


Abstract
A patient with metastatic papillary thyroid carcinoma (after surgical resection of tumor and positive lymph nodes) undergoing thyroid ablation therapy with 131I is described. Whole-body scintigraphy was performed 1 wk after ablation therapy to evaluate the presence of residual disease. The whole-body images demonstrated an artifact caused by tracer accumulation in the patient’s scalp related to recent hair coloring. Common etiologies of false-positive 131I scintigraphic findings are briefly reviewed. The importance of taking preventative measures to decrease the number of false-positive findings and recognizing these findings when they occur is discussed.
Sodium iodide labeled with 131I is frequently used to detect and treat thyroid carcinoma. Whole-body scintigraphy with 131I- or 123I-labeled sodium iodide is commonly used to determine whether thyroid ablation is appropriate for the patient. Thyroid ablation involves oral administration of therapeutic doses of 131I, either in liquid or capsule form. Whole-body scintigraphy is frequently performed 2–10 d after ablation therapy and again after 6–12 mo to detect if residual or recurrent local or metastatic disease may be present. Whole-body scintigraphy with 131I has sensitivity between 60% and 80% and specificity greater than 90% (1). The etiologies of the false-positive findings have been reviewed and well documented (2). In most cases, false-positive radioiodine distribution is attributed to contaminated personal items or, as illustrated by the