


Abstract
Myocardial perfusion imaging (MPI) with SPECT is widely adopted in clinical practice but is associated with a relatively high radiation dose. The aim of this study was to determine the minimum product of tracer dose and scan time that will maintain diagnostic value for cadmium zinc telluride (CZT) SPECT MPI. Methods: Twenty-four patients underwent clinically indicated stress MPI using CZT SPECT and a body weight–dependent (3 MBq/kg) 99mTc-tetrofosmin tracer dose. Data were acquired for 8 min in list mode. Next, images were reconstructed using 2-, 4-, 6-, and 8-min time frames. Differences between the 8-min reference scan and the shorter scans were determined in segmental uptake values (using the 17-segment cardiac model), ejection fraction, and end-diastolic volume. A 5% difference in segmental uptake was considered to significantly influence the diagnostic value. Next, the quality of the 4-, 6-, and 8-min scans was scored on a 4-point scale by consensus by 3 experienced nuclear medicine physicians. The physicians did not know the scan time or patient information. Results: Differences in segmental uptake values, ejection fraction, and end-diastolic volume were greater for shorter scans than for the 8-min reference scan. On average, the diagnostic value was influenced in 7.7 segments per patient using the 2-min scans, in comparison to 2.0 and 0.8 segments per patient using the 4- and 6-min scans, respectively. In addition, the 4-min scans led to a significantly reduced image quality compared with the 8-min scans (P < 0.05). This was not the case for the 6-min scan. Conclusion: Six minutes was the shortest acquisition time in stress MPI using CZT SPECT that did not affect the diagnostic value for a tracer dose of 3 MBq/kg. Hence, the patient-specific product of tracer dose and scan time can be reduced to a minimum of 18 MBq·min/kg, which may lower the effective radiation dose for patients to values below 1 mSv.
For patients with suspected stable coronary artery disease, testing for ischemia is strongly recommended before invasive coronary angiography (1,2). Multiple tests are available for this purpose, of which myocardial perfusion imaging (MPI) with SPECT is the most validated noninvasive method (3).
MPI using SPECT is widely adopted in clinical practice. Yet, this modality is also known to be a large contributor to the cumulative effective radiation dose from medical sources in the general population, accounting for more than 22% of the total effective dose in the United States (4). Despite the introduction of more sensitive γ cameras, such as cadmium zinc telluride (CZT)–based systems, as well as a general awareness of radiation burden, the tracer dose that should be administered has remained largely unchanged over the last decade (5–7). Initially, research on these new cameras focused on decreasing the scan time while maintaining the image quality at a level similar to that of conventional sodium iodide–based γ cameras (8–10). Nakazato et al. reported the minimum number of counts needed in CZT SPECT to provide reproducible results similar to those of a conventional camera (11). Furthermore, Einstein et al. recently validated a low-dose CZT SPECT protocol by comparing it with conventional SPECT (12). However, these studies did not assess the minimum number of counts or scan time needed to maintain the diagnostic value of CZT SPECT. Therefore, the aim of our study was to determine the minimum tracer dose–scan time product (TDSTP) that will maintain the diagnostic value of stress MPI using CZT SPECT.
MATERIALS AND METHODS
Study Population
We retrospectively included 24 consecutive patients who underwent clinically indicated stress MPI using CZT SPECT (Discovery NM 570c; GE Healthcare). This study was approved by the local ethics committee, and all patients gave written informed consent for the use of their data for research purposes, including the collection of multiple patient-specific parameters and coronary artery disease risk factors.
Patient Preparation and Acquisition
Patients were asked not to use any nicotine or caffeine-containing beverages for 24 h before scanning and to discontinue dipyridamole for 48 h before scanning. Pharmacologic stress was induced by intravenous adenosine (140 μg/kg/min for 6 min) or regadenoson (5 mL with 400 μg for 15 s followed by a saline flush). Only pharmacologic stress was used for logistic reasons, in particular the high patient throughput in our center (13). A body weight–dependent tracer dose of 3 MBq/kg was administered intravenously at peak stress to minimize the influence of patients’ physical characteristics on the image quality (7).
Patients were scanned supine 45–60 min after injection, with their arms placed above their heads. Before scanning, the patient’s chest was positioned in the center of the CZT SPECT scanner using real-time persistence imaging. Images were acquired for 8 min using a 20% symmetric energy window centered at 140 keV. Data were acquired in list mode.
The dedicated heart CZT SPECT system that we used has been described repeatedly in the literature (5,6,13,14). In short, the scanner uses 19 pinhole detectors centered around the myocardium containing 32 × 32 pixelated (2.46 × 2.46 mm) highly sensitive CZT elements.
