


Abstract
An automated objective striatal analysis (OSA) software program was applied to dopamine transporter 123I-ioflupane images acquired on subjects with varying severities of parkinsonism. The striatal binding ratios (SBR) of the left and right putamina (relative to the occipital lobe) were computed, and the laterality of that measure was compared with clinical symptoms and visual reads. The objective over-read of OSA was evaluated as an aid in confirming the laterality of disease onset. Methods: One hundred one 123I-ioflupane scans were acquired on clinically referred subjects. SPECT images were analyzed using the OSA software, which locates the slices containing the striatal and background (occipital) structures, positions regions over the left and right caudate nuclei and putamina, and calculates the background-subtracted SBR. Seven images were uninterpretable because of patient motion or lack of visualization of the striatum. The remaining 94 scans were analyzed with OSA. Differences between left and right putaminal SBR ranged from 0% to 36.6%, with a mean of 11.4%. When the difference between the SBR of the left and right putamina was greater than 6%, the lower side was taken as the side of onset. Left-to-right differences less than 6% were considered to be nonlateralizing (symmetric). The 94 scans were reviewed independently by 3 masked expert readers. By majority consensus, abnormal findings were seen on 67 of the 94 scans, of which 46 had available clinical findings. Results: Clinically, 34 subjects presented with lateralized tremors and 12 with symmetric or no tremors. Of the 34 cases of clinically lateralized tremors, 26 (76%) were concordant with the OSA findings, 5 were disparate with OSA (15%), and in 3 the OSA results were symmetric (9%). For the same 34 patients, the visual reads were concurrent with clinical tremor findings in 24 cases (71%), 1 was disparate (3%), and 9 visual reads were symmetric (26%). Of the 9 scans deemed symmetric by readers, 4 were correctly lateralized by OSA, and of the 3 symmetric OSA results, 2 were correctly lateralized visually. Conclusion: The OSA program may be a helpful aid in the interpretation of 123I-ioflupane SPECT images for determining laterality representing the asymmetric loss of dopamine transporters in the striata. OSA offers an objective, reproducible over-read evaluation for the laterality of onset in Parkinson disease.
Parkinson disease (PD) is a movement disorder characterized on physical examination by tremor, rigidity, and bradykinesia. The cellular basis of this neurodegenerative disease is the loss of neurons from the nigrostriatal pathway, which has cell bodies in the midbrain and synapses in the striatum. 123I-ioflupane (DaTscan; GE Healthcare) is the radiopharmaceutical approved for aiding the diagnosis of PD. 123I-ioflupane is a chemical analog of cocaine and therefore has high affinity for the presynaptic dopamine transporter (DaT) in the caudate nucleus and putamen in the striatum. Decreased uptake of 123I-ioflupane in the striatum thus indicates a loss of dopaminergic neurons, which occurs in PD and other parkinsonian syndromes such as dementia with Lewy bodies and multiple-system atrophy (1–5). DaT imaging findings are visually read as abnormal if there is unilateral or bilateral loss of striatal uptake. Reader variability in interpretation exists in daily clinical practice and is often due in large part to assessment of whether the degree of asymmetry is sufficient to be deemed abnormal (6).
Neuroregenerative therapies for PD have the advantage of theoretically improving established symptoms but face many steep challenges. Therefore, neuroprotective strategies are also under evaluation (7). Theoretically, neuroprotective therapies would prevent or slow further degeneration and therefore stabilize but not improve existing symptoms. Thus, neuroprotective strategies inherently rely on early detection with minimal motor symptoms or preferably even in the premotor phase of disease. This optimal strategy of detection or diagnosis of preclinical PD relies on imaging because clinical signs and symptoms are by definition not present. Premotor symptoms such as hyposmia, rapid-eye-movement sleep behavioral disorders, and constipation are potential markers for preclinical PD that may provide a method to screen for higher-risk patients many years before the onset of clinical symptoms. DaT imaging in conjunction with screening for these and other symptoms may allow for detection of premotor PD (8).
