhotics (11–15).
The most accurate test for determining GFR in the United States has traditionally been plasma or urinary clearance of inulin. This method represents a significant technical challenge to routine clinical use. 99mTc-diethylenetriaminepentaacetic acid (DTPA) is a renal imaging agent that is excreted entirely by glomerular filtration and has been used clinically to measure GFR both by camera-based and by plasma clearance methods. Camera-based methods are hampered by attenuation factors, leading to a general preference for plasma clearance methods. Methods for measuring GFR have been developed using a single intravenous injection of 99mTc-DTPA, followed either by single or by multiple plasma samples (16,17). The single-injection, 1-compartment, 2-sample slope-intercept clearance method is widely used. A correction factor, such as that described by Bröchner-Mortensen, is often applied to recover the early compartment area under the curve (16,18,19). The plasma 99mTc-DTPA clearance method requires 2 venous access lines, several hours to complete, and careful attention to laboratory technique. Nonetheless, it is easier to implement than inulin clearance. In many centers throughout the United States and Europe, plasma 99mTc-DTPA clearance has become a commonly used method for GFR determinations when accurate measurements are required.
Several publications have addressed the value of improved prediction equations for estimating GFR in patients with hepatic cirrhosis (11–15,20). However, these reports have compared the performance of the eGFR equations with very disparate reference methods for measured GFR (mGFR). None of these studies used the 1-compartment, 2-sample 99mTc-DTPA plasma clearance method as a reference. The performance of the estimating equations was quite variable in many of these studies and, in most cases, less than optimal. Technical problems with the reference mGFR methods could compromise assessments of the value of the improved estimating equations for eGFR. This is particularly true when single-injection GFR determinations involve timed, voluntary urine collections (21). The purpose of this study was to compare the performance of the MDRD, CKD-EPI (SCr), CKD-EPI (CysC), and CKD-EPI (CysC+SCr) estimating equations with that of the 2-sample plasma 99mTc-DTPA clearance method for mGFR to determine whether any of the eGFR equations perform sufficiently well as to replace plasma 99mTc-DTPA methods in patients with hepatic cirrhosis. A secondary objective was to test the hypothesis that performance of the eGFR equations will be less favorable when compared with mGFR derived from a conventional methodology that incorporates voluntary timed voiding urine collections.
MATERIALS AND METHODS
Subjects
Fifty-four adult patients with hepatic cirrhosis were enrolled under a research protocol approved by the Investigational Review Board of the University of Utah, Salt Lake City, Utah, and were able to complete all portions of the study. Of these, 17 were women and 37 were men, all Caucasian. The mean age was 57 y (range, 37–72 y).
Measured (Reference) GFR Methods
The reference, or mGFR, was determined by 2 separate methods after a single injection of 185 MBq (5.0 mCi) of 99mTc-DTPA. The plasma 99mTc-DTPA method used 2 plasma samples obtained at 1 and 3 h after the intravenous administration of 99mTc-DTPA (16,17). Each sample was ultrafiltered to remove plasma proteins by a described method (21). The single-injection, 2-sample plasma 99mTc-DTPA mGFR is a monoexponential slope-intercept method that neglects the early (fast) exponential phase of what is, in reality, a biexponential clearance curve (16,18). To correct for this, the final GFR was corrected by the Bröchner–Mortensen quadratic formula, which is applicable to both adults and children (16,18,20). For this method, the Haycock method was used for estimating body surface area (BSA) from height and weight (22). However, the final plasma 99mTc-DTPA mGFR was reported as gross GFR (mL/min, not BSA corrected).
