


Abstract
Patients prepared by the generally used fasting protocol show variable myocardial 18F-FDG uptake, which may result in difficult interpretation of mediastinal 18F-FDG uptake. This retrospective study described the effect of a 1-d fat-allowed, carbohydrate-restricted diet on myocardial 18F-FDG uptake. Methods: The study included 100 patients on a carbohydrate-restricted diet from the Medical Center Leeuwarden and 100 patients on an unrestricted diet from the University Medical Center of Utrecht. A visual uptake scale was used, with category 0 indicating myocardial uptake less than liver uptake, category 1 indicating myocardial uptake comparable to liver uptake, and category 2 indicating myocardial uptake considerably higher than liver uptake. Results: After a carbohydrate-restricted diet, 68% of patients had a homogeneously low myocardial uptake of 18F-FDG (category 0), 14% had moderate myocardial uptake (category 1), and 18% had homogeneously intense myocardial uptake (category 2). Without a carbohydrate-restricted diet, 69% of patients showed a homogeneously intense myocardial uptake (category 2), 16% a moderate myocardial uptake (category 1), and 15% a homogeneously low myocardial uptake (category 0). Conclusion: A fat-allowed, carbohydrate-restricted diet starting the day before 18F-FDG administration suppresses myocardial 18F-FDG uptake satisfactorily.
PET using 18F-FDG is widely applied to stage malignant diseases and to evaluate cellular-level metabolic changes in tumors after therapy. The generally accepted patient preparation protocols for 18F-FDG PET or 18F-FDG PET/CT involve fasting for approximately 6 h (range, 4–12 h).
The purpose of fasting is to produce lower levels of serum glucose and insulin, enabling optimal uptake of 18F-FDG, a glucose analog, in pathologic conditions characterized by increased glycolysis.
In the fasting state, oxidation of fatty acids is the most predominant energy source available to the myocyte, supplying over half the myocardial energy. The presence of insulin may lead to increased expression of insulin-sensitive glucose transporters (predominantly glucose transporter 4), and when increased glucose oxidation rates supply more than half the myocardial energy, the balance shifts away from fatty acid metabolism to glucose metabolism. Consequently, myocardial uptake of 18F-FDG may vary greatly with increasing insulin levels (1). Furthermore, marked variability of regional myocardial uptake over time was reported in patients who underwent whole-body PET/CT at multiple time points, each time after 6 h of fasting (2). High myocardial 18F-FDG uptake, usually mainly in the left ventricle, is unwanted since it may hamper image reading in the thoracic and upper abdominal area. High physiologic myocardial 18F-FDG uptake has been reported to result in both false-positive and false-negative findings (3,4). A patient preparation method that minimizes myocardial 18F-FDG uptake is expected to facilitate mediastinal staging and detection of focal lung disease near the left ventricle of the heart.
Because prolonged fasting did not seem to influence physiologic 18F-FDG uptake in the myocardium, perhaps because the energy balance was not shifted far enough away from glucose metabolism, we hypothesized that prescribing a low-carbohydrate diet may lower myocardial 18F-FDG uptake by a shift of the myocardial energy balance in the proper direction, as was previously described by Lum et al. (5) Therefore, we included a 24-h low-carbohydrate diet in the patient preparation protocol, at implementation of PET/CT in our institution in 2005. In this retrospective study, myocardial 18F-FDG uptake in patients from our hospital on a low-carbohydrate diet was compared with patients from another hospital without such a diet preparation.
MATERIALS AND METHODS
Subjects
Both 100 patients on a low-carbohydrate diet from the Medical Center Leeuwarden and 100 patients on an unrestricted diet from the University Medical Center of Utrecht were included in this retrospective study. The patients underwent PET or PET/CT in the fourth quarter of 2008.
All patients were scanned for oncologic reasons, primarily lung cancer, head and neck cancer, and lymphoma. Patients with diabetes mellitus and renal disease were excluded, because most of these patients do not receive a standard patient preparation protocol, and they usually already have an adapted diet. Also, patients with known coronary artery disease and sarcoidosis were excluded because these heart conditions are known to interfere with myocardial 18F-FDG uptake.
Diet Protocol
Two days before scanning, patients being treated in the Medical Center Leeuwarden outpatient clinic received a confirmation telephone call from the technologist, who outlined the diet instructions and described a menu of permitted and nonpermitted foods (Appendix). Clinical patients were instructed via the nursing staff. These diet instructions were then followed for 24 h before scanning.