Most PD patients present initially with hemiparkinsonism or unilateral signs or symptoms. The laterality of the clinical symptoms correlates with greater loss of dopamine transporters in the contralateral striatum. For example, a patient with a right-sided, pill-rolling tremor would be expected to have greater loss in the left putamen than in the right. Typically, patients have lost 50% or more of the dopamine transporters in the striatum when they develop motor symptoms of PD. Not surprisingly, therefore, the absolute loss of 123I-ioflupane uptake in the striatum has been shown to be bilateral even when asymmetric on imaging and clinical presentation (9). The mechanism for why one side degenerates faster or sooner than the other is unclear.
Hypothetical extrapolation of what DaT imaging would show in the premotor phase of PD predicts that the earliest detectable abnormality would be only unilateral. Therefore, assessment of laterality in patients with early symptoms and mild abnormalities on dopamine transporter imaging is clinically important now and also potentially for the future use of DaT imaging for preclinical PD. Given the observer variability in the interpretation of DaT imaging and the desire to detect changes that are potentially subtle and easily missed by the human observer, an automated objective striatal analysis (OSA) software program was recently developed (10). It is applied to dopamine transporter 123I-ioflupane images and calculates the striatal binding ratios (SBR) of the left and right putamina (relative to the occipital lobe). The laterality of that measure can be compared with clinical symptoms and visual reads. In this study, we correlated the clinical, visual, and automated assessments for laterality in the belief that the most accurate and precise assessment is achieved through a combination of analyses.
MATERIALS AND METHODS
Subject Population
The institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived. One hundred one subjects were referred to a single center for DaT imaging by neurologists specializing in the evaluation of movement disorders. The patients’ ages ranged from the 39 to 85 y (mean, 68.5 y; SD, 10.5 y); 65 men and 36 women were imaged (1.8:1).
Clinical Assessment of Tremor
Rest tremor most often occurs in the setting of PD or parkinsonism. The Unified Parkinson Disease Rating Scale was used to follow the longitudinal course of parkinsonism, including tremors, for patients in this study. The lateralization of tremor was determined by the documented medical history of the onset of rest tremor and the more severely affected side on the rating scale during the last physical examination before the DaT imaging. Examinations were performed in the movement disorder clinic by neurologists specializing in movement disorders.
Imaging Protocol
Before injection, patients were premedicated with Lugol solution to block uptake of radioiodine by the thyroid gland. Four hours after injection of approximately 185 MBq of ioflupane, projection data were obtained in a 128 × 128 matrix on a 2-head e.cam camera (Siemens Medical Systems) mounted with low-energy, high-resolution parallel-hole collimators. Projection data were acquired over 120 angles for 30 min. The standard brain protocol was used, whereby the data were reconstructed using filtered backprojection and applying a zoom of 2. As per the manufacturer’s guideline, neither attenuation nor scatter correction was applied.
Visual Reads of the Clinical Scans
Visual reads were performed on the standard clinical images with no additional reorientation or reformatting. The images were transferred to the diagnostic reading station and were read by 2 trained board-certified nuclear medicine physicians already experienced in interpreting ioflupane images. In cases of discrepancy, a third trained reader (with 20 y of experience as the technical director of nuclear medicine and director of imaging for the core laboratory of the Parkinson Progression Markers Initiative clinical trial) made the majority decision, which was the final readout. Scans were read as having normal findings if the striata demonstrated the classic symmetric comma shapes. Scans were read as having abnormal findings if there was unilateral or bilateral loss of the comma appearance or if significant asymmetry was noted between the left and right striata, particularly in the putamen. Readers specifically noted if there was significant asymmetry and, if so, which side was more severely affected. Each reader evaluated the scans independently with no additional reference to other imaging modalities or clinical information.
OSA Automated Image Processing
The processing steps have been previously described in detail, and the algorithm includes correction for suboptimal alignment of the head (10,11).
Briefly, the automated software locates the slices containing the striatal and background (occipital) structures, positions regions over the left and right caudate nuclei and putamina, and calculates the background-subtracted SBR.
For the specific assessment of laterality, when the difference in SBR between the left and right putamina was more than 6%, the lower side was taken as the side of onset. Differences of less than 6% between the sides were considered to be nonlateralizing (symmetric) because 6% is the generally accepted error for quantification in SPECT imaging in these types of scans.