As described by Vivier et al., mGFR was also measured by a method that used both urine and plasma samples (UV/P method) (23). After injection of 99mTc-DTPA (the same dose as above) and observance of a 1-h equilibrium period, two 90-min voluntary voided urine collections were obtained at 150 and 240 min after injection. Blood samples were collected 60, 150, and 240 min after the injection. Urinary clearance was computed as follows: mGFR = UV/P, where U is the cpm/mL of urine sample, V is the urine flow rate in mL/min, and P is the log average of cpm in serum samples bracketing each urine collection. UV/P mGFR was expressed as gross GFR (mL/min, not BSA corrected).
eGFR Equations
mGFR generated by both DTPA methods was compared with the eGFR values generated by 4 different prediction formulas recommended by the National Kidney Foundation that use SCr or CysC (8,9). These include MDRD (from the Modified Diet in Renal Disease Study), which was calculated using 6 variables (SCr, age, race, sex, albumin, and urea nitrogen) and 3 formulas developed by the CKD-EPI including CKD-EPI (SCr), CKD-EPI (CysC), and CKD-EPI (CysC+SCr). Blood tests for the eGFR prediction formulas were obtained on the same day as the mGFR procedures were performed. The eGFR values were expressed as gross GFR (mL/min, not BSA corrected).
Statistical Analysis
The parameters for assessment of the performance of an eGFR test in comparison to mGFR were based on Kidney Disease: Improving Global Outcomes (KDIGO) and National Kidney Foundation Kidney Disease Outcome Quality Initiative (K/DOQI) practice guidelines (10,24). Pearson correlation was used to generate