


Abstract
The aim of this study was to investigate the potential of O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) PET for differentiating local recurrent brain metastasis from radiation necrosis after radiation therapy because the use of contrast-enhanced MRI for this issue is often difficult. Methods: Thirty-one patients (mean age ± SD, 53 ± 11 y) with single or multiple contrast-enhancing brain lesions (n = 40) on MRI after radiation therapy of brain metastases were investigated with dynamic 18F-FET PET. Maximum and mean tumor-to-brain ratios (TBRmax and TBRmean, respectively; 20–40 min after injection) of 18F-FET uptake were determined. Time–activity curves were generated, and the time to peak (TTP) was calculated. Furthermore, time–activity curves of each lesion were assigned to one of the following curve patterns: (I) constantly increasing 18F-FET uptake, (II) 18F-FET uptake peaking early (TTP ≤ 20 min) followed by a plateau, and (III) 18F-FET uptake peaking early (TTP ≤ 20 min) followed by a constant descent. The diagnostic accuracy of the TBRmax and TBRmean of 18F-FET uptake and the curve patterns for the correct identification of recurrent brain metastasis were evaluated by receiver-operating-characteristic analyses or Fisher exact test for 2 × 2 contingency tables using subsequent histologic analysis (11 lesions in 11 patients) or clinical course and MRI findings (29 lesions in 20 patients) as reference. Results: Both TBRmax and TBRmean were significantly higher in patients with recurrent metastasis (n = 19) than in patients with radiation necrosis (n = 21) (TBRmax, 3.2 ± 0.9 vs. 2.3 ± 0.5, P < 0.001; TBRmean, 2.1 ± 0.4 vs. 1.8 ± 0.2, P < 0.001). The diagnostic accuracy of 18F-FET PET for the correct identification of recurrent brain metastases reached 78% using TBRmax (area under the ROC curve [AUC], 0.822 ± 0.07; sensitivity, 79%; specificity, 76%; cutoff, 2.55; P = 0.001), 83% using TBRmean (AUC, 0.851 ± 0.07; sensitivity, 74%; specificity, 90%; cutoff, 1.95; P < 0.001), and 92% for curve patterns II and III versus curve pattern I (sensitivity, 84%; specificity, 100%; P < 0.0001). The highest accuracy (93%) to diagnose local recurrent metastasis was obtained when both a TBRmean greater than 1.9 and curve pattern II or III were present (AUC, 0.959 ± 0.03; sensitivity, 95%; specificity, 91%; P < 0.001). Conclusion: Our findings suggest that the combined evaluation of the TBRmean of 18F-FET uptake and the pattern of the time–activity curve can differentiate local brain metastasis recurrence from radionecrosis with high accuracy. 18F-FET PET may thus contribute significantly to the management of patients with brain metastases.
- radiation necrosis
- stereotactic radiosurgery
- recurrent brain metastasis
- amino acid PET
- 18F-fluoroethyl-L-tyrosine (18F-FET)
The improvement in the treatment of solid tumors has led to an increasing number of patients who experience brain metastases during the course of the disease. Stereotactic radiosurgery (SRS) and whole-brain radiation therapy (WBRT) are commonly used to treat brain metastases, and a growing percentage of patients live long enough to experience a local relapse of these metastases. Thus, the number of patients experiencing local recurrence of previously irradiated brain metastases can be expected to increase. Contrast-enhanced MRI is the method of choice for the evaluation of metastatic brain tumors. However, in many patients, the differentiation of local recurrent brain metastasis from radiation necrosis after radiotherapy (e.g., SRS or WBRT) using contrast-enhanced MRI is difficult (1). This problem necessitates novel diagnostic methods for the follow-up and management of patients with recurrent brain metastases.