Images were reconstructed using 2-, 4-, 6-, and 8-min time frames by applying an iterative reconstruction algorithm with maximum-likelihood expectation maximization (Xeleris, version 3.0562; GE Healthcare). The scans were displayed in traditional short, vertical long, and horizontal long axes. To prevent additional reproducibility influences, CT-based attenuation correction was not applied in this study (15). In addition, the ejection fraction (EF) and end-diastolic volume (EDV) were determined for all scans (Xeleris).
Quantitative Analysis
The measured number of photon counts in the 19 pinhole detectors were determined for each scan time. We then created circumferential polar plots for all MPI scans, representing the percentage of tracer uptake in the 17 myocardial segments (16–18). In these polar plots, the segmental uptake values were normalized and presented as the percentage of the maximum myocardial regional uptake (16–18). For each segment, the uptake differences were determined between the 8-min scan (referred to as the 8-min reference scan) and the 2-, 4-, and 6-min scans (referred to as the shorter scans). Next, for each of the 17 segments, the percentage of patients with an absolute segmental uptake difference of more than 5% was determined. Furthermore, the number of segments with an uptake difference of 5% was determined for each patient for all scans. An uptake difference of 5% is generally associated with possible ischemia and is considered to significantly influence the diagnostic value (19,20). In addition, a subanalysis assessing only the outer (1–6) and only the inner (7–17) segments was performed to account for reproducibility errors (15). Finally, we calculated the mean absolute differences in EF and EDV between the 8-min reference and shorter scans.