following case study, physiologic variants such as accumulation from perspiration and other bodily secretions (3–9). Medical practitioners should be mindful of the etiologies of these false-positive findings and take appropriate steps to properly identify and exclude them when they are suspected.
CASE REPORT
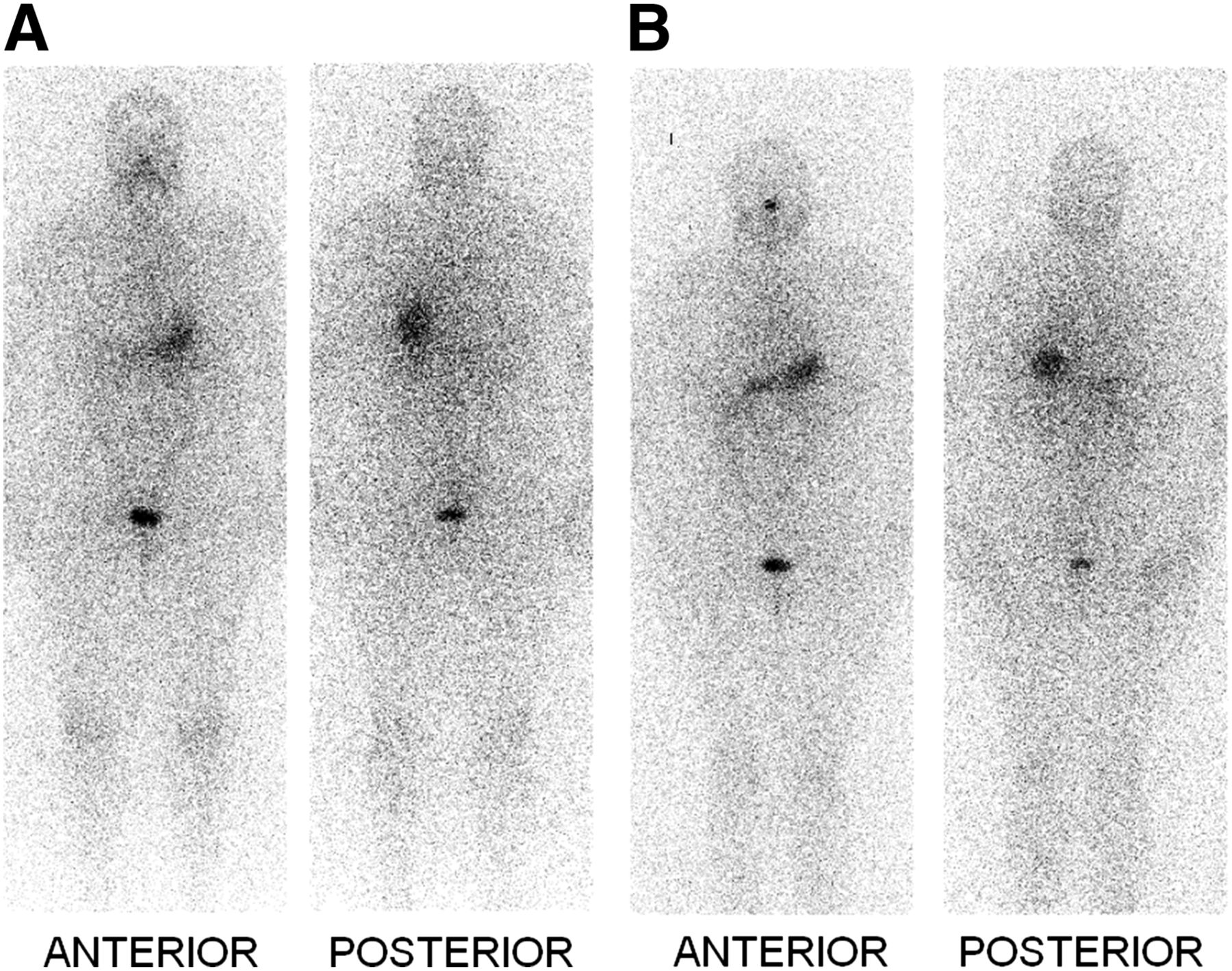
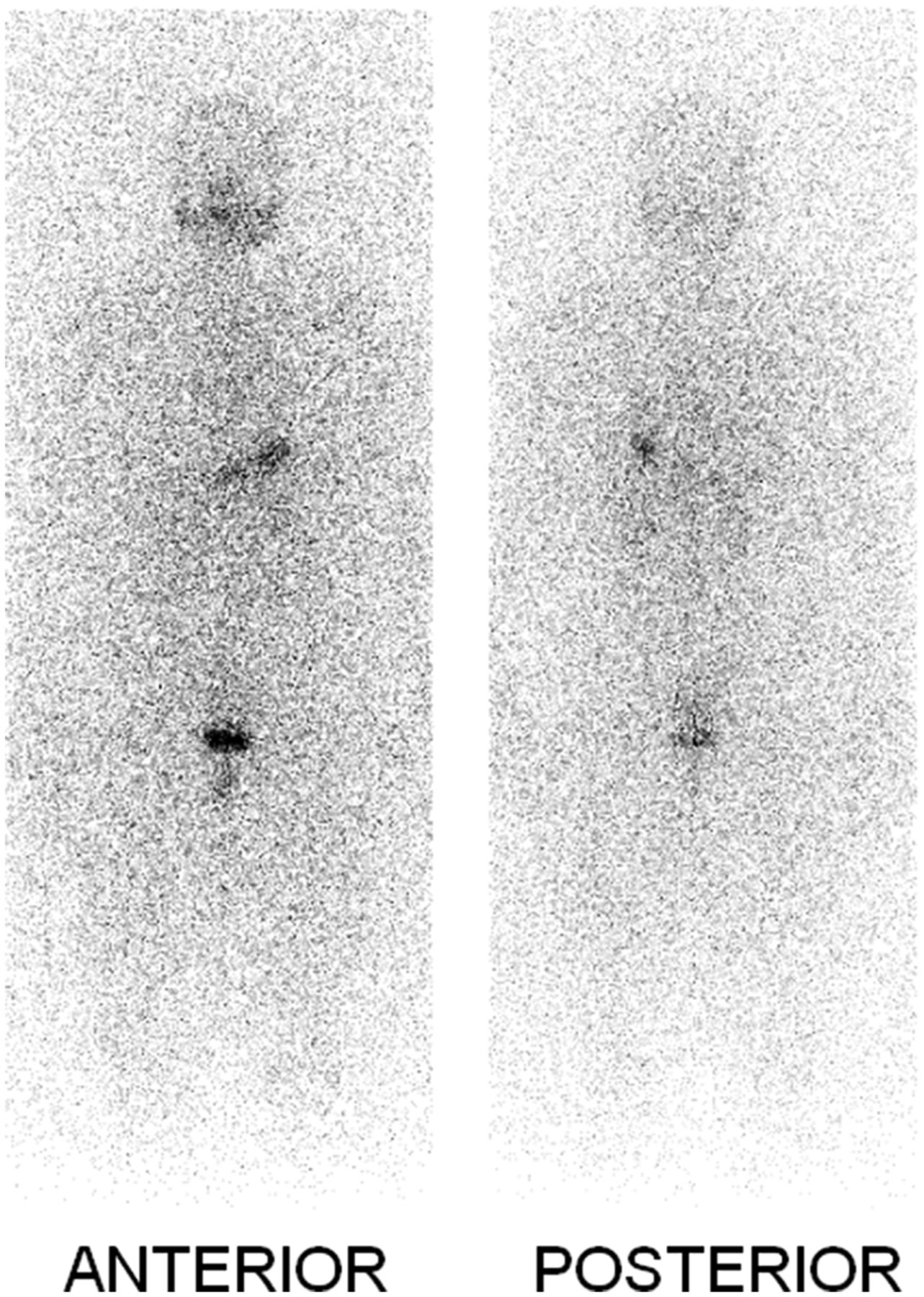
A 42-y-old woman with a history of metastatic papillary thyroid carcinoma had undergone surgical resection of the tumor along with several positive lymph nodes and radioiodine ablation. Whole-body 123I scanning was performed 1 mo before the ablation (Fig. 1A) and just before the ablation (Fig. 1B). These scans showed a normal physiologic distribution of the radioiodine. Before the therapy, the patient’s thyroglobulin level was 1.7 ng/mL (reference range, 0.1–36.8 ng/mL), and her thyroid-stimulating hormone level was 96.1 mIU/L after she had received recombinant human thyroid-stimulating hormone (Thyrogen [thyrotropin alfa]; Genzyme Corp.). The patient was treated with 6.25 GBq of 131I administered orally in capsule form. A whole-body scan obtained 1 wk after ablation therapy showed diffuse increased activity in the periphery of the head, likely in the calvarium (Fig. 2A), which was not present in the preablation scans (Fig. 1). No intense abnormal focal activity was identified in the postablation images to suggest discrete metastatic lesions. Normal physiologic activity was noted in the nasal mucosa and liver. On questioning, the