


Abstract
Left ventricular assist devices (LVADs) provide the ability to maintain cardiac output and sustain life as a bridge to transplantation, definitive therapy, or a permanent decision. We present a case of LVAD drive infection that was differentiated from pump infection by the use of attenuation-corrected and non–attenuation-corrected CT, along with correlation with the planar images. Clinically, the patient was suspected of having infection; however, the clinician did not know which components of the device were involved. The patient’s scan showed abnormal activity along the driveline with and without attenuation correction, whereas the pump showed abnormal activity with attenuation correction only. This finding suggested that the drive line was infected but that the activity within the pump was secondary to overcorrection of attenuation. The driveline was cultured, confirming infection.
The purpose of this teaching case study is to demonstrate the use of both attenuation-corrected and non–attenuation-corrected SPECT images when assessing for infection of intracardiac devices, in particular left ventricular assist devices (LVADs). LVADs provide the ability to maintain cardiac output and sustain life as a bridge to transplantation, definitive therapy, or a permanent decision. Potential complications include bleeding, infection, and thromboembolism. The degree and extent of infection can be difficult to discern by clinical measures, leading to imaging. Infections that involve the pump pocket can be particularly worrisome, as the best way to clear the infection would be to remove the pump. We present a case of LVAD drive infection that was differentiated from pump infection by the use of attenuation-corrected and non–attenuation-corrected CT, along with correlation with the planar images.
CASE REPORT