Qualitative Analysis
The image quality of the 4-, 6-, and 8-min MPI scans was assessed to determine possible noninferiority of the shorter scans compared with the 8-min reference scan. Three experienced nuclear medicine physicians scored the reconstructed images by consensus using a 4-point scale (1, poor; 2, fair; 3, good; 4, excellent). The following parameters were considered: myocardial shape, uptake density and uniformity, endocardial and epicardial edge definition, and myocardium-to-noise ratio (7). In addition, each observer scored diagnostic confidence in image interpretation as sufficient or insufficient, where sufficient indicates enough confidence to make a follow-up decision based on image quality. All interpreters were masked to patient characteristics and scan times. Moreover, all scans were presented in random order.
Statistics
Patient-specific parameters and characteristics were determined as mean ± SD using Stata (StataSE, version 12.0). The mean absolute differences in segmental uptake values, EF and EDV with the 8-min reference scans were compared between the 2-, 4-, and 6-min scans using the Wilcoxon signed-rank test. The number of segments influencing the diagnostic value per patient was compared between the 2-, 4-, and 6-min scans using the Wilcoxon signed-rank test. Image quality between the 8-min reference scan and the 4- and 6-min scans was also compared using the Wilcoxon signed-rank test. To compare mean diagnostic confidence in image interpretation between the 8-min reference scan and the shorter scans, the Cochran Q-test was used. The level of statistical significance was set to 0.05 for all statistical analyses.
RESULTS
The baseline characteristics of all included patients are summarized in Table 1.