In addition to MRI, PET using 18F-FDG (2) has been considered for the evaluation of metastatic brain tumors, but the high physiologic glucose consumption of the brain and the variable glucose uptake of metastatic brain lesions limit its use. For example, in a study of 48 patients with lung cancer and brain metastasis, 33% of the brain lesions showed hypometabolism on 18F-FDG PET, although all primary lung lesions were hypermetabolic (3). Another study demonstrated that after SRS using a γ-knife, 18F-FDG PET is not sensitive enough to differentiate viable brain metastases from radiation necrosis (4). A recent study, however, indicated that dual-phase imaging may improve the diagnostic accuracy of 18F-FDG PET for the differentiation of recurrent brain metastasis from radiation necrosis (5). A limitation of that approach is the long time interval between PET scans (2–5.7 h). Therefore, alternative imaging methods are still of great interest.
Amino acid tracers are particularly useful for PET in neurooncology because of a high amino acid uptake in tumor tissue together with low uptake in normal brain tissue, resulting in an enhanced tumor–to–normal tissue contrast. Previously, it has been shown that PET using l-[methyl-11C]methionine (11C-MET) may be effective in differentiating recurrent metastatic brain tumor from radiation-induced changes with a sensitivity of 78% and a specificity of 100%, respectively (6). In a subsequent study (7) with a larger number of patients (n = 51), these findings could be confirmed, at least in part, with similar sensitivity (79%) but with lower specificity (75%). The use of 11C-MET, however, remains restricted to centers with an on-site cyclotron because of the short half-life of the 11C isotope (20 min). In contrast, amino acids labeled with 18F (half-life, 110 min) such as O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) allow a more widespread use and can be distributed via the satellite concept as has been shown with the widely used 18F-FDG (8–11). Several studies have demonstrated the clinical utility of 18F-FET PET, especially in the diagnostics and therapy assessment of cerebral gliomas (12–14). The tracer exhibits high in vivo stability, low uptake in inflammatory tissue, and suitable uptake kinetics for clinical imaging (15–17). Contrast-enhancing nontumoral tissue on MRI, for example, due to radionecrosis, is usually negative on 18F-FET PET (14). Furthermore, 18F-FET uptake kinetics have been shown to provide valuable information for the differentiation of high-grade from low-grade gliomas and treatment-related changes in the brain tissue (8,16–19). In contrast, the role of 18F-FET PET in the diagnostics and therapy assessment of cerebral metastases is not yet established, and only a few studies have reported on increased 18F-FET uptake in cerebral metastases (20,21).
Accordingly, here we evaluated the clinical usefulness of 18F-FET PET for the differentiation of local recurrent brain metastasis from radiation necrosis.
MATERIALS AND METHODS
Patients
Thirty-one patients with metastatic brain tumors (mean age ± SD, 53 ± 11 y; age range, 17–70 y; 26 women and 5 men), each with at least 1 contrast-enhancing lesion (n = 40) on cerebral MRI, were included in the study (Table 1). The patients were consecutively sent from 2005 to 2011 to our institute because of suggestive MRI findings such as newly contrast-enhancing lesions or progression of contrast enhancement at the site of the initial metastasis, in order to differentiate local recurrent brain metastasis from radiation necrosis using 18F-FET PET. All patients had been previously treated with SRS (range of radiation dose, 8–25 Gy) and partly with WBRT (range of radiation dose, 20–30 Gy). The median interval between radiotherapy and PET was 11.5 mo. All patients gave written informed consent to the PET investigation.
Patient Characteristics
Histopathologic results for definite diagnosis were available for 11 patients (11 lesions). For the remaining patients, diagnosis of recurrent brain metastasis or radiation necrosis was based on the clinical course and results of MRI in the further follow-ups. Recurrent disease was anticipated if a new contrast-enhancing lesion appeared at exactly the same site as the treated metastasis after initial complete response, if the treated metastasis grew during follow-up according to the Macdonald criteria (22) (increase of >25% in the pretreated volume on contrast-enhanced T1-weighted MR images), or if new neurologic deficits or an exacerbation of existing neurologic symptoms occurred. Radiation necrosis or unspecific posttherapeutic changes in the tissue were assumed when the lesions showed spontaneous shrinkage or remained stable in size on contrast-enhanced MRI after a long-term follow-up (median time, 12 mo) and neurologic deficits remained unchanged or no new neurologic symptoms occurred.
