


Abstract
In cardiac nuclear imaging, the liver is mostly remembered as a source of artifact in the left ventricular inferior wall. However, the liver may eventually display unexpected findings, which draw attention to significant noncardiac disease. In a patient referred for myocardial perfusion SPECT to investigate atypical chest pain, focal areas of increased tracer uptake revealed intrahepatic biliary dilatation.
Although the use of nuclear techniques for the diagnosis of biliary disorders is not new, as cholescintigraphy was once considered the noninvasive procedure of choice for the evaluation of biliary tract function, nuclear imaging of the biliary system is nowadays left for selected cases (1). The biodistribution of 99mTc-sestamibi, with accumulation in the liver (2), makes the hepatic image in myocardial perfusion SPECT a common source of artifact, creating either hot spots or false perfusion defects in the left ventricular inferior wall (3). On the other hand, this biodistribution enables the detection of incidental hepatobiliary abnormalities.
CASE REPORT
A 63-y-old woman with atypical chest pain was referred for myocardial perfusion SPECT. She reported prior surgical intervention in the pancreas due to pancreatitis secondary to severe hypertriglyceridemia. No follow-up regarding the abdominal intervention had been performed for several years.
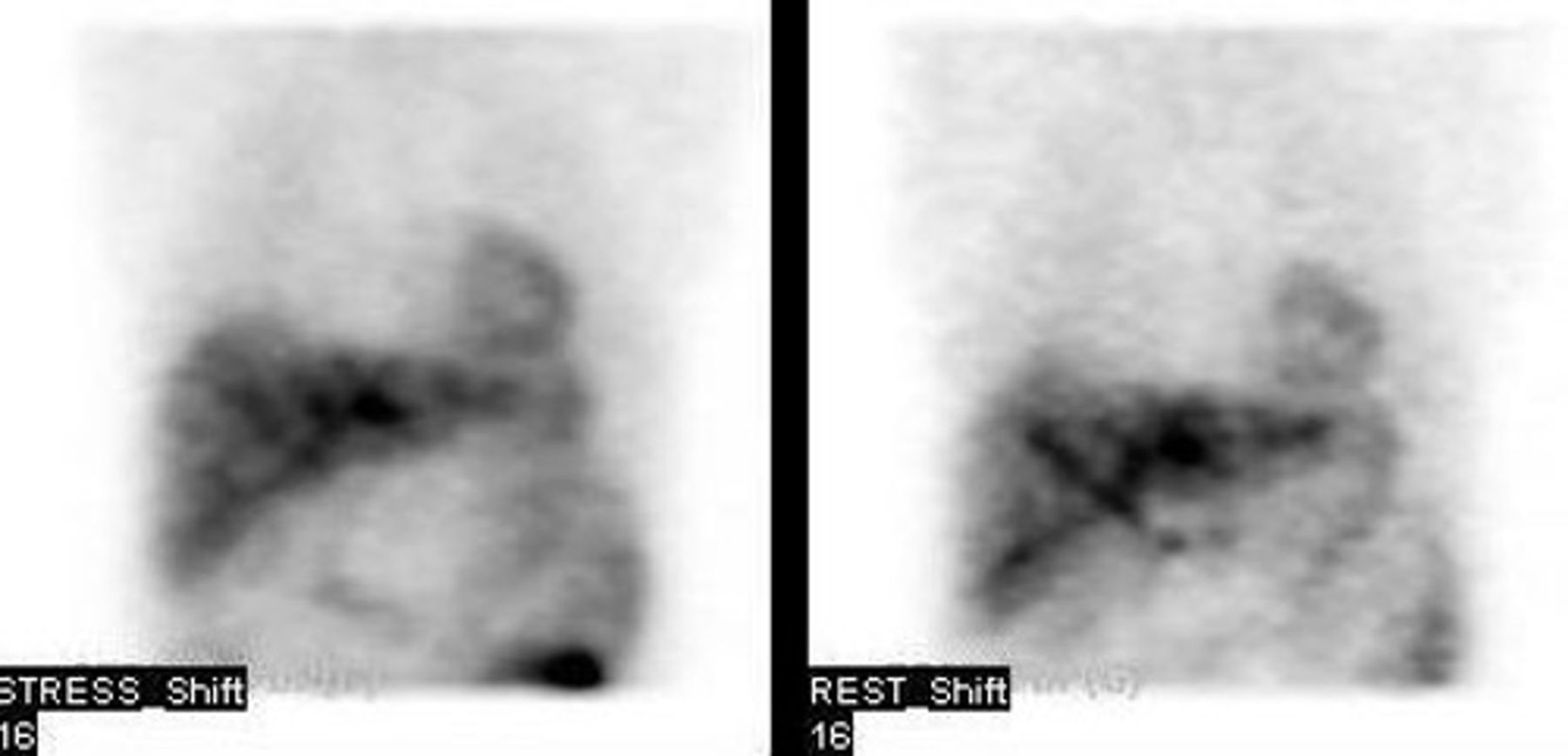
A same-day, rest–dipyridamole stress (370 MBq/1,110 MBq) 99mTc-sestamibi myocardial perfusion SPECT study was performed. Images were obtained in a dual-head camera (Millenium MG; GE Healthcare). Rest acquisition started 30 min after tracer injection. Postdypiridamole images were obtained 45 min after injection. Figure 1 shows scintigraphic findings. There were several areas of increased focal uptake in the liver, both at rest and after stress. Myocardial perfusion was considered overall normal, with a mild anteroapical perfusion defect, which was interpreted as breast attenuation in view of normal thickening and wall motion.

99mTc-sestamibi myocardial perfusion SPECT images showing several areas of increased uptake in liver. (Left) Poststress images. (Right) Rest images.