Baseline Characteristics and Scan Results for All 24 Stable Patients with Suspected Coronary Artery Disease Referred for CZT SPECT
Quantitative Analysis
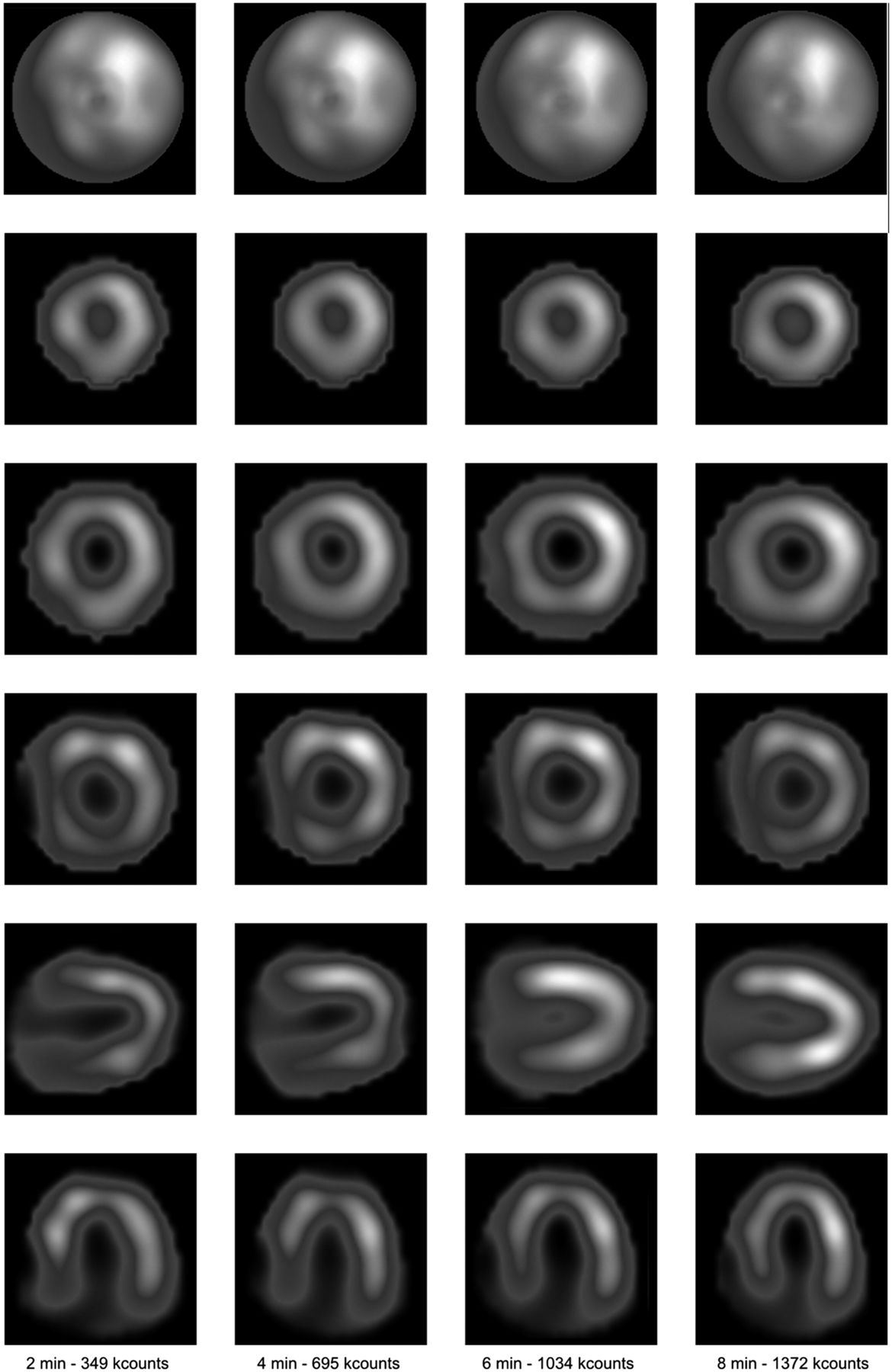
The mean measured photon counts were 303 ± 54, 604 ± 105, 902 ± 157, and 1,196 ± 211 kilocounts using a scan time of 2, 4, 6, and 8 min, respectively. The mean absolute differences in tracer uptake between the 8-min reference and the shorter scans in each of the 17 segments increased significantly for the shorter scans (P < 0.001), as shown in Table 2. These differences decreased from 6.2% ± 4.8% to 3.4% ± 3.0% and 2.2% ± 2.1% for the 2-, 4-, and 6-min scans, respectively.
Absolute Differences and Segmental Uptake Values, EFs, and EDVs Comparing the 8-Minute Reference Scan with the Shorter Scans
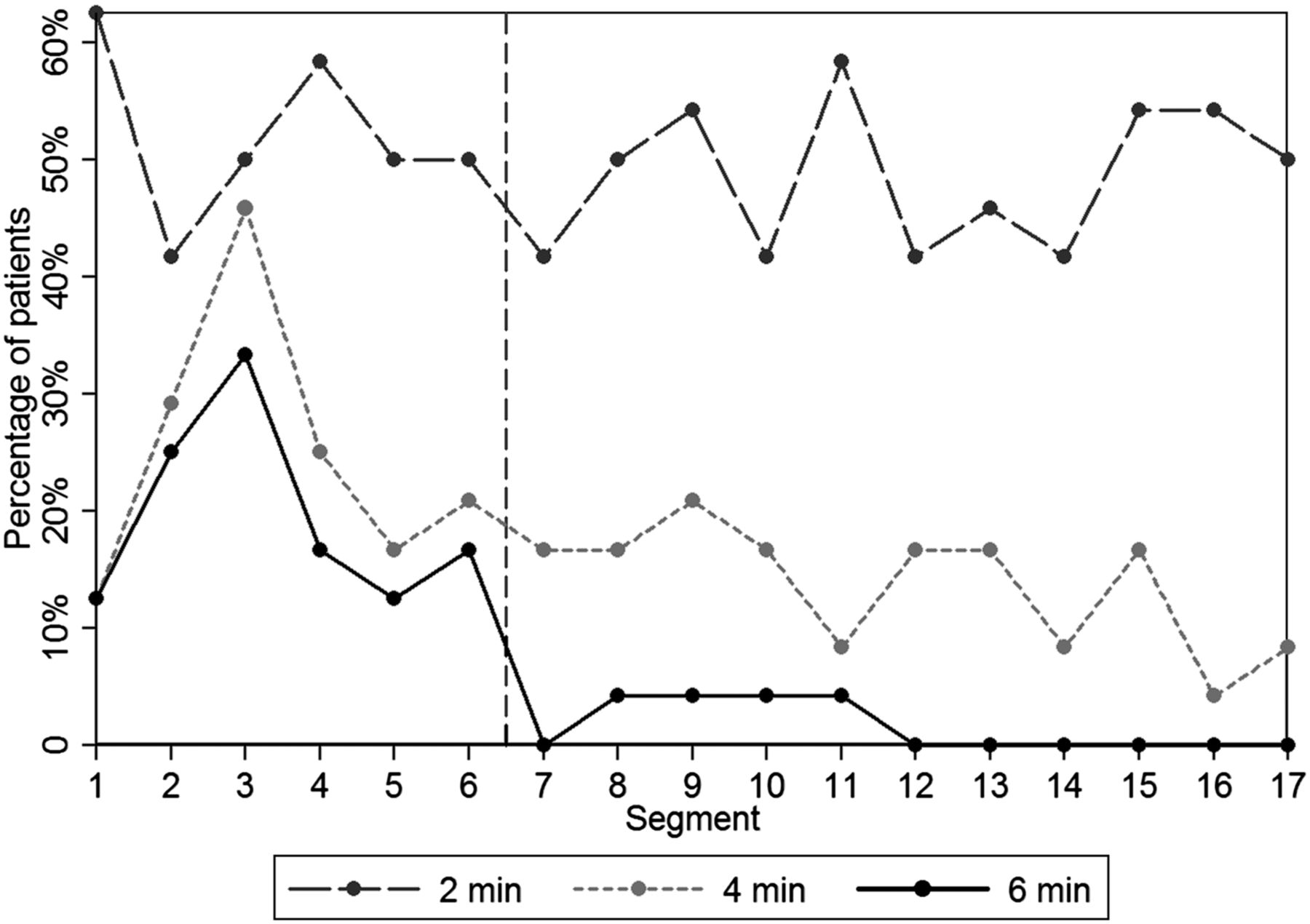
For each of the 17 segments, a decrease in scan time led to more patients in whom the diagnostic value was influenced, as illustrated in Figures 1 and 2. In the 4- and 6-min scans, an influence on diagnostic value was seen for far more patients for the outer segments (segments 1–6) than for the inner segments (segments 7–17).
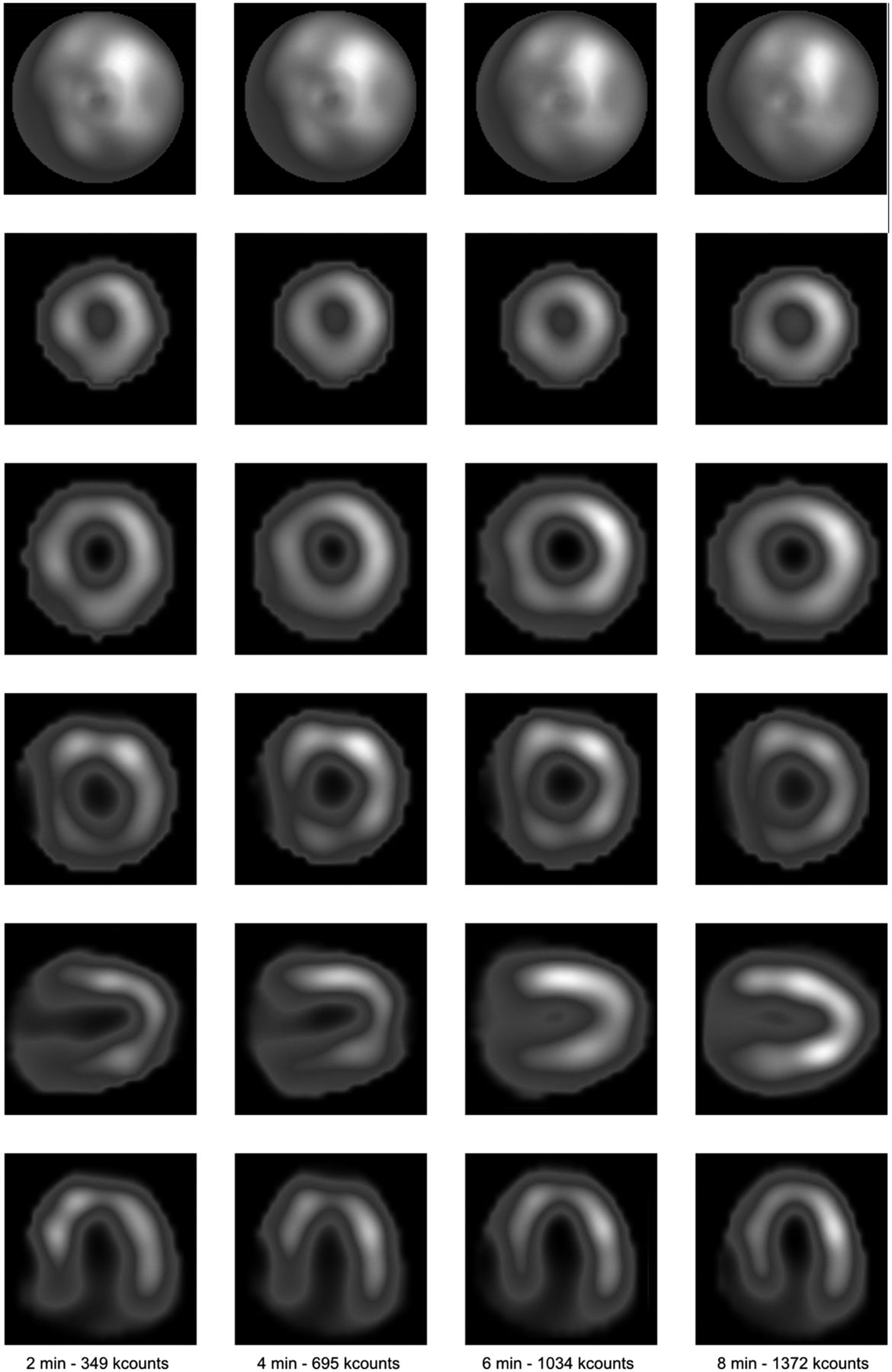
Example of stress MPI using CZT SPECT scans with varying scan times and their corresponding measured photon counts. Scans are from the typical patient (55-y-old woman, 61 kg, 21.1 kg/m2 body mass index, administered 187 MBq). Shown from top to bottom are corresponding bull’s-eye image, 3 short-axis slices (from apical to basal), vertical long-axis slice, and horizontal long-axis slice. For all axes, the same locations are shown for each scan time.
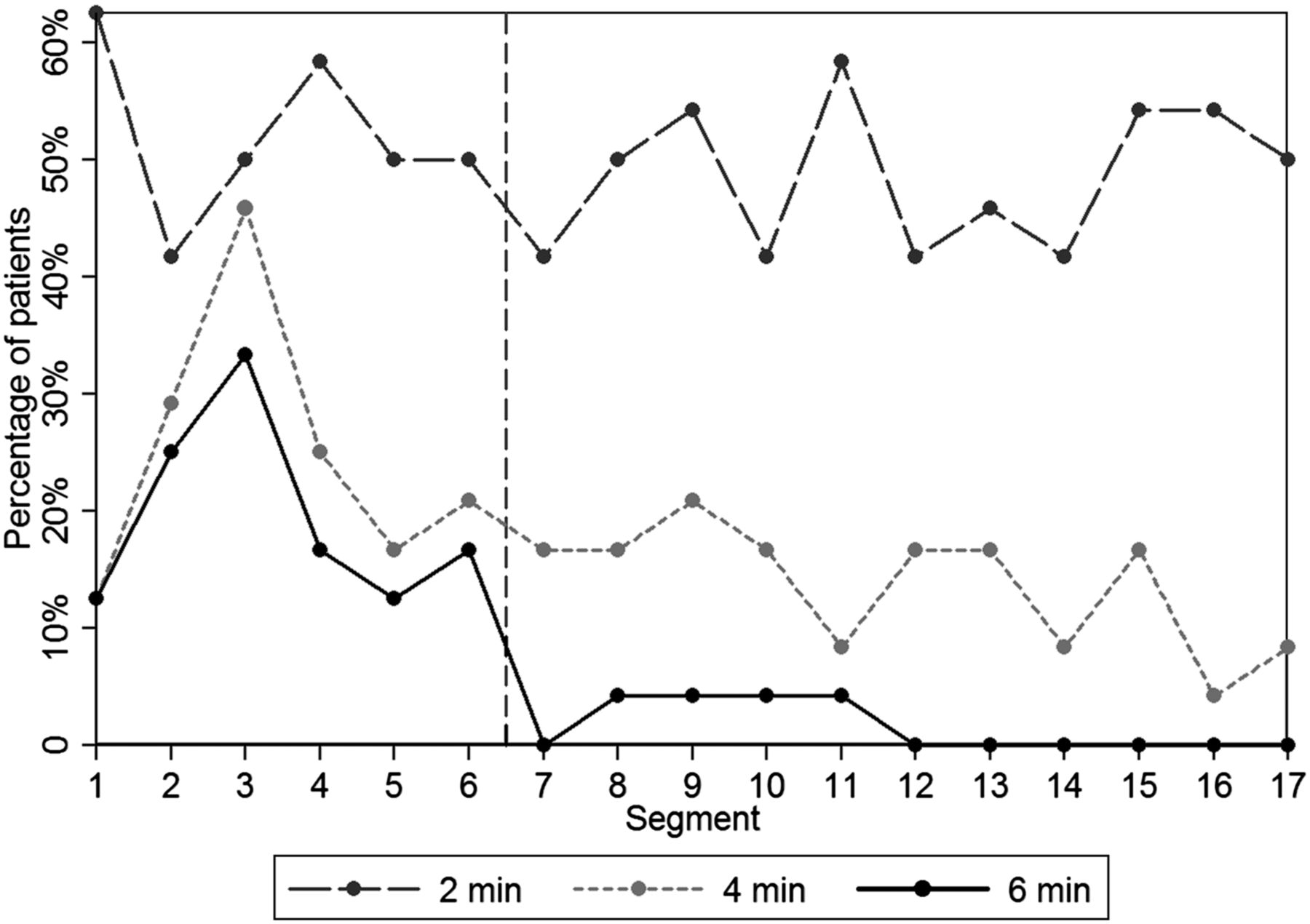