PET with 18F-FET and Data Analysis
The amino acid 18F-FET was produced via nucleophilic 18F-fluorination with a specific radioactivity of greater than 200 GBq/μmol as described previously (11). The radiochemical yield of tracer was about 60%–65% at a radiochemical purity greater than 98%. The tracer was administered as isotonic neutral solution. According to the German guidelines for brain tumor imaging using labeled amino acid analogs, all patients fasted for at least 12 h before PET (23). Dynamic PET studies were acquired up to 50 min after intravenous injection of approximately 200 MBq of 18F-FET on an ECAT EXACT HR+ scanner (Siemens Medical Systems, Inc.) in 3-dimensional mode (32 rings; axial field of view, 15.5 cm). The emission recording consisted of 16 time frames (1–5, 1 min; 6–10, 3 min; and 11–16, 5 min) covering the period up to 50 min after injection. For attenuation correction, transmission was measured with three 68Ge/68Ga rotating line sources. After correction for random and scattered coincidences and dead time, image data were obtained by filtered backprojection in Fourier space using the ECAT 7.2 software. The reconstructed image resolution was approximately 5.5 mm.
18F-FET uptake in the tissue was expressed as standardized uptake value (SUV) by dividing the radioactivity (kBq/mL) in the tissue by the radioactivity injected per gram of body weight.
18F-FET PET and contrast-enhanced MRI were coregistered using MPI tool software (version 6.48; ATV). The fusion results were inspected and, if necessary, adapted using anatomic landmarks. The region-of-interest (ROI) analysis was based on the summed PET data from 20 to 40 min after injection (23). The transaxial slices showing the highest 18F-FET accumulation in the tumors were chosen for ROI analyses. 18F-FET uptake in the unaffected brain tissue was determined by a larger ROI placed on the contralateral hemisphere in an area of normal-appearing brain tissue including white and gray matter (mean area ± SD, 1,651 ± 496 mm2) (23). 18F-FET uptake in the tumor (tumor ROI) was determined by a 2-dimensional auto-contouring process using a tumor-to-brain ratio (TBR) of 1.6 or more. This cutoff is based on a biopsy-controlled study of cerebral gliomas in which a lesion-to-brain ratio of 1.6 best separated tumoral from peritumoral tissue (24). Furthermore, we determined the longest diameter of contrast enhancement on MRI and of 18F-FET uptake (longest diameter of the tumor ROI) and the area of the tumor ROI (mm2) on 18F-FET PET scans.
Mean and maximum TBR (TBRmean and TBRmax, respectively) were calculated by dividing the mean and maximum SUV of the tumor ROI by the mean SUV of normal brain in the 18F-FET PET scan. Time–activity curves were generated by application of the ROIs of the lesions (20–40 min) to the entire dynamic dataset. Time to peak (TTP; time in minutes from the beginning of the dynamic acquisition up to the maximum SUV of the lesion) was determined. Furthermore, the time–activity curves of each lesion were assigned to one of the following curve patterns: (I) constantly increasing 18F-FET uptake without identifiable peak uptake, (II) 18F-FET uptake peaking early (TTP ≤ 20 min) followed by a plateau, and (III) 18F-FET uptake peaking early (TTP ≤ 20 min) followed by a constant descent.
Statistical Analyses
Descriptive statistics are provided as mean and SD or as median and range. To compare 2 groups, the Student t test was used. The Mann–Whitney rank-sum test was used when variables were not normally distributed. P values of less than 0.05 were considered significant. The diagnostic performance of TBR values to differentiate local recurrent brain metastasis from radiation necrosis was assessed by receiver-operating-characteristic (ROC) curve analyses using the results of histopathology or of the clinical course as reference. The diagnostic performance of curve patterns alone to differentiate local recurrent brain metastasis from radiation necrosis was evaluated by Fisher exact test for 2 × 2 contingency tables.
For the combined ROC analysis of TBRmean and curve patterns, patient data were assigned to 1 of 3 categories: recurrent metastasis unlikely (TBRmean < optimal cutoff in ROC analysis and curve pattern I), recurrent metastasis suspected (TBRmean > optimal cutoff or curve pattern II or III), or recurrent metastasis highly probable (TBRmean > optimal cutoff and curve pattern II or III).
