


Abstract
Syringe pumps are commonly used to administer therapeutic 131I-metaiodobenzylguanidine. Here we describe our recent experience with a peristaltic infusion pump system in a pediatric setting. This method can easily accommodate infusions from several vials simultaneously and is adaptable to various types of peristaltic pump. Methods: Simple off-the-shelf components are used to vent the vial: a charcoal filter, a 0.22-μm syringe filter, and a 2.54-cm (1-in) needle. The vial is connected to the primary infusion set using a male/male extension line and a 19-gauge × 8.89-cm (3.5-in) aspirating needle. With aseptic technique, the extension line is attached to the Y connector closest to the primary intravenous line leading from the saline reservoir to the infusion pump. An A-clamp is attached to the primary intravenous line, immediately before the entrance to the pump. Gravity is allowed to clear the air from the extension set and the aspirating needle. After all the air has been purged, the aspirating needle is inserted into the therapy vial using aseptic technique. The pump is programmed with the desired infusion rate and volume to be infused. Results: Twenty-one consecutive infusions have been performed to date using this method. Most of the infusions involved the use of 1 vial. On 7 occasions, 2 or 3 vials connected in series were used to successfully administer the therapy. Overestimation of the volume in the vials or of the total infusion time required can cause air to be pulled into the lines. To prevent this, the volume in the vials is equalized to 30 mL, facilitating calculation of the infusion time. If the infusion is observed over the last 2 or 3 mL and the pump stops when the air–fluid mark is about halfway up the extension set, air will be kept out of the primary infusion set. Conclusion: This method for infusing one or more vials of therapeutic radiopharmaceuticals is robust and easy to use. During infusion, the radiopharmaceutical remains in a shielded vial. Multiple vials can be connected in series to infuse the entire dose simultaneously.
We describe here a method for the administration of 131I-MIBG with a standard peristaltic infusion pump. Although there are other methods that depend on a syringe pump to infuse therapeutic radiopharmaceuticals, the peristaltic infusion pump is versatile, making it easy to perform infusions from several vials simultaneously while the radioisotope remains in its original shielding. This system is also adaptable to different types of peristaltic pumps and infusion sets.
131I-MIBG is an effective therapeutic agent commonly used in treating neuroendocrine malignancies such as neuroblastoma in a dosage range of 222 MBq/kg (6 mCi/kg) to as much as 666 MBq/kg (18 mCi/kg) (1,2). At these ranges, the total infused activity may range from 3.7 GBq (100 mCi) in children to over 44.4 GBq (1,200 mCi) in adults. But handling a high activity of 131I-labeled products poses radiation exposure risks that need to be minimized among team members. In our facility, we use a multidisciplinary approach. The therapy team is composed of members from the medical oncology, radiation oncology, nursing, nuclear medicine, child life, and radiation safety teams, with each providing expertise and perspective that aids in the successful completion of the therapy. Commensurate with their tasks, all team members need to have the appropriate training and experience in managing administration of therapy to patients or using unsealed therapeutic radiopharmaceuticals (3).
Initiating a therapeutic 131I-MIBG program is a complex endeavor that other authors have aptly described (4,5). However, when it comes to the infusion of the 131I-MIBG, other than the mention of a syringe pump, there are no good technical descriptions of how to administer the radiopharmaceutical (6,7). Novices are thus left to develop their own method or arrive at a suitable protocol by trial and error. Our purpose here is to describe the peristaltic infusion pump method for the intravenous administration of 131I-MIBG.
MATERIALS AND METHODS
After considering the available infusion options, we decided to use a modified version of the system described by Yokell et al. (8) and successfully applied in studies by Matthay et al. (9) and Pryma et al. (10). Our decision was based on several factors. First, the method can easily accommodate infusions from multiple vials. Second, the process can be adapted to various types of peristaltic pumps. Third, readily available off-the-shelf components are used to make the various connections. Fourth, the infusion pump system has the potential to minimize radiation exposure during product preparation because the 131I-MIBG does not have to be transferred from the manufacturer’s vial to various syringes. Last, choosing a pump that our hospital uses for routine clinical care helps minimize training because the staff is already familiar with it. Also, the biomedical instrumentation department is already making sure the pumps in use are calibrated and in good working order. When syringe pumps are used, syringes containing the radiopharmaceutical have to be exchanged unshielded out of the syringe pump to complete the administration of the therapeutic infusion, and this unshielded exchange has the potential for increased exposure to medical personnel (11). Minimizing radiation exposure during the infusion is important, as our observations have demonstrated that it is during this part of the procedure that most of the personnel radiation exposure occurs. Turpin et al. (12), though they used a syringe pump, seemed to confirm our observation of a reduction of radiation exposure during infusion. Below, we describe our procedure for administering therapeutic amounts of 131I-MIBG using the peristaltic infusion pump method. With the technique described here, we have successfully infused 21 patients with activity in the range of 10.175–23.125 GBq (275–625 mCi) from up to 3 vials connected in series.