patient revealed that she had colored her hair between the radioiodine ablation treatment and the follow-up scan. To rule out 131I activity on her hair, the patient was instructed to return home and wash her hair thoroughly. She returned 3 d later and images of the head and neck were obtained in anterior, posterior, and lateral projections (Fig. 2B). The neck and the nasal mucosal activity were present and were as expected. The activity in the head was persistent and was likely in the scalp, not in hair, because of the patient’s reported good daily wash. A repeated whole-body scan that was obtained 15 mo later showed no scintigraphic evidence of iodine-avid lesions to suggest residual or recurrent disease (Fig. 3). In addition, the patient’s laboratory values at that time were stable and within normal limits.
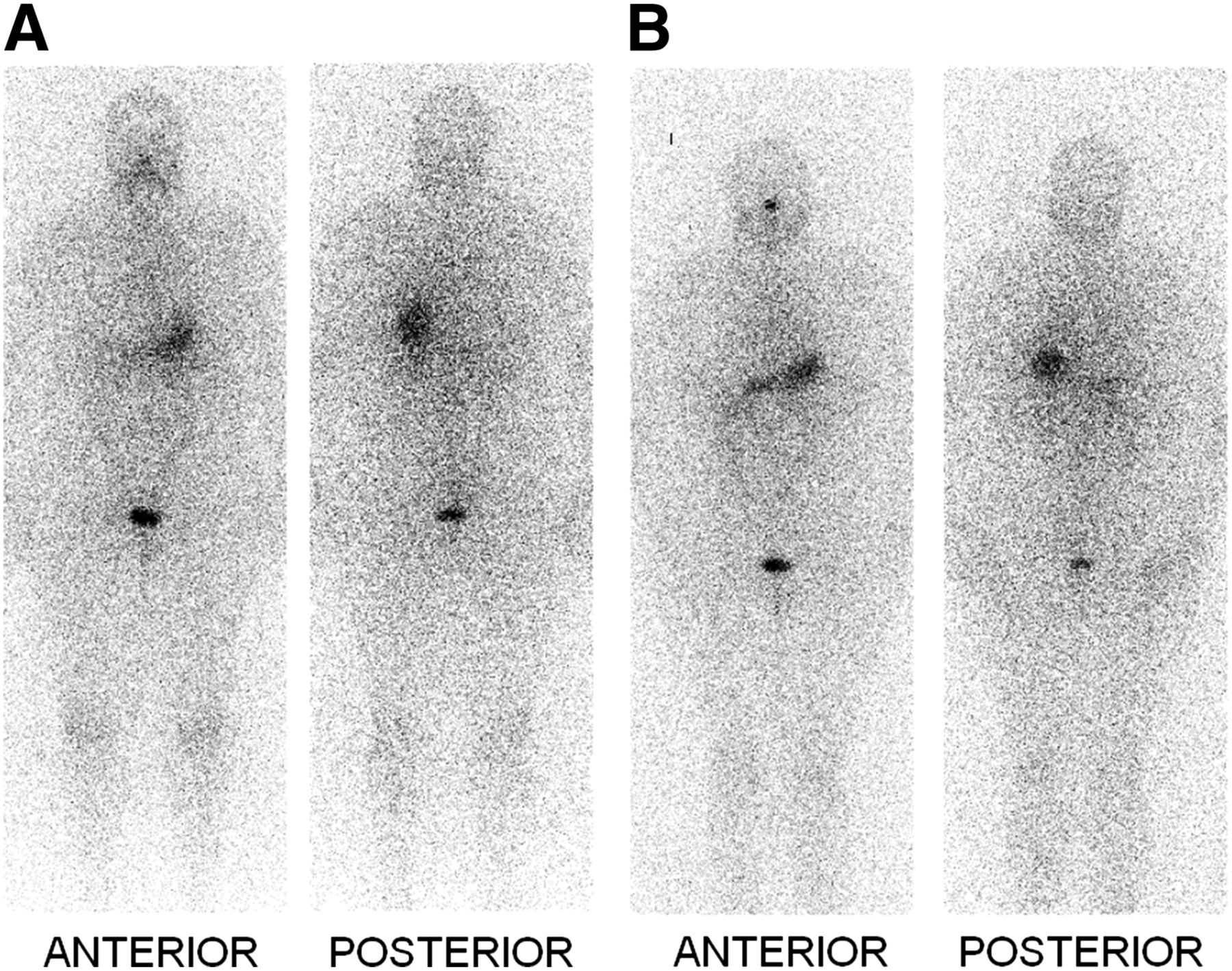
Whole-body iodine scans before radioiodine ablation, in anterior and posterior projections. (A) Scan 1 mo before therapy. (B) Scan on day of radioiodine therapy. There is physiologic distribution of tracer in nasal mucosa, stomach, urinary bladder, and background.
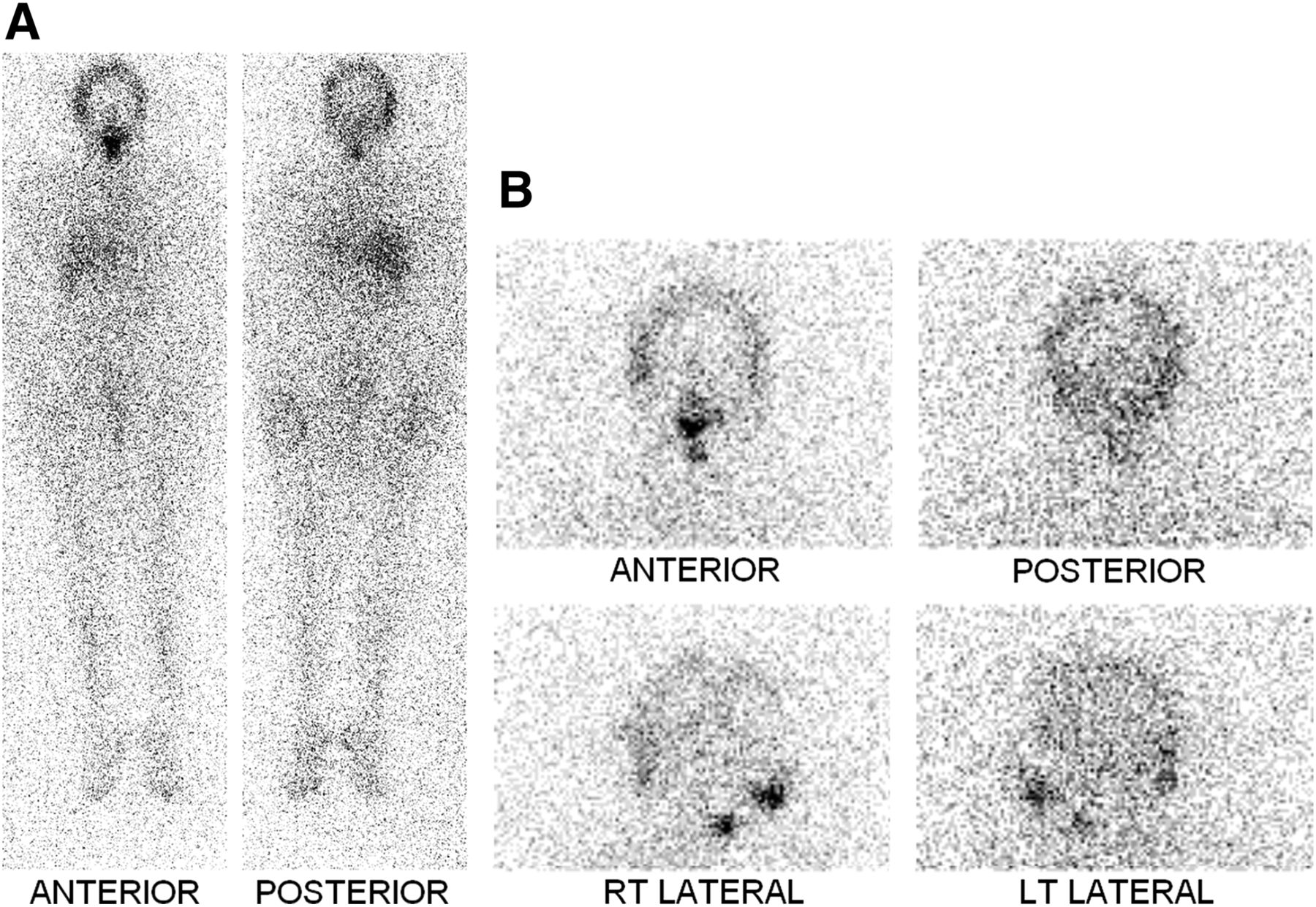
(A) Whole-body iodine scan 1 wk after therapy. There is focal activity in lower neck consistent with iodine-avid tissue that had been treated with ablation dose. Liver activity is physiologic after therapy. There is diffuse helmet-shaped activity in head, likely in scalp or hair. (B) Images of head and neck in anterior, posterior, and lateral projections 10 d after therapy. Neck and nasal mucosal activity is present as expected. Activity in head is persistent and likely is in scalp, not in hair, because of patient’s reported good daily wash.

