


Abstract
Although incidental pituitary findings on 18F-FDG PET are uncommon, there are several reports published in the literature. It is believed that this is the first reporting of incidental pituitary disease found on O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) PET imaging. The case provides valuable insight into pathogenesis, diagnostic tools, and related pathology. The power of 18F-FET in differentiating cerebral metastases and recurrence in patients who had previous surgical and radiation therapy is highlighted, and the incremental benefits over MR imaging and 18F-FDG PET are outlined. The case represents an uncommon finding on MR imaging and 18F-FDG PET and a rare finding on 18F-FET PET.
Although the efficacy of glucose analogue imaging is widely reported for imaging in oncology, radiolabeled amino acids have emerged as valuable molecular probes because tumors tend to have high amino acid metabolism. A number of amino acid molecular probes are available to expand the tools available to clinicians. This is particularly relevant in the evaluation of brain tumors.
CASE REPORT
A 54-y-old woman with breast cancer was treated with chemotherapy, radiation therapy, and mastectomy and underwent craniotomy to remove a metastatic tumor. The patient subsequently developed widespread metastatic disease in the skeletal system requiring further chemotherapy. At follow-up, cerebral metastases in the right parietal lobe were noted and treated with γ-knife therapy. The patient first presented to us for imaging to investigate dizziness and seizures 12 mo after the γ-knife surgery.