RESULTS
Technical Considerations and Aseptic Technique
Quality control to check for radiolytic decomposition and the final product preparation is performed in a Nuaire LabGard class II type B2 biologic safety cabinet that was modified by Capintec. This cabinet is well shielded for work with high-energy radioisotopes such as 131I and 18F while maintaining aseptic conditions. The maintenance of fume hoods and aseptic conditions is beyond the scope of this paper. Detailed information on this topic has been previously published (13,14).
Preparation
Currently, we use therapeutic 131I-MIBG (Draximage) and perform quality control testing for free 131I using the Accell Plus CM Sep-Pac method (Waters). After thawing, the product can be used if quality control testing yields results showing less than 5% free 131I. After completion of the quality control testing, the volume is standardized to 30 mL with sodium chloride, 0.9% for injection.
To prepare for administration of the therapeutic product, the infusion kit is assembled from the materials listed in Table 1. First, a vial venting unit (Fig. 1) is assembled using the charcoal Sep-Pac filter, the 0.22-μm syringe filter, and a 20-gauge 2.54-cm (1-in)-long needle.
Component List for Therapy Administration System

Vial venting unit.
The charcoal filter helps minimize the venting of free 131I from the preparation. The syringe filter helps keep particulate matter from entering the preparation from the air or charcoal filter. Table 1 has a list of off-the-shelf components available to us to connect the vial with the 131I-MIBG therapeutic product to the infusion pump (Fig. 2). Similar items from other vendors can be substituted but should first be tested for compatibility with each other, the pump, and the primary infusion set.

Connection of vial (single-vial method) to infusion set.
The infusion pump is programmed to the determined flow rate as shown in Table 2. By protocol, the product is extracted from the vials so that the infusion is completed within 120 min. Standardizing the volume in the vials facilitates calculating the infusion rate, and if several vials are to be administered, the infusion rate is based on multiples of 30 mL as shown in Table 2.
Sample Infusion Rates for 131I-MIBG Therapy
Infusion Procedure
Peristaltic infusion pump systems offer a wide variety of safety features such as occlusion alarms and free-flow protection coupled with software that ensures proper programming and other features that enhance safety during the infusion. With the use of this infusion process, better shielding of the radiopharmaceutical is available during the infusion because the product remains sealed in the manufacturer’s vial and is shielded during the entire process. Furthermore, the vial is never pressurized, minimizing leaks at intravenous line connections. Readily available sterile components to connect the vial to the intravenous tubing negate the need to find expensive specialty items. An added benefit is that since infusion pumps are standardized in most institutions, nurses and technical personnel are already familiar with their use. As such, problems with the pump during infusion can easily be identified and resolved.
The therapeutic infusion system includes a venting unit made from a 0.22-μm syringe filter that is attached to the charcoal filter unit and affixed with a 20-gauge 2.54-cm (1-in) needle to the Luer-Lok (Becton-Dickinson) end of the syringe filter. The venting unit is then inserted into the patient dose vial. This venting unit filters air entering the vial, minimizing the entry of dust and microbes. The activated charcoal filter traps free iodine that may leave the vial during the venting process.
After the venting unit is inserted, a 19-gauge 8.89-cm (3.5-in) aspirating needle is attached to a male/male 78.74-cm (31-in) Microbore extension set (Braun). With aseptic technique, the opposite end of the aspirating needle, the Microbore extension, is attached to the Y connector closest to the primary infusion line leading from the saline reservoir to the infusion pump. An A-clamp is attached to the primary infusion line, immediately before the entrance to the pump. Gravity is allowed to clear all the air from the Microbore extension set and the aspirating needle. Afterward, the Microbore extension set is clamped. With aseptic technique, the aspirating needle is inserted at an angle into the therapy vial. The sheath from the aspirating needle is placed under the shield in such a way that the resulting tilt pushes the liquid toward the side where the aspirating needle hits the bottom of the vial.