Whole-body iodine scan for routine follow-up 15 mo after ablation. No abnormal activity is identified to suggest iodine-avid lesion. No focal activity in skull or scalp region is seen.
DISCUSSION
To our knowledge, this is the first reported incidence of a false-positive 131I scan of the scalp from hair coloring with a clear timeline of the events and a relatively long-term follow-up to exclude metastatic disease of the scalp. The diffuse increased activity noted in the calvarium in the postablation scans was likely not disease-related, taking into account the patient’s stable thyroglobulin and thyroid-stimulating hormone values and the lack of other abnormal focal activities in the images. Because the thyroglobulin levels were low with stimulation and high thyroid-stimulating hormone values, the new calvarial distribution was not considered to be metastatic. Therefore, we postulate that the irritation from the hair dye may have caused some degree of folliculitis. Subsequently, perspiration accumulating along the scalp may have resulted in an increased 131I distribution.
Several studies have described false-positive findings in whole-body scintigraphy with 131I. Such findings are primarily due to physiologic secretions and distribution in tissues that concentrate the tracer, followed by contaminated personal items, such as handkerchiefs or jewelry, belonging to the patient (10,11). Nishizawa et al. found that 2 d after administration, the concentration of 131I in perspiration was about half the concentration in blood (12). Ash et al. reported uptake in the scalp from accumulated perspiration due to not washing hair and application of petroleum-based jelly to prevent hair drying (6). Meyers et al. reported scalp uptake of 131I after hair dyeing; however, the thyroglobulin levels were elevated and metastatic disease thus could not be ruled out (5). For the case presented in this report, because we had laboratory tests and follow-up scans that ruled out metastatic disease, the evidence is clearer for increased 131I activity in the scalp after hair coloring.
CONCLUSION
Precautions should be taken by medical personnel to reduce false-positive findings. These measures include instituting a thorough checklist to ensure that all personal items have been removed from the patient before scanning. In addition, patients should be counseled to avoid processes such as hair coloring that may cause irritation to the scalp and increase the accumulation of perspiration and activity in the scalp. It is important to recognize false-positive findings when they occur to prevent inaccurate conclusions on the disease and unwarranted investigative examinations.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 4, 2013.
REFERENCES
- Received for publication November 27, 2012.
- Accepted for publication January 23, 2013.





{kind=link}
{kind=link}
{kind=link}