A 61-y-old man with ischemic cardiomyopathy and New York Heart Association class II congestive heart failure after LVAD placement presented with drainage from his drive line exit site and left upper quadrant pain creating concern about infection. The exudate was cultured, and a 67Ga scan was ordered to determine the etiology of his left upper quadrant pain and the extent of infection.
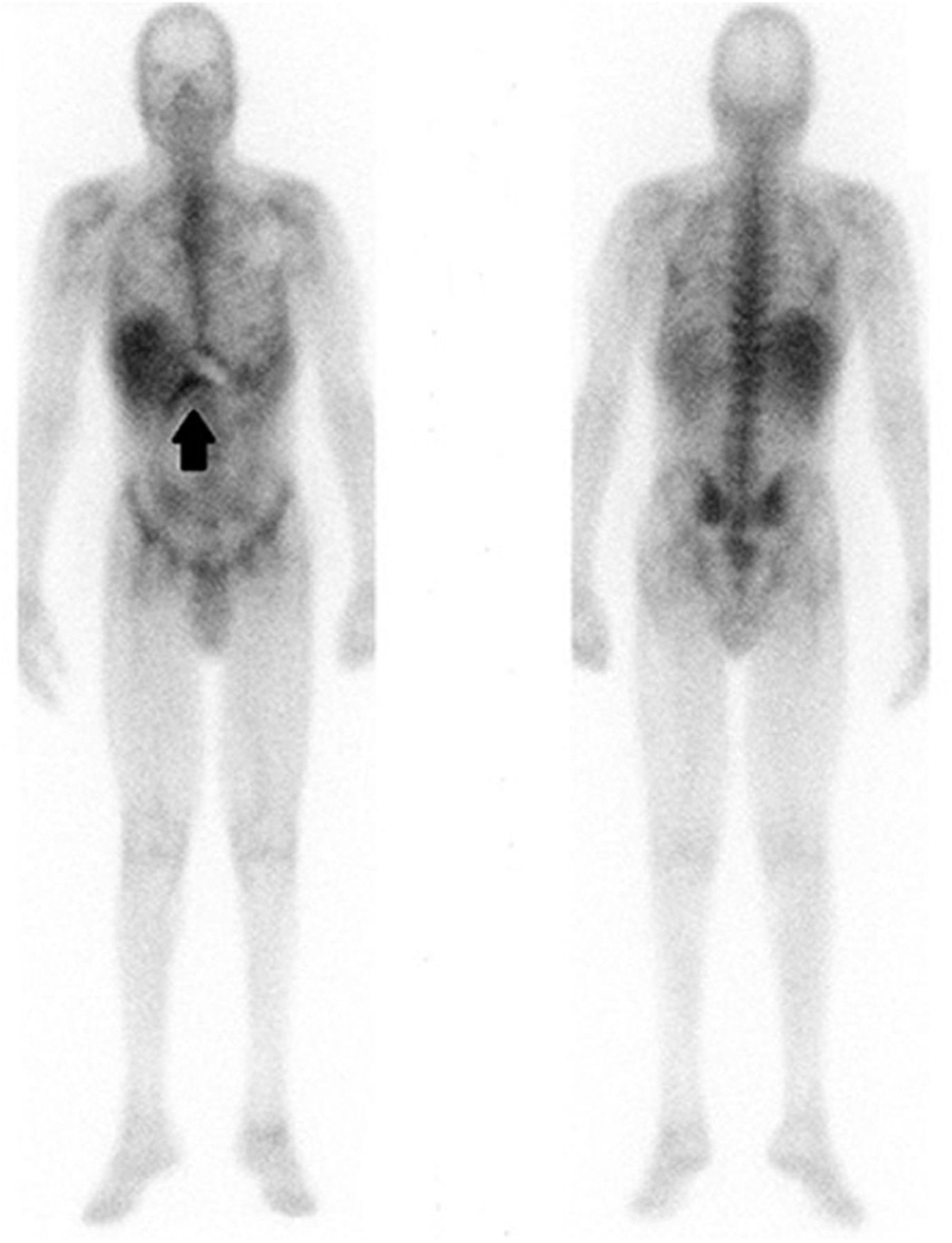
After administration of 1.9 MBq (5.2 mCi) of 67Ga, whole-body and multiple planar views were obtained at 48 h. SPECT/CT images of the lower chest and upper abdomen were obtained for better anatomic localization. The planar images demonstrated abnormal curvilinear activity (Fig. 1) along the suspected course of the LVAD drive line site, which was confirmed by SPECT/CT findings showing abnormal activity along the drive line with and without attenuation correction. The SPECT/CT scan also demonstrated intense activity within the LVAD pump. This activity was not expected as it was not seen on the planar images. The nuclear medicine physician reviewed the non–attenuation-corrected images, which showed no abnormal activity within the LVAD pump (Fig. 2). The observations from the SPECT/CT study were interpreted as consistent with infection of the LVAD driveline only. The cultured exudate was positive for Acinetobacter baumannii. Infection of the LVAD pump itself was not definitively excluded since the LVAD pump was not cultured but was unlikely given the absence of activity on non–attenuation-corrected and planar images.

Planar anterior and posterior images from whole-body 67Ga scan demonstrate curvilinear activity inferior to rib cage near liver (arrow).
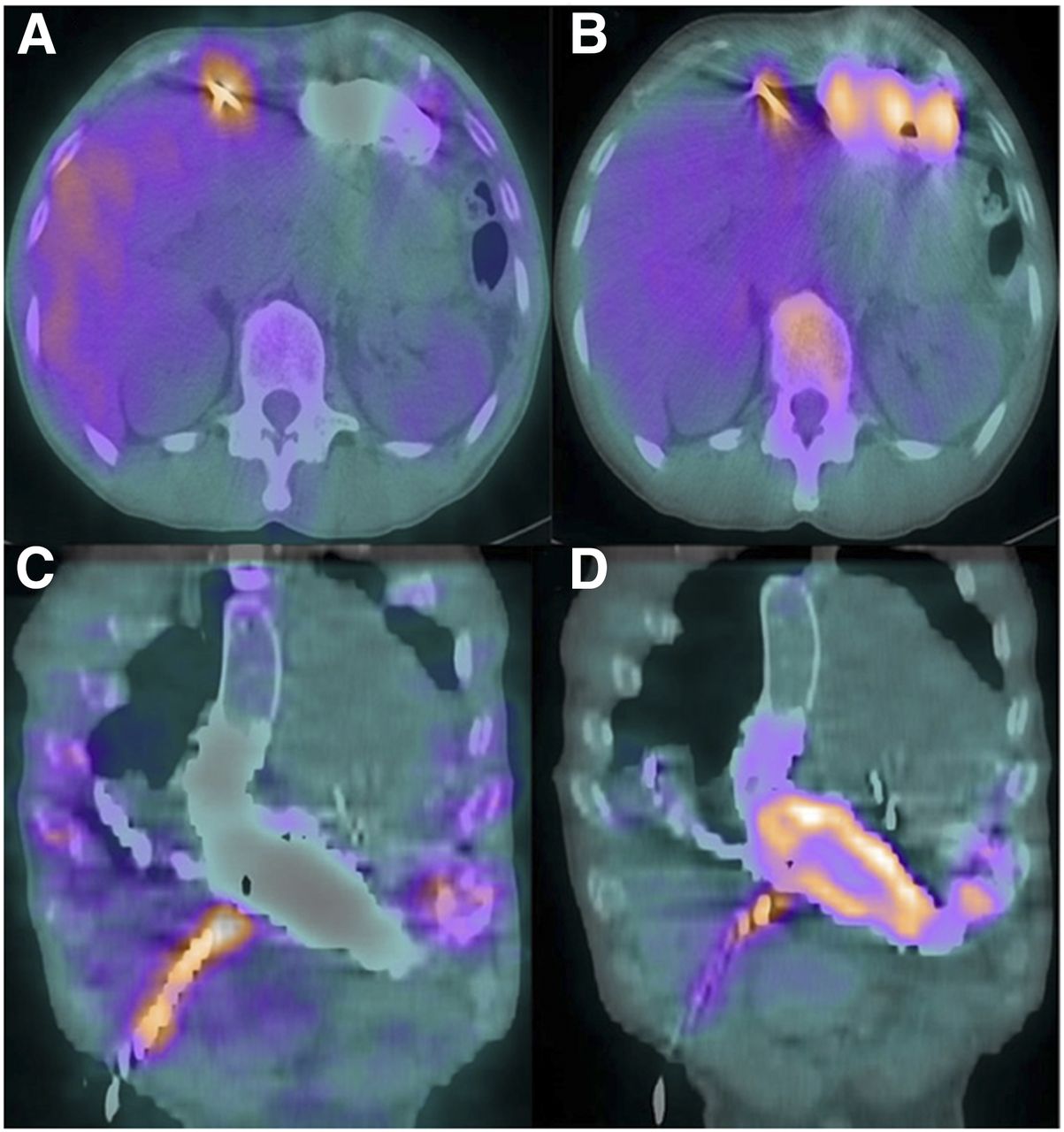
Axial SPECT without (A) and with (B) attenuation correction images, and corresponding coronal SPECT without (C) and with (D) attenuation correction. Increased activity is seen on all images within drive line, whereas pump demonstrates activity on attenuation correction images only.
DISCUSSION