the correlation coefficient (r statistic) between mGFR and eGFR values. Precision of eGFR tests was defined as the root mean square error between the eGFR and mGFR values as determined by linear regression. Bias (mean mGFR-eGFR) and percentage bias (mean of absolute value of [mGFR-eGFR]/[mGFR]) were determined by the Altman Bland agreement test. Accuracy was measured as the percentage of eGFRs varying by <10% (p10), <20% (p20), or <30% (p30) from the corresponding mGFR value.
RESULTS
The descriptive statistics (mean, SD, range) for the GFR values derived from the 2 mGFR measurements (plasma and UV/P 99mTc-DTPA methods) as well as from the eGFRs derived from the 4 estimating equations are shown in Table 1. Results for performance of the estimating equations in comparison to the 2 mGFR methods are summarized in Table 2. Plots of mGFR versus eGFR values are shown in Figures 1 and 2.
Descriptive Statistics for 2 99mTc-DTPA Methods for mGFR and 4 Equations for eGFR in 54 Patients with Hepatic Cirrhosis
Comparison of Performance of Equations for eGFR to 2 99mTc-DTPA Reference Methods for mGFR in Patients with Hepatic Cirrhosis

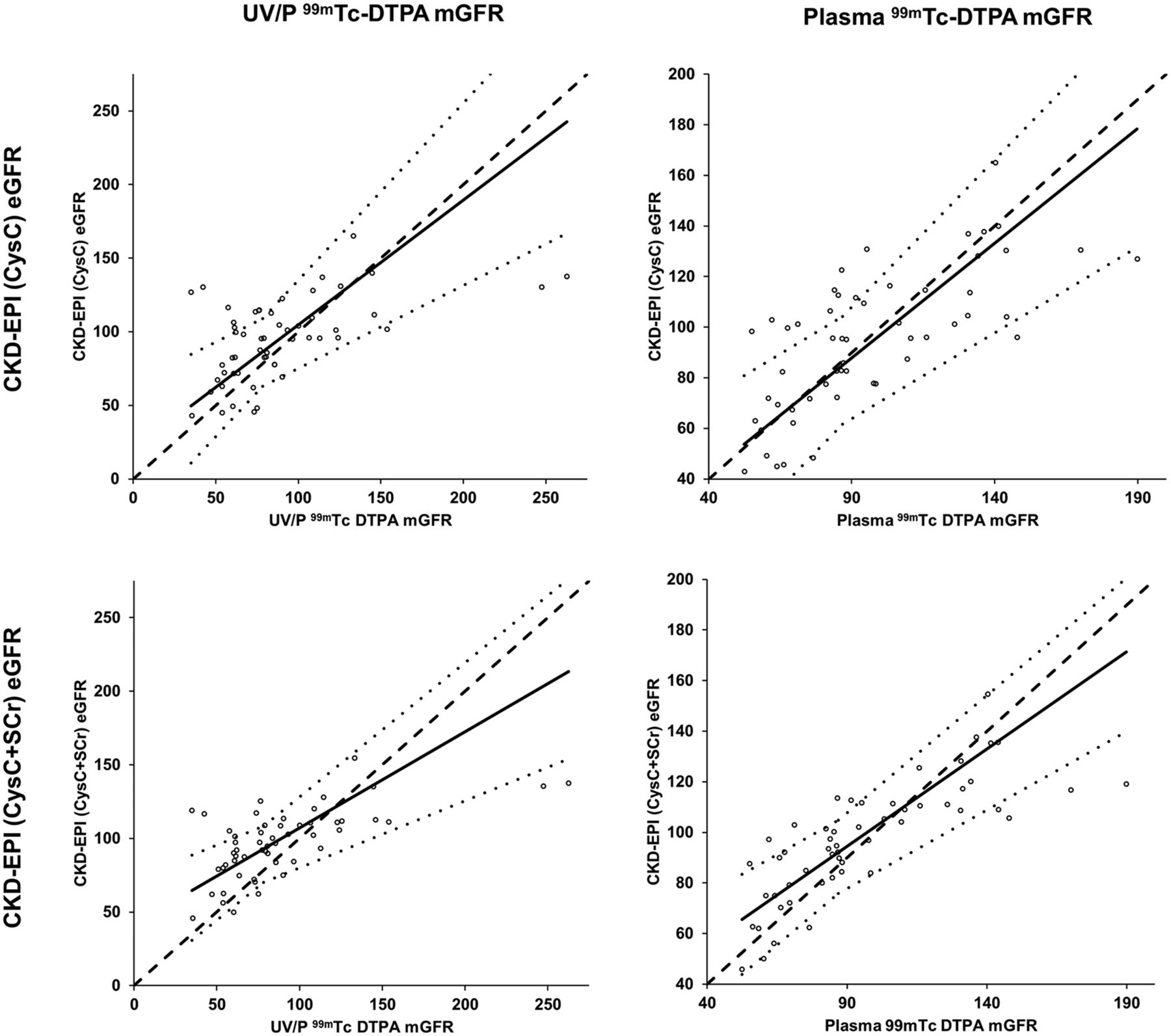
Scatterplots of mGFR vs. eGFR values for MDRD and CKD-EPI (SCr), CKD-EPI (CysC), and CKD-EPI (CysC+SCr). Graphs in left-hand column use UV/P 99mTc-DTPA method for mGFR as reference. Corresponding graphs in right-hand column use plasma 99mTc-DTPA method. Line of identity (dashed line), linear line fit (solid line), and 95% confidence intervals (thin dotted lines) are shown for each set of comparisons.
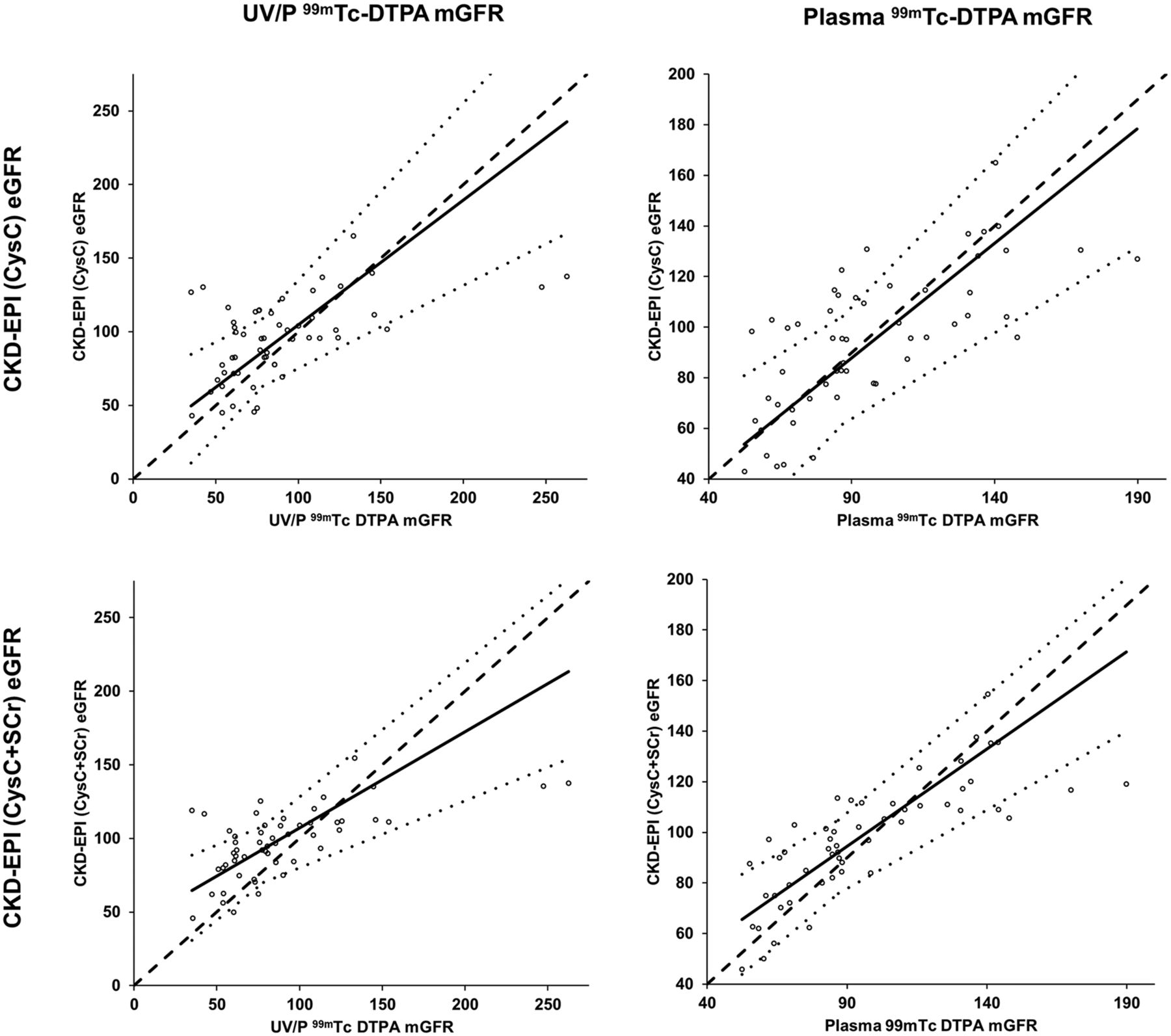