Statistical Analysis
κ value was calculated for agreement between the initial 2 readers. Laterality on clinical examination was considered concordant with imaging if the side contralateral to the tremor showed lower uptake of radiotracer. Percentage agreement with the clinical examination was calculated for visual assessment and OSA. χ2 analysis was performed to analyze differences between visual assessment and OSA.
RESULTS
Seven images could not be interpreted or analyzed because of patient motion or lack of visualization of the striatum. Six of those 7 had such severe loss of uptake in the striata that OSA could not properly detect a maximum. Visually, these patients also had such severe loss of striatal uptake that symmetry could not be assessed. One scan was so severely degraded by patient motion that the readers agreed it was not interpretable and should be repeated. The remaining 94 scans were analyzed with OSA. Differences in SBR between the left and right putamina ranged from 0% to 36.6%, with a mean of 11.4% ± 8.9%. The 94 scans were reviewed independently by 3 masked expert readers. Sixty-seven of the 94 scans had abnormal findings by majority consensus.
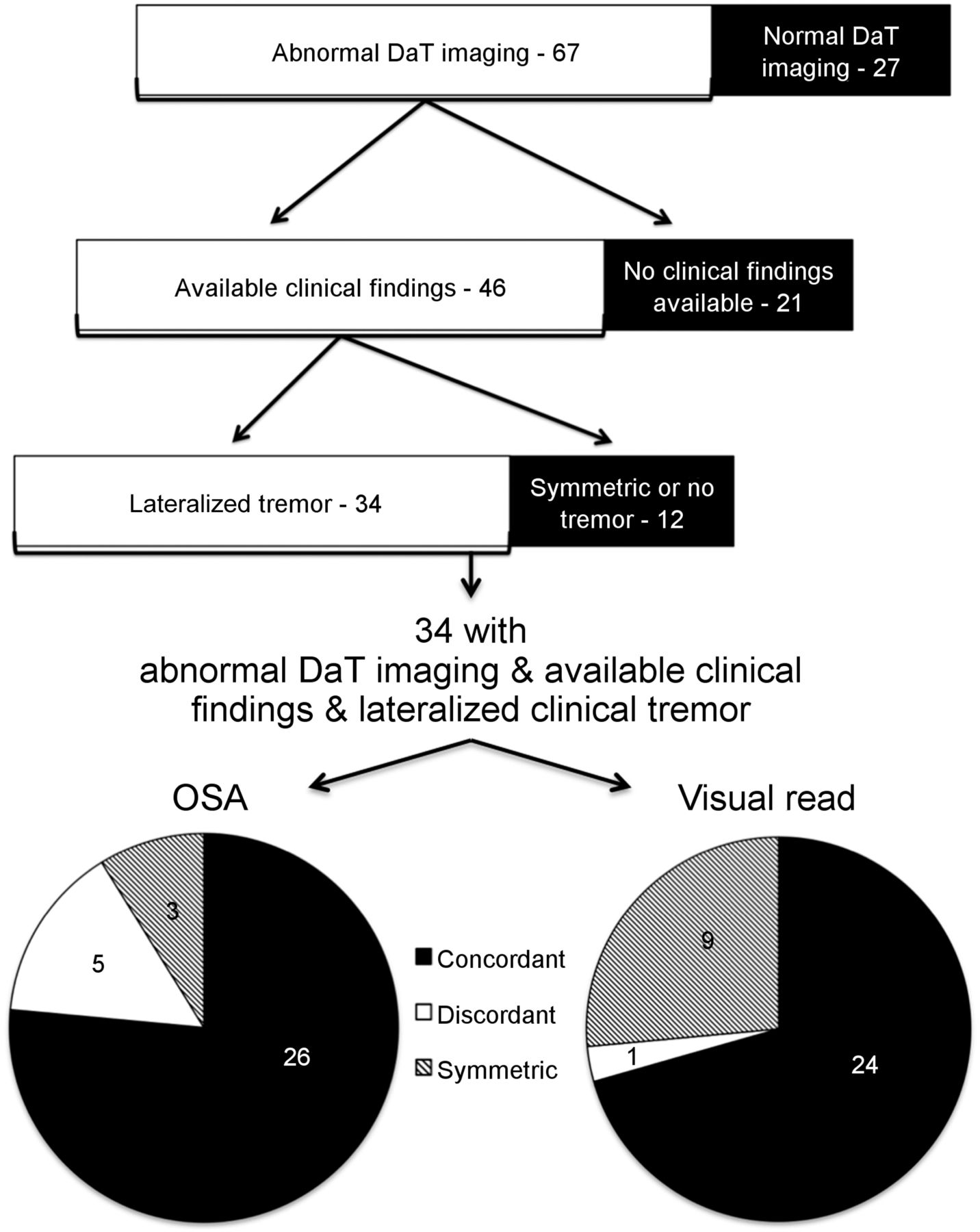
Forty-six of these 67 abnormal scans had available clinical findings. Clinically, 34 subjects presented with lateralized tremors and 12 with symmetric or no tremors. Of the 34 cases of clinically lateralized tremors, 26 (76%) were concordant with the findings of OSA, 5 were disparate with OSA (15%), and in 3 cases the OSA results were symmetric (9%). For the same 34 patients, the visual reads were concordant with clinical tremor findings in 24 cases (71%), 1 case was disparate (3%), and 9 visual reads were called symmetric (26%). Of the 9 scans deemed symmetric