MR imaging indicated that there was an enhancing mass within the inferior aspect of the right parietal lobe, posterior to the superior aspect of the right insular cortex (Fig. 1). This mass measured approximately 1.8 cm in maximum diameter, and there was extensive surrounding edema extending into the right frontal and parietal lobes, with associated sulcal effacement. The lesion had been measured at 9 mm in diameter on previous studies. The patient was referred for an 18F-FDG PET/CT scan to evaluate for residual disease, recurrence, and progression.
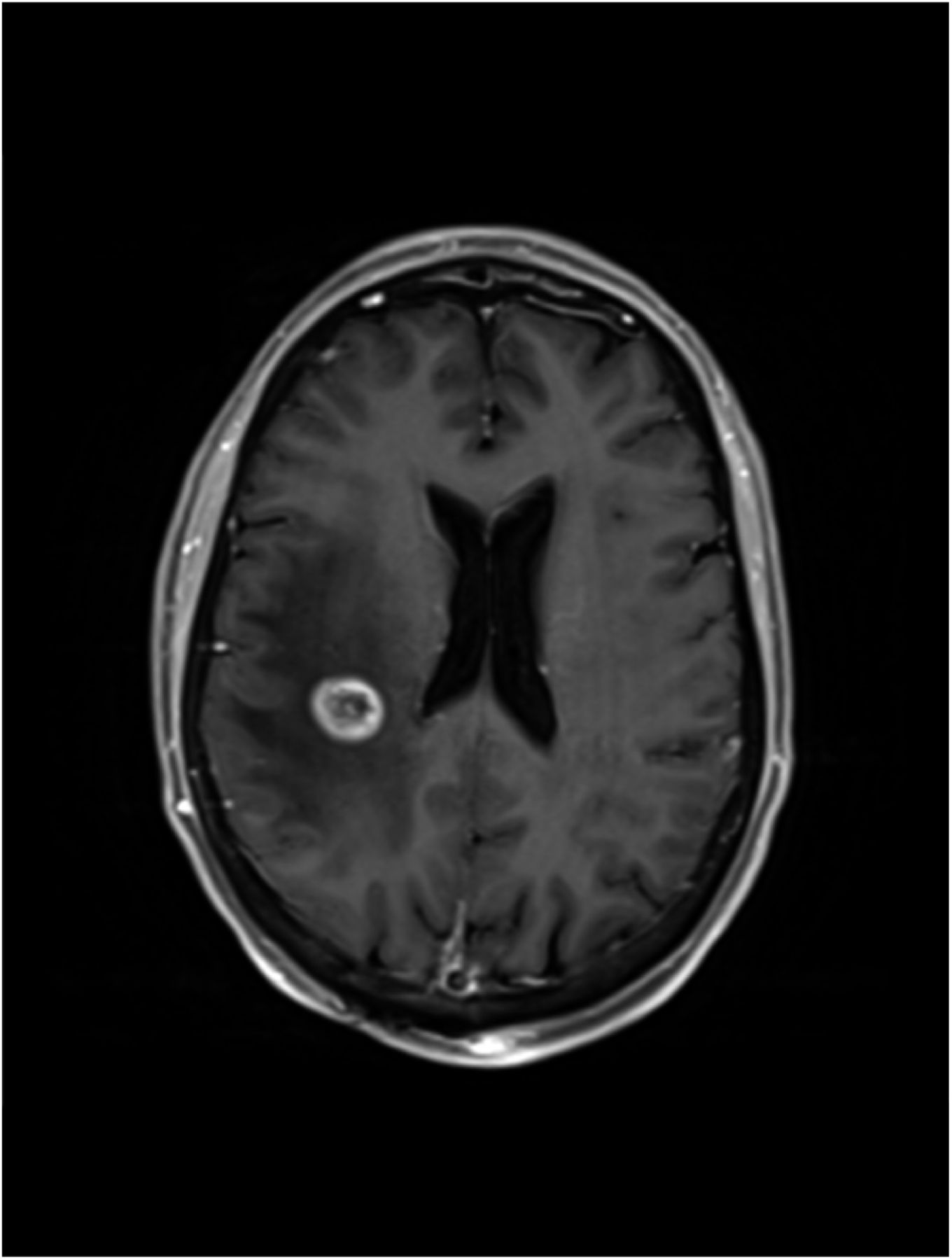
Axial T1-weighted fat-saturation post-gadolinium MR image highlighting enhancing mass.
PET/CT was performed after a 6-h fast (blood glucose concentration, 4.6 mmol/L), intravenous administration of 265 MBq of 18F-FDG, and a 50-min uptake period. Whole-body imaging was performed from the vertex of the skull to below the knees using a Discovery time-of-flight PET/64-slice CT scanner (GE Healthcare). Diagnostic-quality, contrast-enhanced CT was performed through the brain, chest, abdomen, and pelvis, with low-dose CT imaging performed elsewhere for attenuation correction and lesion localization. Water was used as an oral contrast agent to assist in bowel distension. Multiplanar and volume reconstruction was generated, as well as fusion imaging.
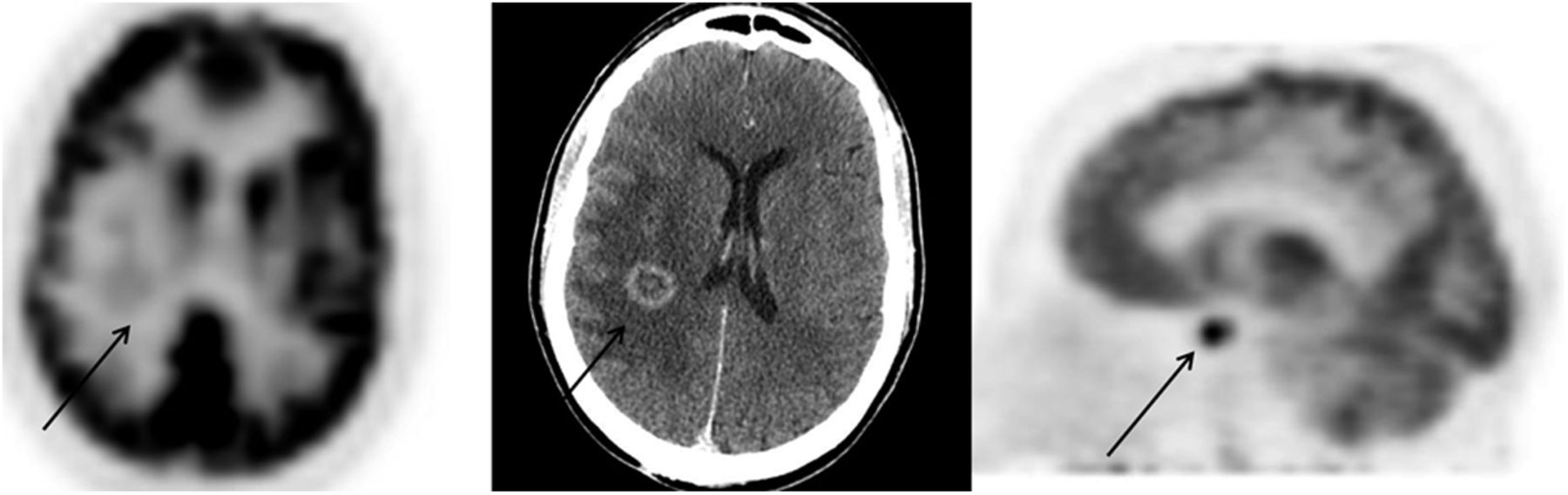