Scatterplots of mGFR vs. eGFR values for CKD-EPI (CysC) and CKD-EPI (CysC+SCr). Graphs in left-hand column use UV/P 99mTc-DTPA method for mGFR as reference. Corresponding graphs in right-hand column use plasma 99mTc-DTPA method. Line of identity (dashed line), linear line fit (solid line), and 95% confidence intervals (thin dotted lines) are shown for each set of comparisons.
Comparison of Plasma 99mTc-DTPA mGFR with eGFRs
The mGFR and each of the eGFR measurements was first confirmed to assume a roughly normal distribution, based on a frequency plot with a normal histogram overlay. There was a moderately strong positive correlation between each of the eGFR and the plasma 99mTc-DTPA mGFR values, but strongest for CKD-EPI (CysC+SCr), at +0.79 (95% confidence interval, 0.66–0.87). When compared with the 99mTc-DTPA mGFR, the precision of eGFR-estimating formulas ranged from 14.18 mL/min (CKD-EPI [CysC+SCr]) to 19.59 mL/min (CKD-EPI [CysC]). Precision was most favorable for CKD-EPI (CysC+SCr). The bias was negligible (< −2.69 to 1.54 mL/min) for the eGFR values when compared with 9mTc-DTPA mGFR. The percentage bias was least for MDRD (2.53%). Accuracy was measured at 3 levels, as the percentage of eGFR values that differ by <30% (p30), <20% (p20), or <10% (p10) of the corresponding mGFR values. The CKD-EPI (CysC+SCr) showed the best overall accuracy, at 85.19% (p30), 75.93% (p20), and 42.59% (p10), respectively. MDRD eGFR showed slightly higher accuracy than CKD-EPI (CysC+SCr), at p30 (88.89%), but slightly lower accuracy at p20 (68.52%) and p10 (35.19%). Accuracy was lower for both CKD-EPI (SCr), at 83.33% (p30), and CKD-EPI (CysC), at 77.78% (p30).