For ROC analyses of TBR values, decision cutoff was considered optimal when the product of paired values for sensitivity and specificity reached its maximum. In addition, the area under the ROC curve (AUC), its SE, and level of significance were determined as a measure of diagnostic quality. Statistical analysis was performed using SigmaPlot software (version 11.0; Systat Software Inc.) and PASW statistics software (release 18.0.3; SPSS Inc.).
RESULTS
Surgical intervention was performed in 11 patients with single lesions, and histopathology showed viable tumor tissue in 6 patients and necrosis with no viable tumor cells in 5 patients. Sixteen lesions in 12 patients without histologic evaluation were classified as radiation necrosis because the patients exhibited stable neurologic symptoms and no significant enlargement of the lesion was observed on follow-up MR images after a median of 12 mo. Because of clinical deterioration of neurologic symptoms or progression in size on contrast-enhanced MRI during follow-up, 13 lesions in 8 patients were classified as recurrent brain metastases (Table 1).
Comparison of Uptake Indices for Recurrent Brain Metastasis and Radiation Necrosis
The TBRmax and TBRmean were significantly higher in patients with recurrent metastases (n = 19) than in patients with radiation necrosis (n = 21) (TBRmax, 3.2 ± 0.9 vs. 2.3 ± 0.5, P < 0.001; TBRmean, 2.1 ± 0.4 vs. 1.8 ± 0.2, P < 0.001). No significant size differences between radiation-induced lesions and recurrent metastases (median area of the tumor ROI, 230 vs. 404 mm2; P = 0.16) could be observed. The smallest lesion size on 18F-FET PET was 6 mm (range of longest diameter of tumor ROIs, 6–51 mm).
ROC Analysis of TBR Values
The diagnostic accuracy of 18F-FET PET TBR values for the correct identification of recurrent brain metastases reached 78% using TBRmax (AUC, 0.822 ± 0.07; sensitivity, 79%; specificity, 76%; cutoff, 2.55; P = 0.001) and 83% using TBRmean (AUC, 0.851 ± 0.07; sensitivity, 74%; specificity, 90%; cutoff, 1.95; P < 0.001) (Table 2).
Results of Diagnostic Performance
Evaluation of Curve Patterns
In 31 patients, time–activity curves of 40 lesions were assessed. Two lesions were present in 4 patients (patients 16, 17, 22, and 31), 3 lesions in 1 patient (patient 27), and 4 lesions in 1 patient (patient 23) (Table 1). Time–activity curve pattern I (Fig. 1, patient 24) was found in 24 lesions (60%) of 21 patients, pattern II (Fig. 1, patient 12) in 10 lesions (25%) of 9 patients, and pattern III (Fig. 1, patient 9) in 6 lesions (15%) of 4 patients (Table 1). A preliminary analysis of our dataset revealed that kinetic pattern type I occurred mainly in lesions that had been caused by radiation necrosis whereas patterns II and III were typical of recurrent brain metastasis. The diagnostic accuracy was 92% for curve patterns II and III versus curve pattern I (sensitivity, 84%; specificity, 100%; P < 0.0001).