Scanning Procedure
In Medical Center Leeuwarden, a Biograph 6 lutetium oxyorthosilicate Hi-Rez hybrid PET/CT scanner was used, with CT-based attenuation correction (Siemens Medical Systems). The patients had followed the carbohydrate-restricted diet for 1 d before the PET/CT investigation. A solution containing 0.2% locust bean gum and 2.5% mannitol was used as an oral contrast agent, to provide useful bowel distension (optimal imaging of the intestinal tract) while avoiding contrast material–induced PET artifacts (6). The patients had fasted for 6 h before the injection of 3.7 MBq (0.1 mCi) of 18F-FDG per kilogram of body weight, with a maximum of 333 MBq (9 mCi). Blood glucose levels were measured before administration. Ninety minutes after the 18F-FDG administration, the data acquisition of the diagnostic CT scan was started, with intravenous administration of 120 mL of Optiray 300, followed by a 3-dimensional PET scan with the patient in the same supine position. The field of investigation ranged from the base of the skull to the mid thigh in 6–9 (patient length–dependent) 3-min bed positions. The total imaging time of a PET/CT study lasted approximately 30 min. The CT parameters were 95 kV (quality reference mAs [a mAs value that will be used in a normal-sized patient] CARE Dose 4D [the dose modulation system used by the CT vendor]), a slice thickness varying from 0.6 to 5.0 mm, collimation of 6 × 1 mm, and pitch of 1.33. PET images were reconstructed iteratively using ordered-subset expectation maximization software.
In the University Medical Center of Utrecht, an Allegro PET scanner (Philips) was used with attenuation correction by a 68Ge transmission scan. (Philips). Patients had fasted for 6 h before the injection of 3.7 MBq (0.1 mCi) of 18F-FDG per kilogram of body weight. Blood glucose levels were measured before administration. Sixty minutes after the 18F-FDG administration, the data acquisition of the 3-dimensional PET scan was started, with the patient supine. The field of investigation ranged from subcranial to above the knees in ten 3-min bed positions. Including 12 transmission frames of 38 s, the total imaging time of a PET/CT study lasted approximately 40 min. The PET images were reconstructed using a 3-dimensional row-action maximum-likelihood algorithm.
Quantification of 18F-FDG Uptake and Image Analysis
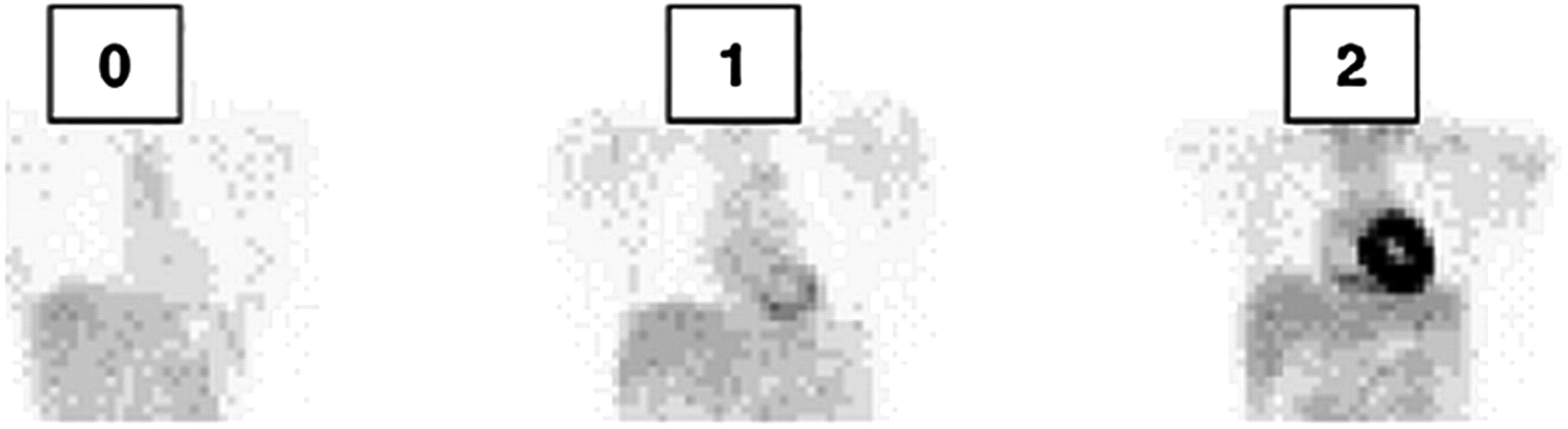
Because of the differences in PET hardware and acquisition protocols between the 2 hospitals, comparison of standardized uptake value in the myocardium was deemed unreliable. Also, assessment of only the intensity of myocardial uptake based on a qualitative visual uptake scale was not considered reliable enough. For this reason, a visual uptake categoric scale was used, comparing myocardial uptake to liver uptake. Myocardial 18F-FDG uptake was graded using 3 categories (Fig. 1): category 0, myocardial uptake less than liver uptake (homogeneously minimal); category 1, myocardial uptake comparable to liver uptake (mostly mild or moderate uptake); and category 2, myocardial uptake considerably higher than liver uptake (homogeneously intense).