Widespread metastatic disease was seen in the thoracic spine and ribs. The lesion of interest in the right parietal lobe had a peripheral rim of prominent contrast enhancement and considerable surrounding edema; the peripheral enhancing rim had only mild-grade 18F-FDG uptake with a maximum standardized uptake value (SUVmax) of 10.2 (Fig. 2). The findings were considered consistent with viable tumor. No uptake was present in the areas of edema seen extending into the adjacent frontal lobe and parietal lobe on MR imaging. There was reduced uptake in the gray matter superficial to the focal lesion, consistent with previous radiotherapy or related deafferentation. An occipital prosthesis was also noted consistent with previous craniotomy. The 18F-FDG PET study also demonstrated intense uniform tracer accumulation in the pituitary (Fig. 2). Pituitary adenomas are a common (4%–20% of brain studies) incidental finding on CT and MR imaging (1,2) but uncommon on 18F-FDG PET (0.8%). When pituitary is incidentally noted on 18F-FDG PET, adenoma is the confirmed pathology 90% of the time (3).
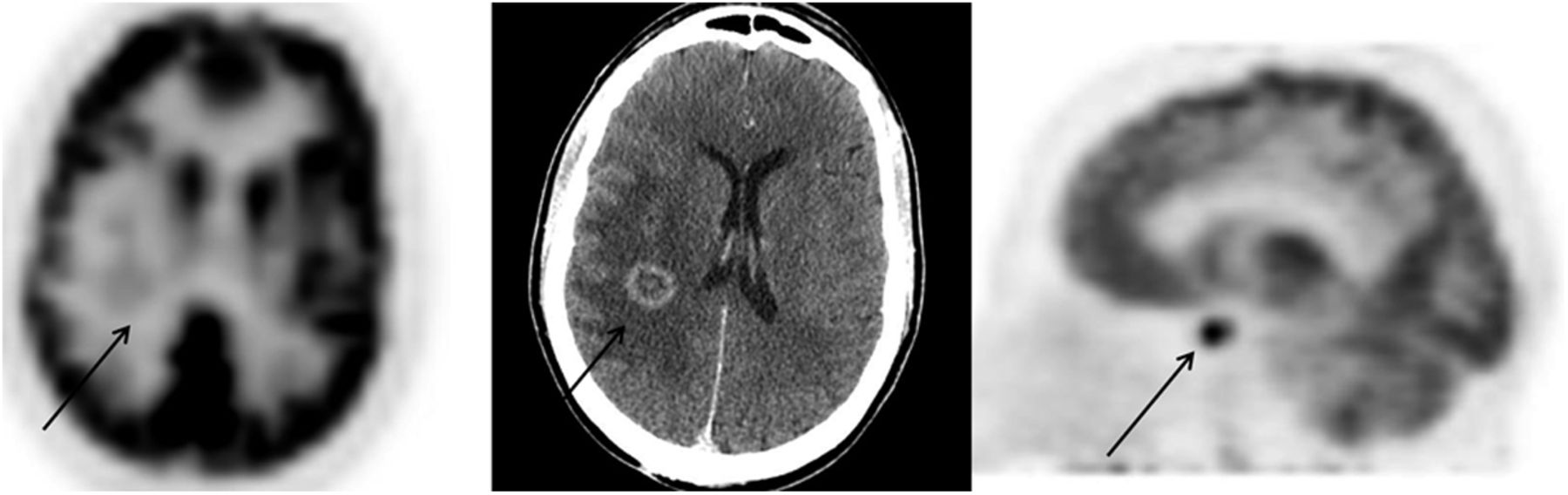
18F-FDG PET scan (left) demonstrating mild 18F-FDG avidity (arrow) in parietal lesion noted on CT (center). PET/CT image coregistration (not shown) revealed no uptake in areas of edema on CT and MR imaging, with subtly increased 18F-FDG accumulation corresponding to described lesion. 18F-FDG accumulation in pituitary (right) on PET confirms that activity is localized to pituitary.