Comparison of UV/P 99mTc-DTPA mGFR with eGFR
For each of the estimating equations, performance was less favorable when the UV/P 99mTc-DTPA mGFR was used as the reference method than when the plasma 99mTc-DTPA mGFR was used (Table 1). When compared with the UV/P 99mTc-DTPA mGFR method, precision of the eGFR measurements ranged from 16.45 to 25.55 mL/min. The eGFR equations gave higher GFR values than the UV/P 9mTc-DTPA, with a bias ranging from −6.23 (MDRD) to −10.46 (CKD-EPI [SCr]). Accuracy was also considerably poorer when the UV/P 99mTc-DTPA mGFR method was used as a reference than when the plasma 99mTc-DTPA mGFR was used. For the least discriminating measurement (p30), eGFR accuracies ranged from 55.56% (for CKD-EPI [SCr]) to 61.11% (for CKD-EPI [CysC+SCr]) when compared with the UV/P as a reference method.
DISCUSSION
Patients with hepatic cirrhosis present a particular challenge in accurately measuring GFR. Renal function is often impaired in this population because of a combination of factors, including hypovolemia caused by hypoalbuminemia and large-volume ascites, renal ischemia caused by bleeding varices, drug toxicity, and hepatorenal syndrome (1–3). In this population, factors other than renal function can falsely lower the SCr. These factors include impaired production of creatinine by the liver, reduced muscle mass, and malnutrition. This results in an overestimation of glomerular filtration with methods that use creatinine alone. Accurate measurements of renal function are particularly critical in patients with hepatic cirrhosis. First, renal functional has substantial prognostic significance in these patients (4,5), with a 7-fold increase in mortality in cirrhotic patients who have reduced renal function (25). Pharmacokinetics can be altered both by hepatic and by renal disease. Adjustments in dosing of medications require an accurate knowledge of the magnitude of renal dysfunction. The Model of End Stage Liver Disease score is an important determinant in prioritizing patients for liver transplantation but has been criticized in that it uses SCr. Improved and more accurate methods to measure GFR in patients with hepatic cirrhosis would greatly facilitate their medical management and may provide a more informed methodology for the allocation of liver transplants.
It is recognized that improved estimating equations for GFR offer significant theoretic advantages over SCr or urinary creatinine clearance estimators (10). These include MDRD and CKD-EPI equations that use both SCr and CysC. However, whether the performance of these improved estimating formulas is sufficiently accurate in patients with cirrhosis as to obviate the necessity for more accurate but laborious methods for measuring GFR remains debatable. In accurately evaluating the performance of the estimating equations, it is critical that the reference method used for mGFR be scrupulously accurate. Single-injection GFR methods that use voluntary timed voided urine collections are potentially fraught with inaccuracy unless exceptional steps are taken to ensure complete emptying of the bladder. Patients at risk for, or with a history of, urinary retention may require bladder catheterization. Ultrasound conducted after each episode of voiding can ensure complete emptying of the bladder. However, these maneuvers are rarely used, and technical details regarding assurances of bladder emptying are seldom discussed in the published reports using reference GFR methods.
In the current report, we tested and confirmed the hypothesis that inaccuracies are introduced by the addition of voluntary timed voiding urine collection (without ultrasound or bladder catheterization) as a component of a single-injection 99mTc-DTPA mGFR method. The performance of the eGFR equations was considerably poorer when the UV/P 99mTc-DTPA method was used as a reference for mGFR than when the plasma 99mTc-DTPA method was used. Because the eGFR measurements were the same and plasma samples similar for both sets of comparisons, the source of error was likely the urine collections. We therefore conclude that if scrupulous urine collection methods cannot be used, then plasma-only methods for measuring GFR should be used, such as the 1-compartment, 2-sample plasma 99mTc-DTPA method. If long continuous infusion techniques are used with extended intervals of urine or plasma collection, plasma clearance methods should equal urinary clearance. However, this would require a substantially greater investment of time and effort in performing these studies than the methods performed herein.