The pump is programmed with the desired infusion rate and volume (Table 2). Because the volume in the vials has previously been standardized to 30 mL, the volume to be infused is set at 28 mL in order to stop the pump before air gets into the infusion lines. Before the pump is started, the A-clamp on the extension set is removed and closure of the A-clamp above the Y connector on the primary line throughout the infusion is ensured. Once the pump is running, the pressure in the primary tubing and the Microbore extension tube above the infusion pump decreases, pulling the fluid from the radiopharmaceutical vial through the infusion pump, the primary line, and on to the patient. The venting unit maintains ambient pressure in the radiopharmaceutical vial, facilitating the flow of fluid from the vial.
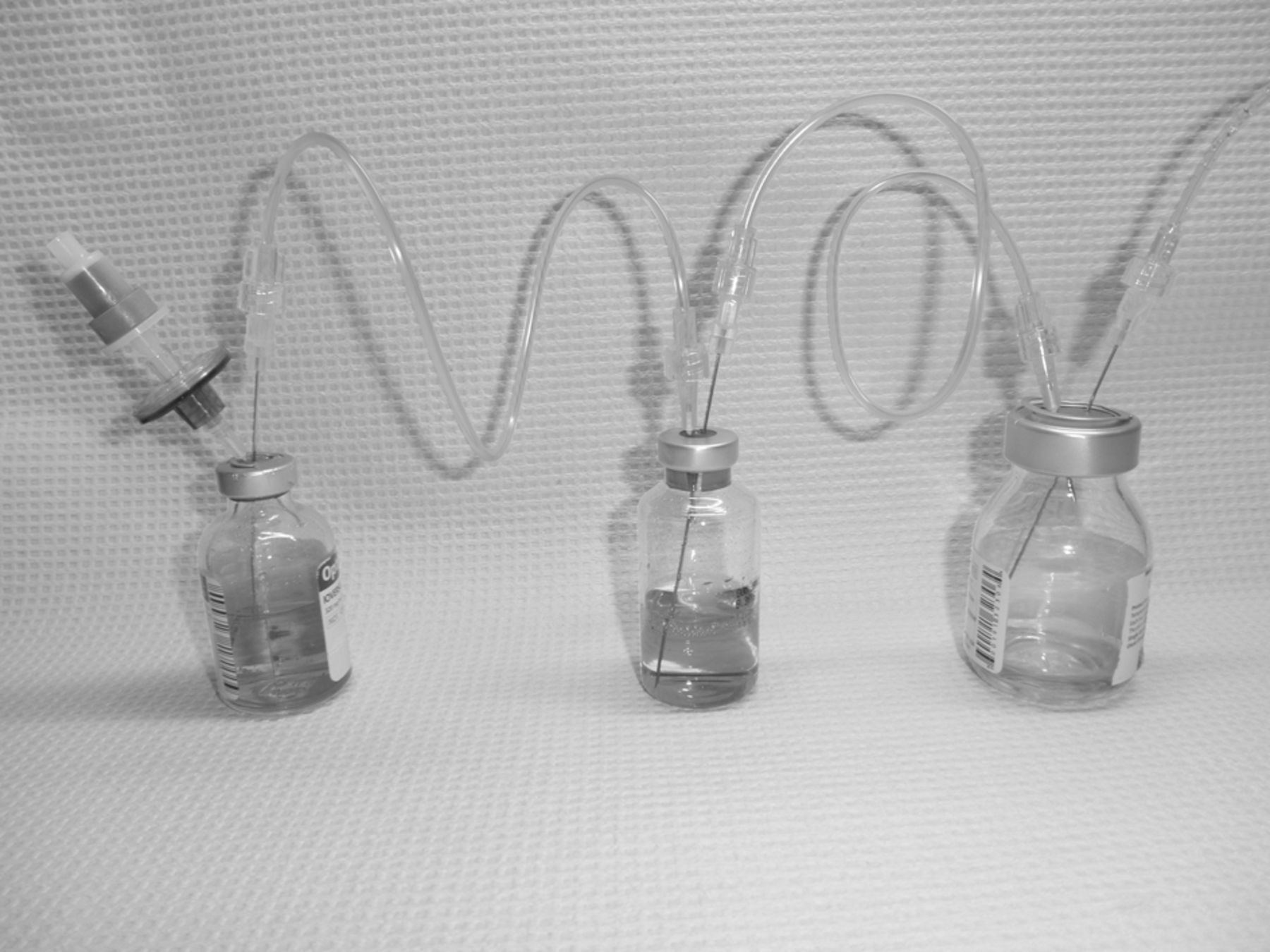
If more than one vial is being administered, connecting them in series (piggyback method) as shown in Figure 3 allows the combined volume to be infused simultaneously. Infusing several vials connected in series minimizes subsequent manipulation of the system and helps reduce radiation exposure to the technical staff. When the pump stops, there should be 2 or 3 mL left in the vial. At that point, adding 10 mL to the vented vial (or the one at the start of the chain if the piggyback method is used) flushes any remaining activity from all the vials. The pump is restarted to deliver the last of the product (the extension line is carefully observed from behind the shield). When the air–fluid mark is about halfway to the end of the 78.74-cm (31-in) extension set tube, the infusion is stopped. With aseptic technique, the extension tube is disconnected from the infusion pump primary set tubing.