Implanted intracardiac devices present a unique challenge in terms of diagnosing the presence of infection. The clinical presentation varies depending on the type of device implanted, the causative organism, the location (generator or pump pocket, subcutaneous leads, endovascular leads), and whether there is concomitant bacteremia (1). In particular, LVADs have a higher incidence of infection secondary to their large surface area, varied construction material, and crossing of several tissue planes and organ spaces (1). 67Ga and white blood cell studies offer the ability to diagnose the presence and extent of infection in a noninvasive manner (2). SPECT/CT has made it possible to determine the precise location of infection by eliminating overlap from adjacent structures and showing excellent anatomic detail. Although CT attenuation correction has the benefit of improved localization, there remains the possibility of overcorrection when imaging traverses very dense structures, resulting in an incorrectly perceived increase in radiotracer uptake (3). Therefore, this phenomenon could lead to overestimation of the extent of disease. Inaccurate details about the site of infection may lead to improper therapy, as the treatment algorithms depend on the site of infection. Attenuation correction errors with PET/CT have been previously described when dense structures are concerned; however, this phenomenon has not been described clinically with SPECT/CT (4–6).
CONCLUSION
SPECT/CT has improved the ability to localize findings on planar images; however, this teaching case study demonstrates the importance of correlating the planar images with both non–attenuation-corrected and attenuation-corrected SPECT/CT to increase the accuracy with which infections of intracardiac devices are diagnosed. Further investigations of the effectiveness of having both attenuation-corrected and non–attenuation-corrected images available at the time of image review are ongoing.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 13, 2015.
REFERENCES
- Received for publication March 2, 2015.
- Accepted for publication June 25, 2015.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.