At the time of preparation of the current report, we are aware of several other publications evaluating the performance of improved equations for eGFR in patients with hepatic cirrhosis. In each of these reports, different reference methods were used to establish mGFR. One small study of 14 subjects used inulin clearance, presumably with urine and plasma collections, but did not include comparisons with the MDRD formula nor was there a discussion of methods used to ensure complete urine collection (13). Another report used Sinistrin clearance for mGFR (14). A report by Mindikoglu et al. used iohexol (nonradioactive iothalamate iodinated contrast medium), which requires high-performance liquid chromatography (15). Another study (12) used a camera-based 99mTc-DTPA method for measuring GFR. Although the camera-based method can be useful in following patients over time, we and others have shown that this method correlates poorly with more traditional reference methods for measuring GFR (12). An additional study used urinary excretion of 99mTc-DTPA but did not include details regarding methods to ensure complete urine collections (11).
There are similarities and differences between the results of the current study and those of the other publications that evaluate the performance of the MDRD and EKD-EPI estimating equations in measuring GFR in patients with hepatic cirrhosis. In all of the reports, including ours, the CKD-EPI (CysC+SCr) equation, which incorporates both SCr and CysC, outperformed the other estimating equations based on SCr or CysC alone. All the referenced publications, including the current, show a moderately good positive correlation between the mGFR and each of the eGFR estimating equations. However, this value can be misleading if it considered in isolation, as it does not provide an assessment of the precision, bias, or accuracy of the tests.
A parameter that is commonly used in the literature to describe accuracy of the estimating GFR equations is the percentage of patients in whom the eGFR varies by less than 30% from the mGFR (p30). This cutoff value has been criticized as insufficiently rigorous. More discriminating targets of accuracy (p20, p10) are more clinically justifiable but less frequently reported. In the current study, using the plasma 99mTc-DTPA method for mGFR, the estimating equations show better performance in terms of accuracy than most of the published reports, with a p30 of 88.89% for MDRD and 85.19% for CKD-EPI (CysC+SCr). The p30 for CKD-EPI (CysC+SCr) was reported as 60.4% for the Torre report (11), 64.3% for the Adlachi report (13), and 76.39% for the Mindikoglu report (15). These values are to the performance of the eGFRs in comparison to the UV/P plasma 99mTc-DTPA mGFR in the current report (p30, 55.56% to 61.11%). This further calls into question the rigor of the reference methods for mGFR in these prior reports. There were no major differences identified in the overall renal function between the subjects examined in these reports from the current study. In 1 published report, the Krones article (11), accuracy of CKD-EPI (CysC+SCr) resulted in a p30 of 84% and a p10 of 49%, which are similar to our results with plasma 99mTc-DTPA mGFR. The Krones study used a very conscientious methodology for establishing mGFR, Sinistrin (Inutest) clearance. This is laborious, with 12 serially drawn blood samples obtained over an interval of 4.5 h following injection. Sinestrin is not Food and Drug Administration approved for use in the United States. The plasma 99mTc-DTPA method used in the current report is simpler, involving 2 blood samples, and gives results similar to a reference for eGFR performance.
Absolute bias, percentage bias, and precision are less consistently reported in the literature in evaluating the performance of estimating equations for measuring GFR in patients with hepatic cirrhosis. As was true for measurements regarding accuracy, bias and precision were better in the current study, as well as in the literature when reported, for CKD-EPI (CysC+SCr) than for the other estimating equations. Precision for CKD-EPI (CysC+SCr) for the current study was 14.18 mL/min when compared with plasma 99mTc-DTPA mGFR. This was slightly better than values reported in other articles, which ranged from 17.9 to 23.49 mL/min (11,13,15). Measurements of bias of eGFR values vary somewhat in the literature, but are generally fairly small, both as a raw value and as a percentage of the mGFR. For the current study, bias of eGFR values, when compared with plasma 99mTc-DTPA mGFR, ranged from approximately −2.69 to 1.54 mL/min and were lower for CKD-EPI (CysC+SCr) than for the other estimating equations. Inaccurate eGFR values that are similarly distributed both above and below the mGFR could result in a small mean bias. Therefore, bias should be carefully considered in conjunction with the other measures of test performance.