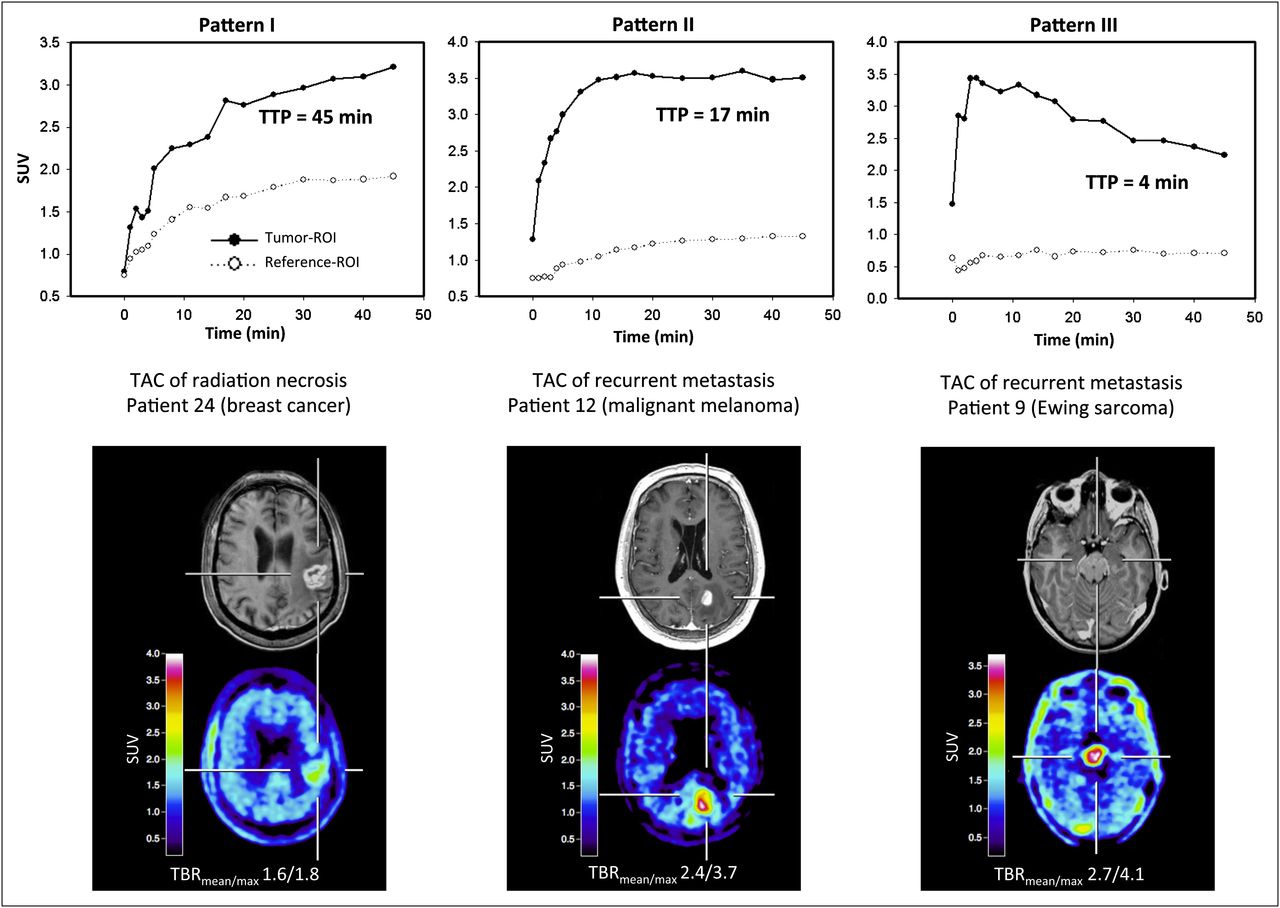
Examples of kinetics of radiation necrosis (pattern I) and recurrent brain metastasis (patterns II and III). All studies show pathologic contrast enhancement on T1-weighted MRI (minimal enhancement in patient 9) and corresponding increased 18F-FET uptake (TBRmean and TBRmax values are given below PET images). Dynamic evaluation of patient 24 (58-y-old woman 32 mo after SRS [brain metastasis of breast cancer, ductal carcinoma]) shows constantly increasing 18F-FET uptake until end of acquisition. TTP is 45 min. Diagnosis of radiation necrosis was based on clinical course. Dynamic evaluation of patient 12 (50-y-old man 16 mo after SRS [brain metastasis of malignant melanoma]) shows early peak of 18F-FET uptake (TTP = 17 min) followed by stable uptake until end of acquisition. Diagnosis of brain metastasis was based on clinical course. Dynamic evaluation of patient 9 (17-y-old girl, MRI findings and clinical course suggestive of first manifestation of metastatic brain tumor) shows early peak of 18F-FET uptake after 4 min followed by constant decline of uptake until end of acquisition. Diagnosis of brain metastasis was confirmed histopathologically (Ewing sarcoma). TAC = time–activity curve.