by readers, 4 were correctly lateralized by OSA; of the 3 symmetric OSA results, 2 were correctly lateralized visually. In 31 of the 34 cases, the initial 2 readers agreed on symmetry and laterality (if asymmetric). The κ value for the agreement between the 2 readers was 0.72, a high level of agreement. These results are diagrammed in Figure 1.
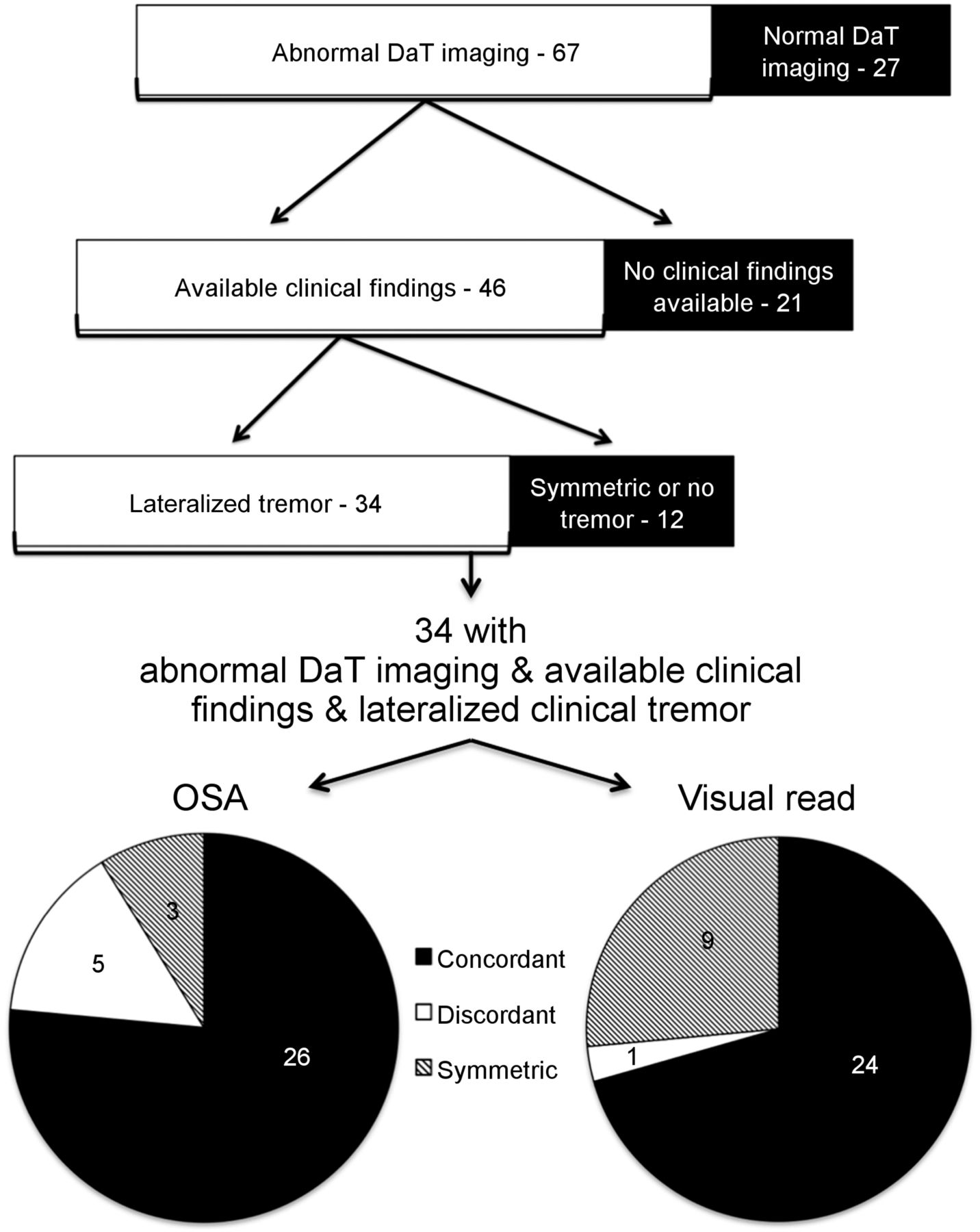
Flow chart showing breakdown of patient population according to findings on DaT imaging, clinical examination, and quantitative software analysis.
Of the 12 patients with no lateralizing tremor, 3 had symmetric tremor and 9 had insufficient tremor for assessment. OSA results were symmetric in 3 and asymmetric in 9. Visual reads were symmetric in 1 and asymmetric in 11.
χ2 analysis showed no significant difference between OSA and visual ratings (z = 0.47, P > 0.05). Assuming that, by chance alone, 17 of 34 would be correct, OSA performed significantly better than chance (z = 2.22, P < 0.05). On the other hand, compared with chance, visual scoring approached statistical significance but did not perform significantly better (z = 1.68, P > 0.05).
DISCUSSION
Although there was no statistically significant difference between OSA and visual assessment for laterality, a separate analysis showed that OSA performed significantly better than chance whereas visual assessment did not. Therefore, the OSA program may provide a potentially helpful over-read when DaT images are used for determining laterality representing the asymmetric loss of dopamine transporters in the striata. OSA could complement visual reads by delivering an objective, reproducible evaluation that may be particularly helpful in following patients in clinical trials. Further study needs to be done to determine whether providing OSA outputs to the radiologists affects their decisions.