PET/CT imaging with O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) was recommended to further evaluate the right parietal lobe lesion. 18F-FET has shown superiority over 18F-FDG in differentiating tumor from inflammatory tissue (4), particularly in patients who had previous surgery or radiation therapy.
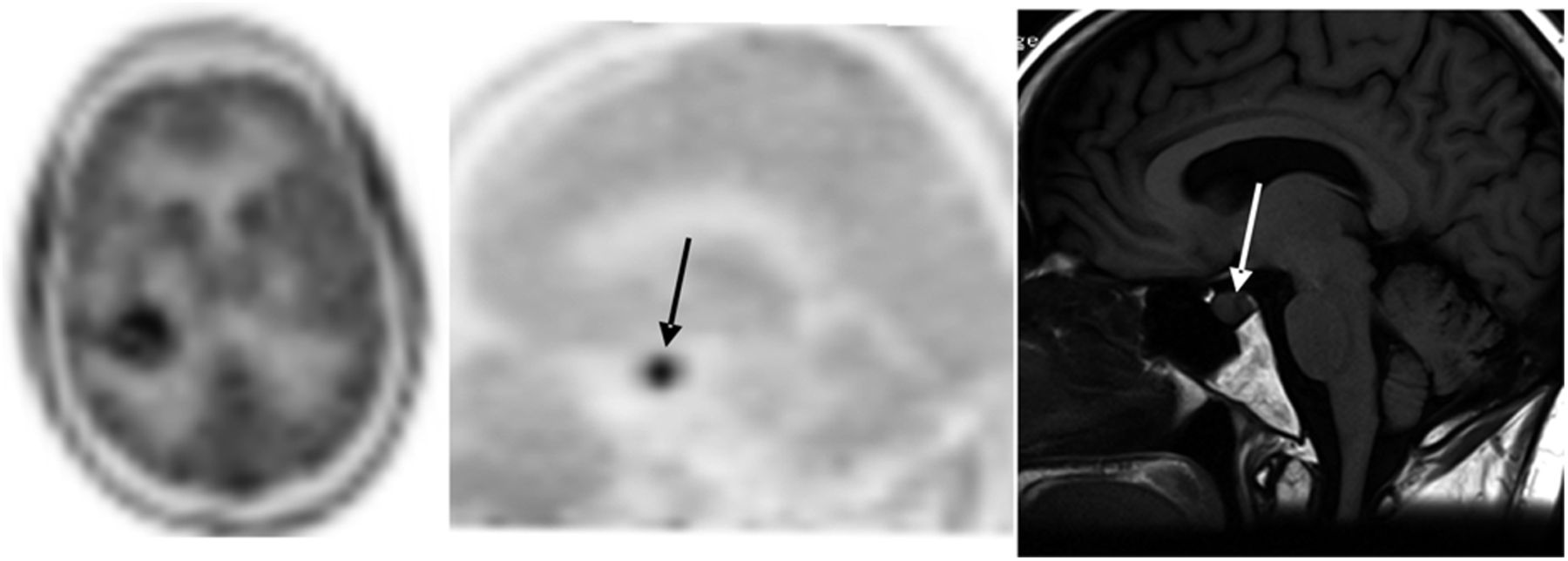
Cerebral PET imaging was performed after intravenous administration of 256 MBq of 18F-FET and a 30-min uptake period in a quiet, dark room. Low-dose CT was acquired for attenuation correction and lesion localization. Moderate 18F-FET accumulation was noted in the inferomedial aspect of the rim-enhancing right parietal lesion (SUVmax, 3.0) (Fig. 3). The mass in the right parietal lobe had central photopenia in keeping with central necrosis. Low-grade uptake was seen elsewhere in the rim of the right parietal lesion. Faint 18F-FET uptake diffusely present throughout the gray matter was thought to be secondary to previous radiation therapy. There was also moderate to intense focal 18F-FET accumulation in the pituitary (SUVmax, 5.8) (Fig. 3). Although moderate physiologic uptake has been reported in the normal pituitary with other amino acid PET tracers (e.g., 11C-methionine), the intensity of accumulation on this study warrants exclusion of an underlying pituitary adenoma or pituitary metastasis. Indeed, based on methionine kinetics, one expects a decline in pituitary accumulation of the tracer from 15 to 30 min after intravenous injection and beyond (5). An absence of this trend is a reliable marker for disease (over normal biodistribution) (5).