Combined ROC Analysis of TBRmean and Curve Pattern
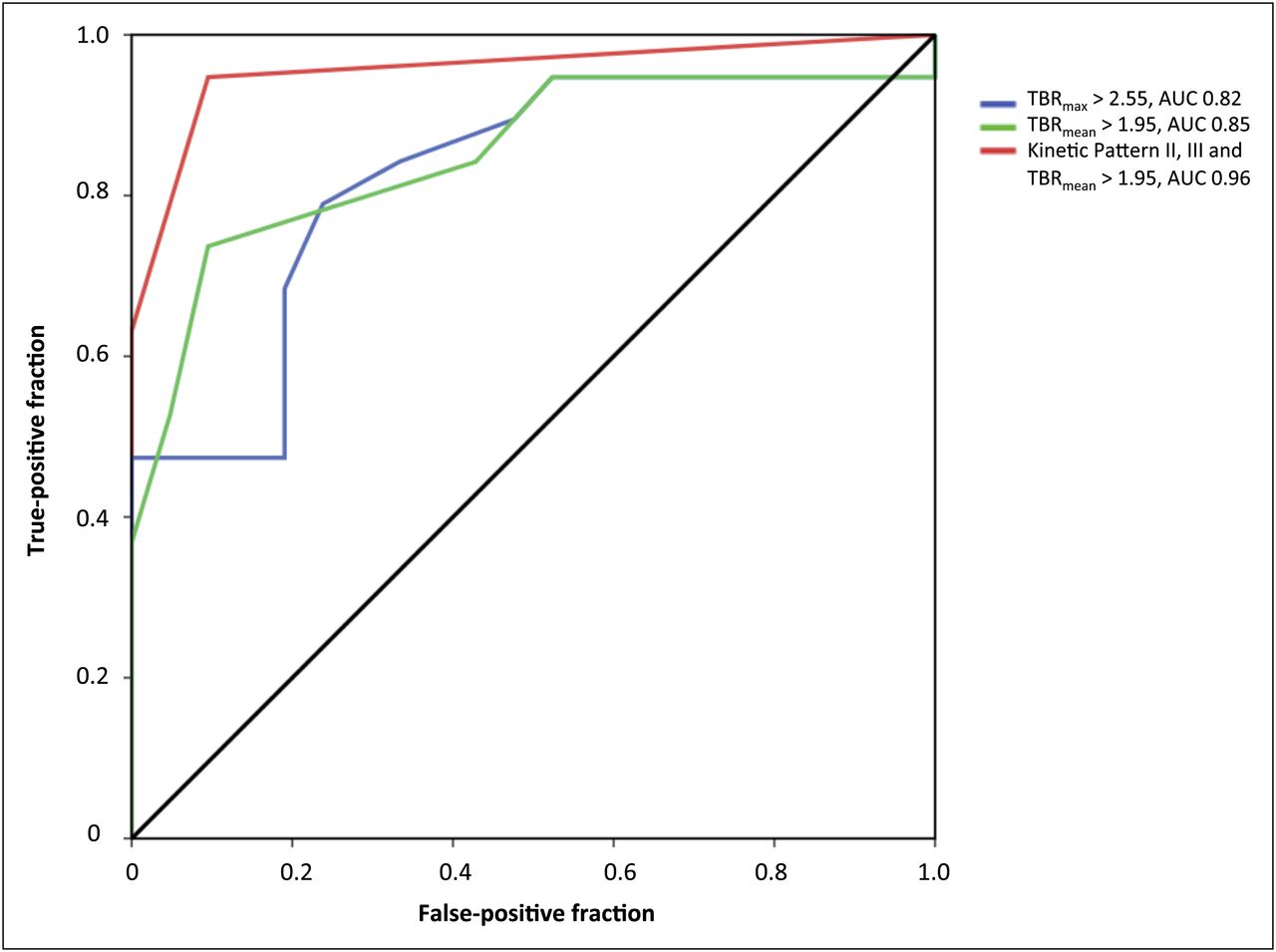
The highest accuracy (93%) in diagnosing recurrent metastasis was obtained when both the TBRmean was greater than 1.9 and the curve pattern was II or III (AUC, 0.959 ± 0.03; sensitivity, 95%; specificity, 91%; P < 0.001) (Table 2). Figure 2 shows the ROC curves for the TBRmax, TBRmean, and combined use of TBRmean and curve pattern for differentiation of local recurrent brain metastasis from radiation necrosis.