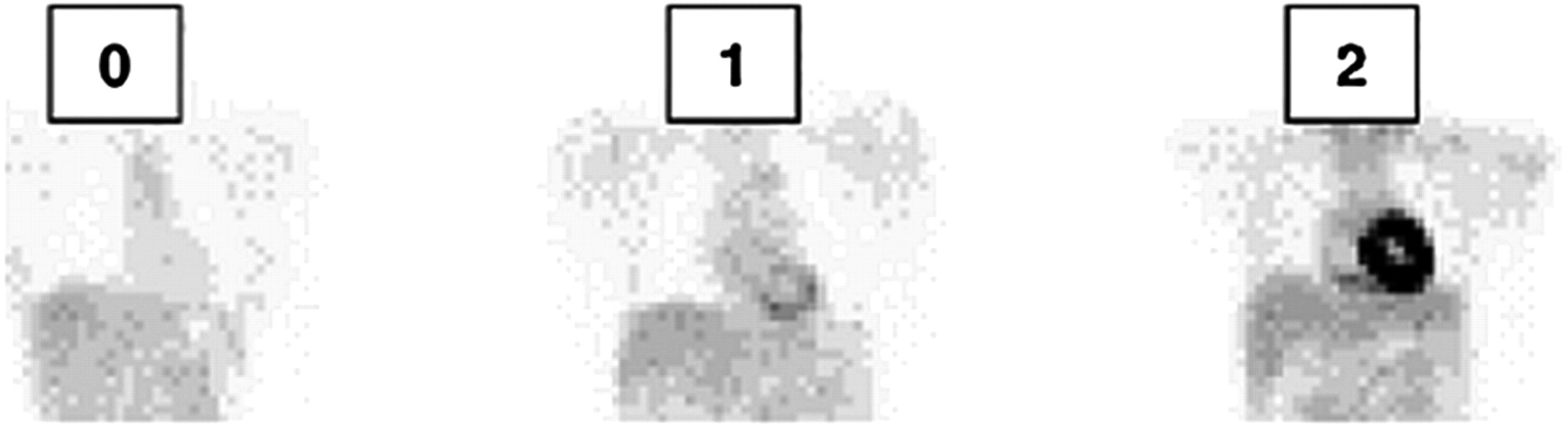
Myocardial uptake levels compared with liver, in categories 0, 1, and 2.
Visual assessment was conducted as a triple-observer analysis; when all 3 observers agreed on the category of myocardial uptake, the categorization was definitive. In cases of disagreement, the 3 observers performed a consensus reading and discussed the category until they reached an agreement.
Statistical analysis was performed using the SPSS statistical software package (release 15.0; IBM) for Windows (Microsoft) and a χ2 test.
RESULTS
Table 1 shows the results as percentages for the 100 patients with a carbohydrate-restricted diet and the 100 patients without a carbohydrate-restricted diet, per category of myocardial uptake. The diet-related difference in 18F-FDG myocardial uptake is statistically significant (χ22 = 63.837; P < 0.0001).
Contingency Table of Myocardial 18F-FDG Uptake and Diet
Table 2 shows that no difference was found between the sexes in the beneficial effect of lowering myocardial uptake with a carbohydrate-restricted diet.
Contingency Table of Myocardial 18F-FDG Uptake and Diet Analyzed by Sex
Table 3 shows that weight, expressed as body mass index, did not contribute to the degree of myocardial 18F-FDG uptake.
Contingency Table of Myocardial 18F-FDG Uptake and Diet Analyzed by Body Mass Index
With reference to age, patients were separated into categories of 5 y each. No difference in myocardial uptake was found among the different age categories.
DISCUSSION
These results show that a fat-allowed, carbohydrate-restricted diet starting the day before 18F-FDG administration suppresses myocardial 18F-FDG uptake satisfactorily. A homogeneously low myocardial uptake of 18F-FDG was found in 68% of patients after a carbohydrate-restricted diet, compared with only 15% of patients without such a diet.
The use of a fat-allowed, carbohydrate-restricted diet in patient preparation before 18F-FDG scanning may have some advantages, such as more accurate recognition of disease in the mediastinum and of focal lung disease near the myocardium. In a case report describing a patient who had 2 sequential 18F-FDG examinations for the characterization of a solitary pulmonary nodule, the patient had mistakenly eaten a meal just before the first examination. Those images showed high myocardial uptake, and the nodule was almost missed because of low focal uptake. In the second examination, performed after proper preparation, the images showed low uptake in the myocardium but high focal uptake in the nodule (4).