Percentage of patients who had more than a 5% absolute difference in segmental uptake between 8-min reference scan and 2-, 4-, and 6-min scans, for each of the 17 segments. For example, segment 7 was affected in 42% of patients when the scan time was reduced to 2 min, whereas this percentage was 17% and 0% for the 4- and 6-min scans, respectively. The vertical dashed line represents the separation between the inner and outer segments.
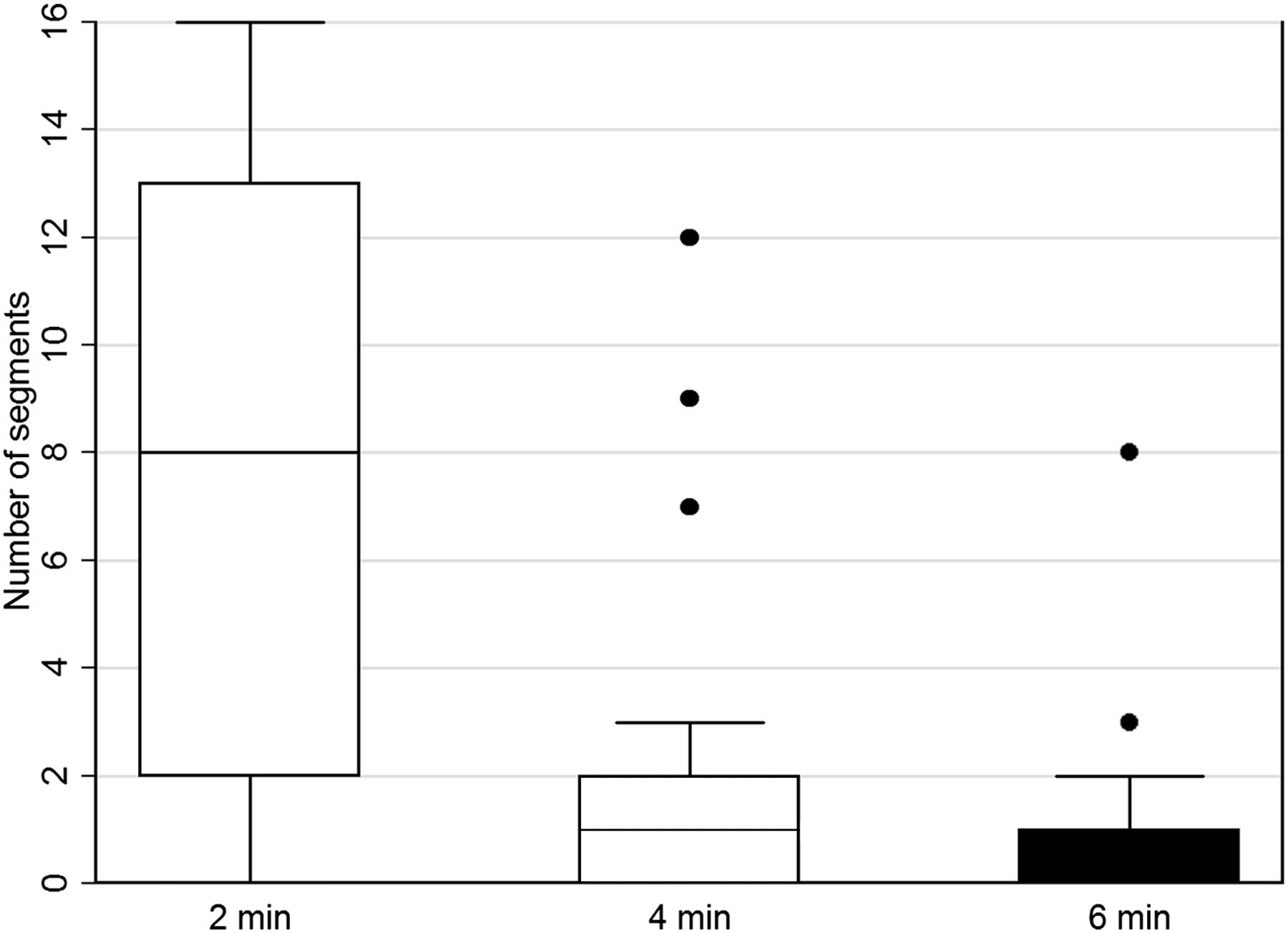
The use of the 2-min scans led to more segments in which the diagnostic value per patient was influenced, as illustrated in Figure 3. The mean number of influenced segments compared with the 8-min scan decreased significantly from 7.7 ± 5.4 to 2.0 ± 3.1 and 0.8 ± 1.7 for the 2-, 4-, and 6-min scans, respectively (P ≤ 0.013).

Box plot of the number of segments per patient that showed segmental uptake difference of 5% or more for 2-, 4-, and 6-min scans compared with the 8-min reference scan. Black lines within the box represent median, box demarks 25th and 75th percentiles (interquartile range), and whiskers demark highest and lowest numbers of segments that are not outliers. Values that are more than 1.5 times interquartile range are represented by dots.
The mean absolute difference in EF and EDV when the 8-min reference scan was compared with the shorter scans increased when scan time decreased, as shown in Table 2. The absolute differences in EF differed significantly between the reference scan and the 2-, 4-, and 6-min scans (P < 0.04). Yet, the absolute differences in EDV were significant only when the 2-min scan was compared with the 6-min scan (P < 0.04). No significant differences were found for either EF or EDV when the mean absolute difference of the 4- and 6-min scans was compared.
Qualitative Analysis