ROC curves for TBRmax, TBRmean, and combined use of TBRmean and curve pattern for metastatic brain tumors. AUC was 0.82 for TBRmax (blue line; optimal threshold > 2.55), 0.85 for TBRmean (green line; optimal threshold > 1.95), and 0.96 for combination of kinetic patterns II and III and TBRmean > 1.95 (red line).
DISCUSSION
Cerebral metastases affect 20%–30% of all cancer patients and are the second most common form of cerebral neoplasm in adults. Today, the use of SRS is a widely accepted treatment option for cerebral metastases (25), either as a single modality or in combination with WBRT. Radiation-induced changes (i.e., radiation necrosis) on follow-up MRI studies including alterations in T2-weighted images and changing patterns of contrast enhancement have been reported in about 20% of all patients and can often not be distinguished from local tumor recurrence (26–28). The current gold standard for distinguishing tumor recurrence from radiation necrosis remains biopsy, which has an accuracy of more than 95% (29,30). Biopsy, however, is invasive and has potential complications such as infection, procedure-associated new neurologic problems, and hematoma, although the risk of permanent complications is relatively low (29,30). Therefore, a noninvasive imaging technique is desirable to derive valuable additional information.
As outlined here, the use of standard 18F-FDG PET for the differentiation of tumor recurrence from radiation necrosis is unsatisfactory (3,4) but may be improved by dual-phase imaging (5). Differentiation using 11C-MET PET could be achieved at a TBRmean threshold of 1.41, with a sensitivity and specificity of 75% and 78%, respectively (7). Although this result is better than the performance of standard 18F-FDG PET, it may still not be sufficient for clinical decision making. In the present study, we observed at a cutoff TBRmean of 1.95 with 18F-FET PET a similar sensitivity (74%) and improved specificity (90%). When our data are compared with the results using 11C-MET PET (7), different cutoff values may be explained by methodologic differences in the generation of ROIs for the tumor and the background area. Another cause may be differences in the metabolic properties of the 2 different amino acids. Thus, 18F-FET PET, compared with 11C-MET PET, shows not only considerable logistic advantages but also improved accuracy in differentiating local recurrent brain metastasis from radionecrosis.
In addition to the diagnostic value of the TBR of 18F-FET uptake, several studies have shown that the evaluation of 18F-FET kinetics may add relevant diagnostic information, especially for noninvasive tumor grading and the differentiation of recurrent high-grade glioma from radiation necrosis (8,16–19). Time–activity curves of high-grade gliomas are characterized by an early peak of 18F-FET uptake followed by a constant descent, whereas low-grade gliomas and benign brain lesions typically show a steadily increasing curve pattern. In contrast, 11C-MET PET studies showed no different curve patterns in high- and low-grade gliomas (31).
To explore the putative impact of 18F-FET kinetics, we analyzed time–activity curve patterns of 18F-FET uptake in recurrent metastasis and radiation necrosis. A preliminary evaluation indicated that radiation necroses typically showed a steadily increasing curve pattern as previously reported for low-grade gliomas or benign posttherapeutic changes (curve pattern I), whereas curve patterns in recurrent metastases typically showed an early peak of 18F-FET uptake followed by either a plateau (curve pattern II) or a constant descent (curve pattern III). Differentiation of local recurrent metastasis from radiation necrosis could be achieved with a sensitivity and specificity of 84% and 100%, respectively, when these different curve patterns were used as a diagnostic parameter. The highest accuracy in diagnosing recurrent metastases was obtained when both a pathologic TBRmean and a type II or III curve pattern was present.
To the best of our knowledge, this is the first study exploring the usefulness of dynamic 18F-FET PET for the differentiation of local recurrent brain metastasis from radiation necrosis. This approach may achieve an accuracy that is sufficient to influence clinical decision making and may therefore help to reduce the number of invasive diagnostic interventions and overtreatment in a considerable number of seriously ill patients with brain metastases. Limitations may be the relatively long scanning time (50 min), which may cause artifacts due to patient’s head motion. This problem, however, did not occur in our study.