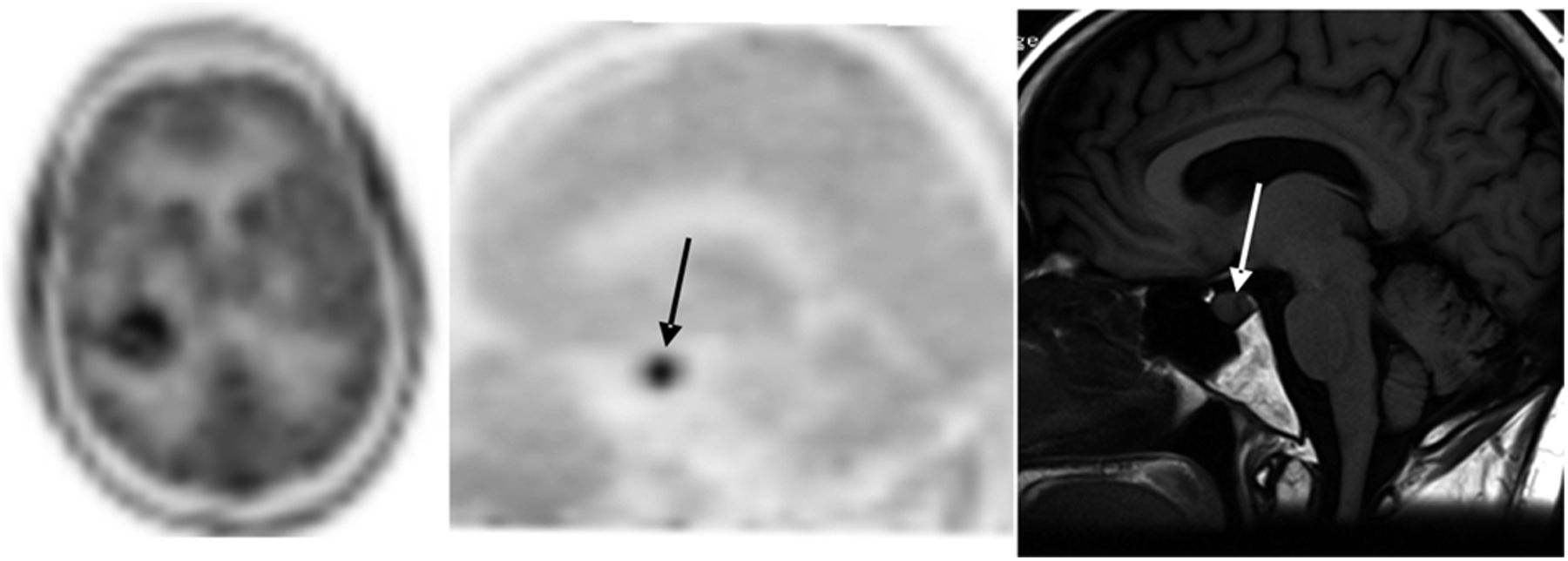
18F-FET PET scan (left) showing enhanced tracer localization in parietal lesion noted on MR imaging and 18F-FDG PET (not shown). Sagittal slices through pituitary demonstrate moderate to intense 18F-FET accumulation (arrow) in pituitary (center) on PET and enlarged pituitary on MR imaging (right).