Because the 2-min scans were found to be inferior to the 4-, 6-, and 8-min scans, the 2-min scans were not incorporated in the image quality assessment.
Image quality was scored as good or excellent by the physicians for 46%, 75%, and 67% of the 4-, 6-, and 8-min scans, respectively, as shown in Figure 4. No difference in image quality was found between the 6- and 8-min scans (P = 0.43). However, the mean image quality of the 4-min scans was inferior to that of the 6- and 8-min scans (P < 0.05).

Scored image quality for myocardial scans for all 24 patients using scan times of 4, 6, and 8 min. Image quality was scored on 4-point grading scale by consensus of 3 experienced, masked nuclear medicine physicians. Image quality was lower for 4-min scans than for 6- or 8-min scans (P < 0.05).
The mean diagnostic confidence in image interpretation remained unchanged when shorter scans were used (P = 0.93), as both the 4- and 6-min scans yielded adequate diagnostic confidence in 92% of all cases, versus 93% for the 8-min scans.
DISCUSSION
In this study, we have demonstrated that 6 min was the shortest acquisition time that maintained the diagnostic value in terms of segmental uptake values, EF, and EDV, in patients administered 3 MBq/kg for stress MPI using CZT SPECT. Scan times of 2 or 4 min led to a substantially lower diagnostic value and are therefore not recommended.
Our results can be compared with previously reported low-dose protocols using TDSTP. The TDSTP accounts for both the recommended tracer dose and the scan time and therefore allows easy comparison between varying protocols. Assuming a patient of 80 kg, our proposed TDSTP is 1,440 MBq·min for stress imaging (18 MBq·min/kg). This dose is even lower than the recently