Connection of several vials in series (piggyback method).
Once the extension tube has been disconnected, the pump is run at 50 mL/h or at a rate determined by the physician for at least 2 h to make sure the 131I-MIBG in the infusion line leading from the pump is completely delivered to the patient. At the end of the 2 or 3 h, the saline intravenous lines may be disconnected or set at a rate the physician deems appropriate to maintain hydration. Unless there is a medical necessity, the venous catheter is not removed until 3 d after infusion to minimize radiation exposure to nursing personnel.
Problems
Air occasionally enters the main infusion set after the therapy vial empties. Standardizing the volume in each vial to be infused solves this problem. Before the volume is standardized, all testing for radiolytic decomposition is completed. Once the product passes quality control, saline is added to each vial to equalize the volume in each to 30 mL; in this way, the infusion rate is easily calculated and the total infusion time is known (Table 2). The infusion is stopped about 3 mL before all 30, 60, or 90 mL has finished, depending on whether 1, 2, or 3 vials are being infused. The infusion line is carefully observed from behind a lead glass shield during the last few milliliters of the infusion, and the pump is stopped when the air–fluid mark is about halfway up the 78.74-cm (31-in) extension set tube. If air does enter the line, a quick solution is to affix a 60-mL syringe on the access port closest to the entrance to the pump. Then, the extension set and infusion line are clamped just behind the Y connector the empty syringe is affixed to. A syringe with about 10 mL of saline is affixed to the Y connector closest to the outlet of the pump, and the line is clamped immediately below the saline flush. The infusion line is pulled out from the infusion pump, and the bubbles are pushed up to the 60-mL syringe. When the infusion line is free of air, it is reconnected to the infusion pump, the clamp is released from the extension set and the main infusion line below the pump, and the pump is restarted. If there is some 131I-MIBG in the syringe, it is aseptically reinjected into the vial as part of the flush, or the pump is allowed to pull it back from the syringe.
DISCUSSION
Peristaltic pumps typically use computer-controlled rollers that compress against a pressure plate the tube through which fluid flows. For some reason not fully understood, the rollers and pressure plate in the pump become contaminated. As such, only one pump is strictly used for this purpose. If the pump needs repairs or calibration, it is set aside for the radioactivity to decay and a substitute is used.
131I-MIBG is not approved as a therapeutic agent in the United States. The use of this product in the therapeutic setting must be performed with a Food and Drug Administration–accepted investigational new drug application, along with an institutional review board–approved protocol (number 2012-026/study number MIBG EAP) and in accordance with Nuclear Regulatory Commission title 10 of Code of Federal Regulations part 35.6 or agreement state equivalent. Information on setting up a successful program is provided in appendices S, T, and U of the Nuclear Regulatory Commission NUREG-1556 (15). Furthermore, the radiation safety officer will have to establish safety procedures for the handling of radiopharmaceuticals containing 131I and determine exposure risk to medical personnel and caregivers (3,11,12,16). Initial and ongoing training of medical, nursing, and technical staff, as well as the patient’s caregiver, with respect to radiation safety must also be developed and implemented.
Patients infused with this system are treated with 131I-MIBG obtained from Draximage under its “Expanded Access” protocol as approved by the Cook Children’s Medical Center institutional review board. Because all subjects are minors, assent is obtained when appropriate and informed consent obtained from a parent or guardian.
CONCLUSION
The peristaltic pump method for infusing a high activity or large volume of therapeutic radiopharmaceuticals is a user-friendly and robust system that allows for effective shielding of the radiopharmaceutical during the infusion process. Readily available components mitigate compatibility problems with various pumps and infusion sets. With this system, single or multiple vials linked in series can be connected to the primary intravenous line for infusion of the therapeutic. The chance that air will enter the system can be mitigated as long as the precise volume to be infused and the infusion rate are known.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 5, 2014.
REFERENCES
- Received for publication March 4, 2014.
- Accepted for publication April 18, 2014.





{kind=link}
{kind=link}
{kind=link}