Axial and sagittal T1-weighted, axial T2-weighted, coronal fluid-attenuated inversion recovery, coronal gradient-recalled echo, axial diffusion-weighted, and postcontrast axial T1 sequences were performed with MR imaging through the whole brain. Coronal and sagittal T1-weighted, coronal T2-weighted, and postcontrast coronal and sagittal T1-weighted sequences were performed through the pituitary fossa. Enlargement of the pituitary gland was noted, measuring up to 1.5 cm in mediolateral dimension and almost 1 cm in coronal dimension (Figs. 3 and 4). There was mild superior surface convexity without suprasellar extension or impingement on the optic nerves or optic chiasm. The T2-weighted coronal sequence demonstrated early lateral encroachment into the cavernous part of the internal carotid artery bilaterally. The infundibulum was deviated just to the right of midline. After intravenous contrast administration, there was relatively heterogeneous enhancement of pituitary tissue. Cavernous carotid flow voids were within normal limits.
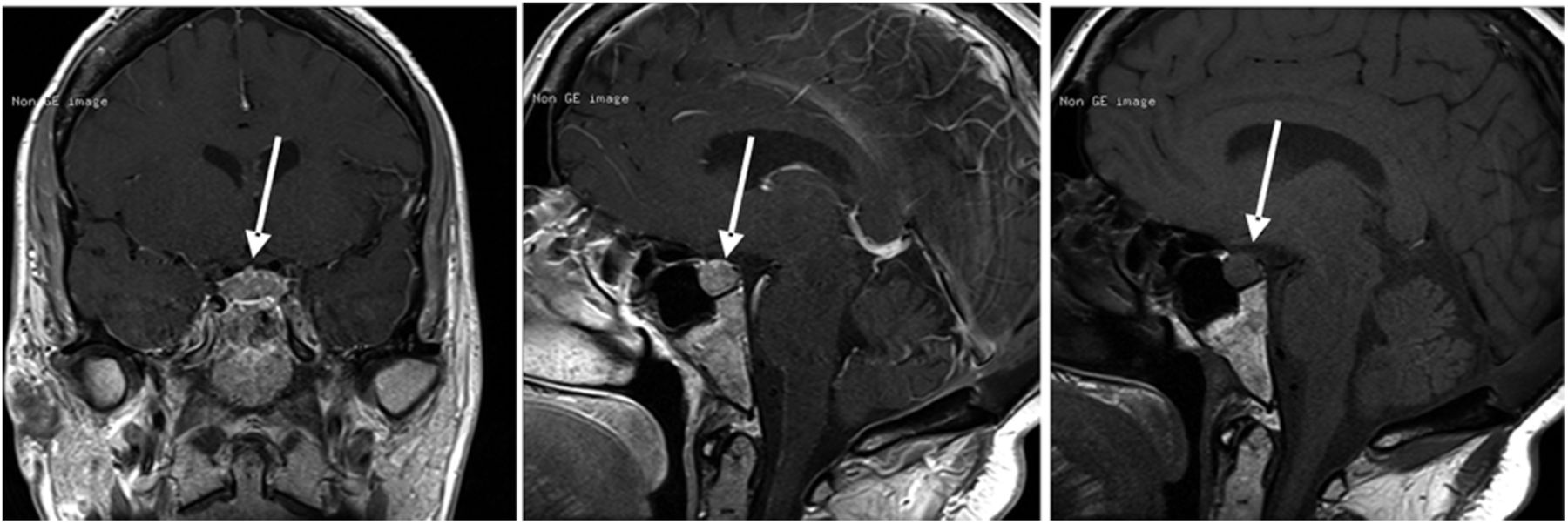
MR imaging slices after (left [coronal view] and center [sagittal view]) and before (right) gadolinium administration showing enlargement and enhancement of pituitary.
Relatively diffuse enlargement of the pituitary gland in a patient with this history may represent metastatic disease in the pituitary; however, skull base CT findings were inconsistent with typical bony destruction associated with pituitary fossa metastasis, and the sella floor cortex appeared intact. A rapidly developing macroadenoma was thought a more likely possibility on CT criteria. Because of the patient’s poor prognosis, a biopsy of the pituitary gland was not considered. Unfortunately, the patient passed away without further follow-up or autopsy.