proposed low-dose protocol by Einstein et al. with a TDSTP of 1,690 for an average patient (12). Yet, the minimal tracer dose to administer was not determined in this study, and rest rather than stress images were used. Moreover, our proposed protocol is higher than the previously reported low-dose CZT SPECT protocols using 1,210 MBq·min, as suggested by Nakazato et al. (11), and 981 MBq·min, as suggested by Herzog et al. (8). Yet, both research groups determined the TDSTP to achieve the same image quality or diagnostic value as obtained with their conventional γ camera instead of aiming for the minimum TDSTP needed to maintain the diagnostic value acquired using a CZT-based SPECT camera. Consequently, the TDSTP for a conventional camera differed between the two studies, which may explain the differences in the recommended TDSTP using a CZT camera. Furthermore, the dose regime proposed by Herzog et al. (8) is comparable to a scan time of 4 min in our study. Considering our results, the use of a 4-min scan time can be associated with lower diagnostic value and image quality than the use of a scan time of 6 or 8 min. This finding might indicate that CZT SPECT provides a higher diagnostic value and image quality than conventional γ cameras. This indication is in agreement with 2 previous studies. Mouden et al. compared the need for additional imaging and the 1-y outcome between CZT SPECT and conventional cameras (13). They showed that using CZT SPECT resulted in more normal scans with identical clinical outcome after 1 y of follow-up. Furthermore, although Einstein et al. did not find any diagnostic differences between conventional and CZT SPECT when using a low-dose protocol, they did find an improvement in image quality using CZT SPECT (12).