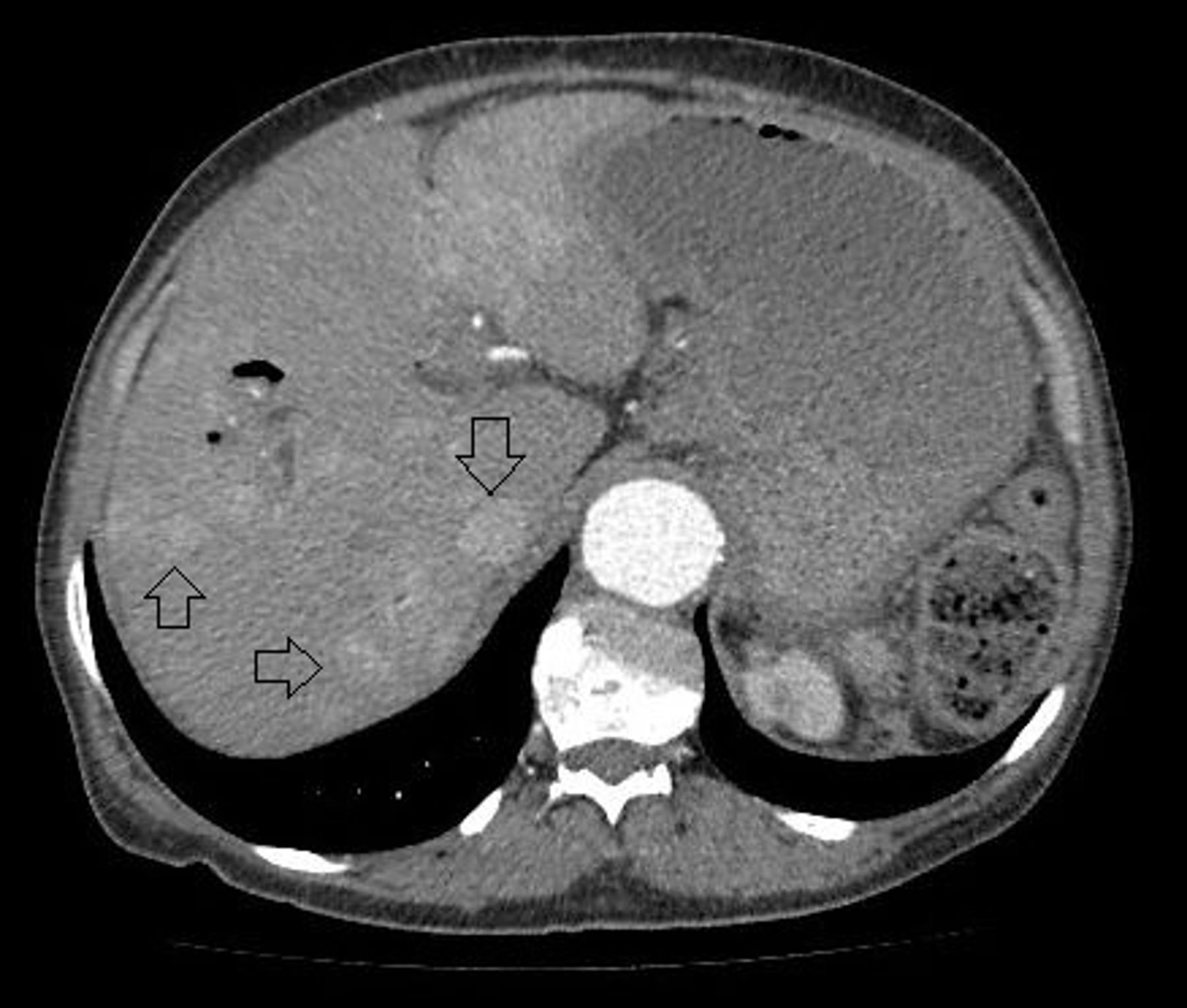
After the nuclear scan, further investigation of the liver abnormalities was indicated. The patient underwent abdominal CT scanning (Fig. 2), which revealed multiple intrahepatic biliary tract dilatations. The focal areas of increased tracer uptake in the scintigraphic images were therefore attributed to bile stasis within biliary tract dilatations. The patient was therefore referred for specialized, surgical follow-up. Laboratory evaluation showed serum bilirubin values within the reference range (total, direct, and indirect bilirubin of 1.2, 0.1, and 1.1, respectively); amylase, 21 U/L; lipase, 36 U/L; alkaline phosphatase, 779 U/L; γ glutamyl transferase, 659 U/L; fasting glucose, 359 mg/dL; and triglycerides, 2,740 md/dL. Because the patient was stable in relation to the hepatobiliary condition, no further intervention was performed. Her follow-up was noteworthy only for frequent episodes of severe hyperglycemia needing admission for glycemic control despite the domiciliary use of insulin.