DISCUSSION
Radiolabeled amino acids have been used widely in molecular imaging and have been found to be of particular benefit in the assessment of brain tumors because of their high amino acid metabolism (4). Historically, PET imaging has been undertaken with [methyl-11C]-l-methionine (11C-MET), but this tracer is limited by the short half-life (20 min) of 11C (4,6). The move to 18F-FET capitalizes on the longer half-life (110 min) and lack of requirement for an onsite cyclotron. 18F-FET uptake is mediated by both sodium-independent and sodium-dependent transport systems (4). As an artificial amino acid, 18F-FET is not incorporated into proteins themselves (unlike 11C-MET) (7–9). The biochemistry is complex; however, amino acid transport systems are typically either sodium-dependent or sodium-independent (10). Of the various sodium-dependent systems, system A is upregulated in some types of cancer such as hepatocellular carcinoma (10,11). For the various sodium-independent systems, system L is upregulated for aromatic and branch-chain amino acids in some types of cancer such as brain tumors (10). The short half-lives of PET tracers are prohibitive of imaging protein synthesis, anabolic processes, or catabolic processes, and thus, both 11C-MET and 18F-FET represent an evaluation of amino acid transport (10). Consequently, tumor uptake tends to be similar for both amino acids and analogs thereof. Amino acid analogs in PET tend to be l-tyrosine in nature, including 18F-FET. Both L and A amino acid upregulation occurs independently of vascular permeability, phase of the cell cycle, and integrity of the blood–brain barrier (11).
When compared with 11C-MET and 18F-FDG, 18F-FET demonstrates much lower uptake in nonneoplastic cells, including inflammatory cells (6,12). This characteristic makes 18F-FET particularly useful in differentiating tumor from posttherapy inflammation and scarring (7,13). Moreover, unlike 18F-FDG, which suffers from confounding from high tracer uptake in normal surrounding brain tissue, 18F-FET demonstrates good contrast in both high-grade and low-grade tumors (6,7,14). Like the patient in this case study, there is a growing demand for 18F-FET imaging because improved therapies mean patients live long enough to first develop brain metastases and secondly be treated for recurrent ones (6,15). Although MR imaging is the preferred modality for assessment of brain metastases, differentiating recurrence from radiation necrosis after therapy can be problematic (6). PET imaging with 18F-FDG has been reported to have variable accuracy for this indication in different studies (6). This limitation is highlighted by a study that reported that 18F-FDG PET after γ-knife therapy could not differentiate viable brain from radiation necrosis (16). Indeed, this limitation is the premise of dual-phase 18F-FDG imaging. Clearly, dual-phase imaging presents several barriers (e.g., time, dose, and decay) that have led to the emergence of 18F-FET in clinical practice as a problem-solving tracer.
18F-FET has been used to differentiate pituitary metastases from more benign pathology (1). When sequential MR imaging has demonstrated regression, stable disease without growth, or slow continuous growth of incidental brain findings, the 18F-FET study has always been negative. Sudden or rapid growth of incidental brain findings on MR imaging, on the other hand, has always been associated with positive findings on 18F-FET PET. Moreover, no patient with diffuse, positive 18F-FET PET findings has been shown to have a benign disease course, whereas diffuse growth on MR imaging in the presence of positive 18F-FET PET findings has been strongly predictive of a malignant course. These observations are consistent with our patient’s having breast cancer metastases in the pituitary rather than adenoma.
Pituitary adenomas are a common (4%–20% of brain studies) incidental finding on CT and MR imaging (1,2). A large study of 13,145 consecutive subjects undergoing 18F-FDG PET revealed a 0.8% incidence of incidental pituitary neoplasia, with 90% of those with a confirmed tumor type having adenoma (3). These results differed substantially from a similar study of 40,967 subjects undergoing 18F-FDG PET, with only 0.07% showing incidental pituitary findings (2). Although these observations have little bearing on this case, they do highlight how uncommon incidental findings in the pituitary are on 18F-FDG PET studies. Nonetheless, the differences in actual incidence may reflect differences in the criteria used and variations in the cross-section of cancer patients included in the studies, with a higher incidence expected when a greater number of cancers known to more commonly metastasize to the pituitary (e.g., breast and lung) are included.