To date, experience with 18F-FET PET in patients with brain metastases is limited, and 18F-FET kinetics in the lesions have not yet been considered (20,21). Grosu et al. (21) reported for patients with confirmed recurrent brain metastases (clinically or through biopsy) after treatment with SRS (n = 9) a mean 18F-FET uptake of 2.1 ± 0.6. In 4 patients with a final diagnosis of radiation injury, the mean 18F-FET uptake was 1.5 ± 0.3. Pichler et al. (20) observed a mean 18F-FET uptake of 2.7 ± 1.8 in 3 patients with histologically confirmed brain metastasis (lung cancer, seminoma, and malignant melanoma). These results are in line with the results of the TBR values in our study and suggest that 18F-FET PET may also be an option for the differentiation of recurrent brain metastases and nonneoplastic lesions.
Several factors may contribute to the different kinetic behaviors in recurrent brain metastasis and radiation necrosis. Weckesser et al. (8) suggested that the higher initial uptake in high-grade gliomas might be due to a higher regional blood volume as a consequence of increased angiogenesis and intratumoral microvessel density in patients with malignant progression (32). Accordingly, angiogenesis has long been established as a key element in the pathophysiology of development and growth of brain metastasis (33). Another explanation (34) may be an upregulation of facilitated amino acid transport, which is responsible for an increased 18F-FET uptake in gliomas (35). An increased expression of sodium-independent L-type amino acid transporters has also been reported for metastatic tumor cells, for example, squamous cell carcinoma and adenocarcinoma (36). Most probably, the tracer kinetics in recurrent brain metastasis and radiation necrosis may be caused by both differences in vascularity and a differential expression of amino acid transporters that influence tracer influx and efflux. That both factors are likely to contribute to different kinetic patterns in brain metastasis is further supported by the finding that amino acid uptake has been shown to correlate with vascular density and microvessel density (37,38). In addition, SRS-induced effects (e.g., antiangiogenic effect) resulted in a change of the kinetic pattern (Fig. 3).

In patient 19, with lung cancer, γ-knife SRS of left parietal metastasis induced change in kinetic pattern of 18F-FET uptake. Before SRS, values of TBRmean and TBRmax were 2.0 and 2.8, respectively, and 18F-FET uptake peaked early after 11 min and then stabilized (kinetic pattern II; top). Eleven months after SRS, values of TBRmean and TBRmax declined (1.6 and 1.8, respectively), and 18F-FET uptake pattern constantly increased (pattern I; bottom), indicating treatment response. TTP is 45 min. Sixteen months later, patient was still alive and without clinical signs of tumor recurrence. TAC = time–activity curve.
Although conventional MRI cannot reliably distinguish between recurrent brain metastasis and radiation necrosis, several advanced MRI techniques are presently evaluated that may eventually help to overcome this problem. For example, the value of multivoxel proton magnetic resonance spectroscopic imaging and dynamic susceptibility-weighted contrast-enhanced perfusion MRI has been successfully investigated (39,40). From both the patients’ and the clinicians’ perspective, the results are promising, but the clinical relevance of these methods is not yet established. These developments are, however, encouraging, and comparative studies are needed to investigate the relationship, diagnostic performance, and complementary character of amino acid PET and modern MRI techniques.
Because of the small sample size, the results of our study should be considered cautiously, and a larger prospective study is needed to confirm the clinical usefulness of 18F-FET PET–derived imaging parameters for differentiating local recurrent brain metastasis from radiation necrosis after radiation therapy.
CONCLUSION
Our findings suggest that the TBRmean and results of kinetic studies in 18F-FET PET can differentiate local recurrent brain metastasis from radiation necrosis with a high sensitivity and specificity. 18F-FET PET may thus contribute significantly to the management of patients with brain metastases.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 7, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 19, 2012.
- Accepted for publication April 2, 2012.





{kind=link}
{kind=link}
{kind=link}