Although differences were observed in segmental uptake values, EDV, and EF between the 6- and 8-min scans, the 6-min scans were considered to achieve the same diagnostic value as the 8-min scans. Koopman et al. showed that the diagnostic value was influenced in 18%–43% of all outer segments and 0%–16% of all inner segments because of reproducibility errors (15). Comparing these errors with our data shows that the observed differences in segmental uptake for the 6-min scans are likely due to reproducibility errors. The 2- and 4-min scans revealed higher differences than the reported reproducibility errors, indicating the loss in diagnostic value for these scan times. In addition, Cherk et al. reported a reproducibility error of more than 5% in the SD of the differences in determining the EF using CZT SPECT (21). Although we did not determine the SD of the difference in EF in this study, the results of Cherk et al. suggest that a large part of our observed differences in EF will presumably be due to reproducibility errors.
Several assumptions were made in this study. First, the 8-min reference scan (TDSTP of 24 MBq·min/kg) was considered to provide a sufficient diagnostic value in all patients. Although it was not tested whether a higher TDSTP would further improve diagnostic value, a TDSTP of 24 MBq·min/kg is almost twice as high as the TDSTP previously suggested for CZT SPECT (8,11). Moreover, the influence of patient’s physical characteristics on the study outcomes was considered to be eliminated because of the use of a patient-specific dose protocol (7). Second, the diagnostic value was influenced in the quantitative assessment when shorter scans were used, but this effect was not observed in the qualitative assessment, as illustrated in Figures 2 and 4. The randomized and masked design of the qualitative image assessment resulted in scoring of the appearance of the scans and not of possible emerging defects corresponding with the diagnostic value. Therefore, the qualitative assessment should be interpreted solely as a measurement of scan appearance instead of diagnostic value. This might also explain the absence of differences in the scored diagnostic confidence between the 4-, 6-, and 8-min scans. Third, only the minimum TDSTP in stress MPI was determined. Yet, we recommend the same TDSTP for rest as for stress MPI when using a 2-d protocol, as mentioned in EANM/ESC and ASNC procedural guidelines (16,17). When using a 1-d stress–optional rest protocol, we assume that administering a rest tracer dose of triple the stress dose, as recommended in guidelines (16,17), would automatically lead to sufficient image quality in rest MPI. Finally, to prevent inclusion of additional errors, CT-based attenuation correction was not applied in this study (15). Yet, when attenuation correction is applied on (hypothetically) identical 6- and 8-min scans, they will still be identical after correction. Moreover, as indicated by Heller et al., attenuation correction will lead to more reliable diagnosis only when the original scans have sufficient photon counts (22). Hence, applying attenuation correction on the 2- or 4-min scans, associated with an insufficient photon count, would only introduce additional errors, possibly influencing the results.
Our findings show a possible reduction of 25% in tracer dose or scan time when a dose regimen of 24 MBq·min/kg is applied (7). For a 10-min acquisition time, the administered dose for stress MPI will be 1.8 MBq/kg, associated with an effective dose of approximately 1 mSv for an average patient of 80 kg (23). In comparison, the mean effective dose associated with CT angiography can be as low as 3 mSv, whereas a diagnostic cardiac catheterization can be associated with a mean effective dose of 7 mSv (4,24). Consequently, if this proposed dose reduction is widely adopted in clinical practice, MPI may no longer be the largest contributor to the effective dose in the general population (4).
CONCLUSION
Six minutes is the shortest acquisition time that does not affect diagnostic value when a tracer dose of 3 MBq/kg is applied for CZT SPECT stress MPI. Hence, the TDSTP can be minimized to 18 MBq·min/kg. This adjustment may lower the effective radiation dose for patients to values below 1 mSv.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 22, 2015.
REFERENCES
- Received for publication September 16, 2014.
- Accepted for publication November 10, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}