Pituitary metastases, first described in 1857 (15), are a rare complication generally associated with advanced disease in cancer patients (15,17,18). The literature is mixed; however, on the basis of autopsy, it is generally reported that 1%–3.6% of cancer patients have pituitary metastases (17,19,20). Pituitary metastases represent only 1% of all pituitary lesions, but the percentage of all brain metastases represented by pituitary metastases has been reported to be as high as 28% (15,18). In women, breast cancer is the most common tumor to metastasize to the pituitary, and for men it is lung cancer (15,17,20,21), with 20%–30% of pituitary metastases linked to breast cancer and 30%–50% to lung cancer (18). A large series of 380 cases showed that 40% of metastatic pituitary disease arose from breast cancer and 24% from lung cancer (15). For breast cancer, it is thought that the hormone-rich pituitary gland offers favorable conditions for metastatic disease (enhanced proliferation), resulting in pituitary metastases in as many as 29% of breast cancer patients (15,22–26). Pituitary metastases are more common in the posterior lobe than in the anterior lobe (85% vs. 15%) (15,17), because there is direct hematogenous spread to the posterior lobe via hypophyseal arteries whereas the anterior lobe is supplied via a portal supply (no arterial supply) (15). Pituitary metastasis has several recognized pathways, including direct hematogenous spread (posterior lobe), secondary spread via portal vessels from metastases in other structures, extension of local metastases in the skull base, spread through the meninges, and contiguous spread (from posterior to anterior lobes) (15).
In this case, known breast cancer with cerebral metastases and widespread skeletal metastases raised the possibility of hematogenous spread to the posterior lobe with contiguous spread into the anterior pituitary.
Pituitary metastases are associated with symptoms in 2.5%–18.2% of patients at the time of detection by various imaging techniques (15,18). That is, either the symptoms are clinically silent, or end-stage cancer status does not afford sufficient time for symptoms to evolve, or the symptoms are diluted in the morbidity of cancer treatment and survival (15). Diabetes insipidus and its associated symptoms are the most common clinical manifestation associated with pituitary metastases, evident in 45%–70% of patients. In contrast, diabetes insipidus is rare (1%) in pituitary adenoma (15,18,20,27). Although not definitive, the lack of a history of diabetes insipidus in our patient points to a diagnosis of pituitary adenoma.
Antemortem differentiation of pituitary adenoma from metastases is difficult (15,17). CT and MR imaging are generally not specific (15,18,28), and a definitive diagnosis based on histologic evaluation (29) may be undesirable. Although pituitary metastases can mimic benign and malignant sellar lesions, pituitary adenoma is the notable differential (15). Nonetheless, the presence of coexisting brain metastases is a strong indicator that an incidental pituitary lesion is also metastatic, although only 17% of pituitary metastases have coexisting brain metastases (15). The key relationship, however, is that in a patient such as ours, with a history of previous and recurrent brain metastases, an incidental finding of pituitary disease is consistent with metastatic disease (over adenoma). However, pituitary metastases and adenoma can histologically coexist (15).
The treatment of metastatic pituitary disease is generally palliative but may vary depending on the patient’s symptoms and is, therefore, related to symptom relief rather than survival (17,20). In all patients, prognosis is poor, with a life expectancy of a few months after diagnosis (15,20) and mean survival on the order of 6–7 mo (15,30). The rapid decline to mortality in this patient after discovery of pituitary disease is consistent with the course of metastatic disease.
CONCLUSION
Although incidental observation of 18F-FDG accumulation in the pituitary is not unique, the incidental reporting of pituitary accumulation on 18F-FET is, to our knowledge, a first in the literature. This case provides insight into the potential benefits of 18F-FET over both 18F-FDG and anatomic imaging in the assessment of suspected disease recurrence after brain metastases. Although the circumstances in our case were prohibitive of confirmatory investigation with biopsy or autopsy, imaging series provided valuable data to support a high likelihood of pituitary metastases. The history of breast cancer with known widespread metastatic spread to the skeleton, known brain metastases with recurrence after treatment, an incremental increase in 18F-FET localization compared with 18F-FDG, and rapid growth on MR imaging represent findings suggestive of pituitary metastases. The case represents an uncommon finding on MR imaging and on 18F-FDG PET and a rare finding on 18F-FET PET.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 19, 2014.
REFERENCES
- Received for publication December 12, 2013.
- Accepted for publication March 17, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}