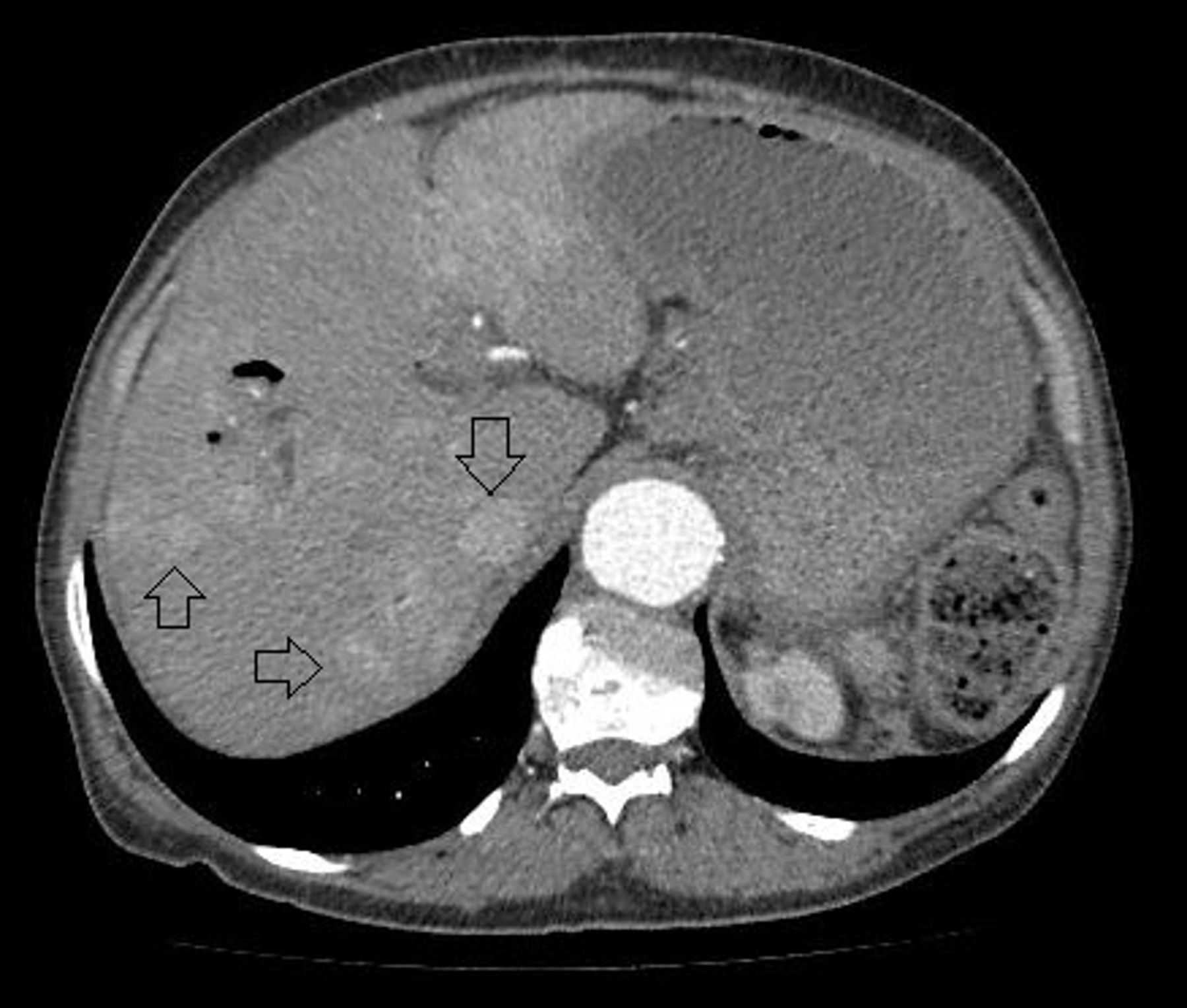
Abdominal CT scan showing multiple dilatations of intrahepatic biliary tract (arrows). Liver had normal size and parenchyma, whereas gallbladder was not visualized. Biliodigestive bypass was found, with anastomosis of common bile duct to duodenum (not shown in figure).
DISCUSSION
The case illustrates the importance of careful inspection of raw images when analyzing myocardial perfusion scintigraphy. Eventually, extracardiac findings may point toward significant subclinical disease. In this case, the biodistribution of 99mTc-sestamibi enabled the detection of biliary abnormalities, because tracer excretion into the biliary system occurs as long as liver uptake of 99mTc-sestamibi decreases, 30–60 min after injection (2,4).
CONCLUSION
In cardiac nuclear imaging, attention must be given to extracardiac findings, as these may uncover relevant pathology. Early diagnosis of disease may have important clinical implications, with impact on the patient’s prognosis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 25, 2015.
REFERENCES
- Received for publication March 28, 2015.
- Accepted for publication May 1, 2015.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.