Our study had limitations, including small sample size. Visual scoring was trending toward significance and might have been significantly better than chance if our sample size had been larger. The fact that clinical findings were available for 46 of the 67 abnormal DaT images may have introduced a selection bias, but as far as we know, the availability of clinical findings was random. Clinical findings of laterality may have been confounded by conditions such as rigidity or preexisting essential tremor. Also, scans were considered abnormal by majority consensus of the visual reads.
Filippi et al. reported finding bilateral dopaminergic deficits in patients with hemiparkinsonism (9). The study compared patients who had clinical hemi-PD (unilateral tremor) with age-matched healthy controls. Given the wide range of normal striatal uptake of ioflupane with increasing age, for the purpose of diagnosis our methodology may have the potential advantage of comparing symmetry within an individual rather than with age-matched controls.
CONCLUSION
Although the clinical and research significance of these results will require further study such as a prospective trial, the statistically significant capability of OSA to determine laterality supports the possibility that the combination of visual assessment and OSA may aid in more accurate diagnosis of early PD.
DISCLOSURE
This work was conducted with support from NIH-2R44NS055475. Phillip H. Kuo is a consultant for GE Healthcare and has received grant funding from GE Healthcare. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 13, 2014.
REFERENCES
- Received for publication November 9, 2013.
- Accepted for publication December 27, 2013.





{kind=link}