There are several potential limitations of the current study that should be acknowledged. Although the bias was low for the plasma 99mTc-DTPA mGFR method, when compared with the estimating equation eGFR methods, there is the theoretic potential that the plasma method could overestimate GFR in patients with hepatic cirrhosis. The volume of distribution and elimination of radiometal-DTPA varies as a function of extracellular fluid volume (26). In the case of cirrhosis, a third space/compartment is created by ascites as well as edema due to decreased serum albumin/protein. 99mTc-DTPA could diffuse into this fluid space, artifactually appearing as enhanced renal clearance from the blood. This could result in an overestimation of GFR by plasma 99mTc-DTPA clearance methods in patients with cirrhosis. In this study, few patients had more than trace ascites and a distinction was not made between the patients with and those without ascites. Nonetheless, in patients with significant ascites, consideration for measurement of GFR by a more rigorous method that uses a constant infusion and both plasma and urine sampling should be considered.
In the past, 99mTc-DTPA showed variable degrees of protein binding. We have traditionally performed plasma 99mTc-DTPA clearance methods using ultrafiltered plasma samples to eliminate protein binding as a variable in GFR measurements (21). However, current 99mTc-DTPA formulations are quite stable and there is no current evidence that filtration of plasma samples is required any longer.
In the study design of the current report, the timing of the plasma samples for the single-injection, 1-compartment, 2-sample 99mTc-DTPA plasma clearance method for measuring GFR was at 60 and 180 min after injection, which is consistent with our previously reported methodology (21). However, more recent recommendations support that longer intervals from injection to plasma sampling, for example, at either 90 or 120 min and again at 240 min, may be preferable (16,27). It is possible that sampling of plasma at later intervals could further improve performance of the 99mTc-DTPA plasma clearance mGFR and of comparisons with the eGFR derived from estimating equations.
GFR values are often indexed (normalized) to a standard BSA, typically 1.73 m2, allowing a comparison to be made between the GFR of different patients. It has long been recognized that there is not a constant relationship between BSA, weight, and height (28). There is considerable controversy regarding the necessity or preferable methodology for indexing GFR by BSA (29). Scaling GFR to BSA may be fraught with inaccuracy in children and obese and very thin patients. This is especially true when using BSA calculations based on height and weight. In the current report, mGFR and eGFR values are reported as mL/min (not BSA corrected). However, this could slightly affect direct comparisons eGFR performance between the current and previous published reports.
CONCLUSION
In this report, the CKD-EPI (CysC+SCr) showed the best overall performance of the various estimating equations for GFR. The performance of all of the equations was generally better in the current report than in most of the published comparisons. The published reports have used inconsistent reference methods for mGFR determination. Inaccuracies inherent in many of the reference methods, particularly those that use camera-based or urinary excretion, may have contributed to the less favorable performance of the estimating equations in many of the other reports. The single-injection, 1-compartment, 2-sample ultrafiltered plasma 99mTc-DTPA clearance, which is widely used as an accurate method for measuring GFR in the United States and Europe, avoids many of the sources of inaccuracy. Despite these improved results, and using the best performing eGFR formula (CKD-EPI [CysC+SCr]), 14% of subjects in the current study demonstrated an eGFR of 30% or more of the mGFR, 24% demonstrated an eGFR of 20% or more of the mGFR, and approximately 57% had an eGFR of 10% or more of the mGFR. These results support that the estimating equations, particularly CKD-EPI (CysC+SCr), may be adequate in following renal function under routine circumstances. However, when highly accurate assessments of renal function are required for management of patients with hepatic cirrhosis, or when significant ascites is present, more rigorous procedures should be considered. Methods for measuring GFR that used voluntary timed voiding urine collections after a single injection of 99mTc-DTPA should be regarded as potentially inaccurate and are not recommended unless conscientious measures can be taken to ensure completeness of the urine collections, that continuous infusion techniques are used, and that more extended intervals of sample collection can be observed.
DISCLOSURE
This research was supported by a grant from the National Institutes of Health (RO1DK088375) and by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through grant 5UL1TR001067-02. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 2, 2017.
REFERENCES
- Received for publication July 10, 2016.
- Accepted for publication January 9, 2017.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.