A second advantage of the fat-allowed, carbohydrate-restricted diet is that the lower myocardial 18F-FDG uptake may increase accuracy in the detection of myocardial disease, such as myocardial sarcoidosis. In our experience, low myocardial uptake made it possible to recognize pericarditis in a patient who was referred for fever of unknown origin (Fig. 2) (7).
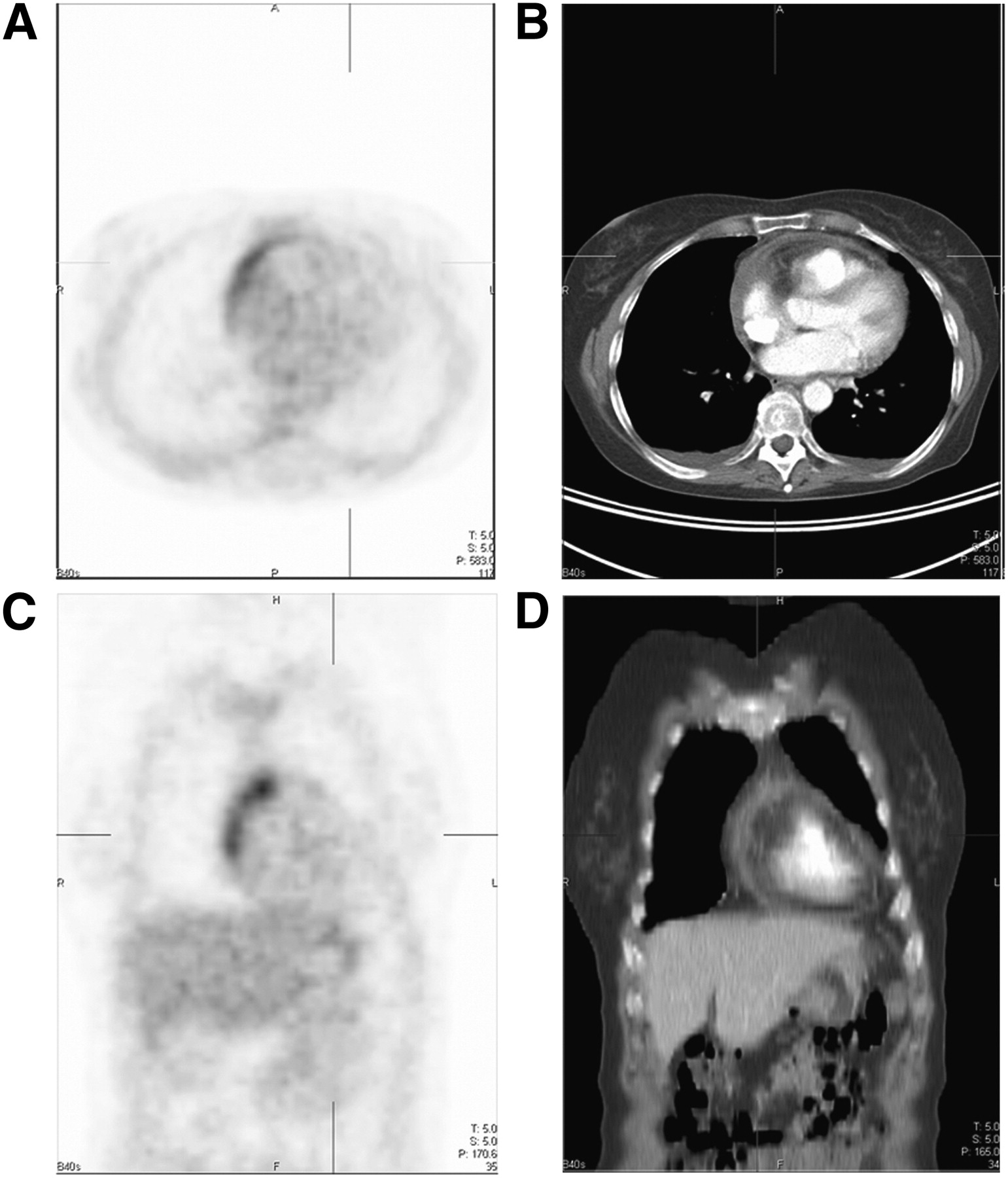
Transverse 18F-FDG PET slice (A), corresponding transverse CT slice (B), coronal 18F-FDG PET slice (C), and corresponding coronal CT slice (D). The irregular increased 18F-FDG uptake in ventral portion of pericardium adjacent to right ventricular wall would not have been recognized in the otherwise moderate to high 18F-FDG uptake ventral in right ventricular wall. Both transverse and coronal CT slices show thickened pericardium ventral in right ventricular wall, up to 8 mm.
As a third advantage, this adapted method of patient preparation may permit the detection of biologically active coronary artery disease. In a retrospective study, 32 patients were instructed to eat a low-carbohydrate, high-fat meal the night before and to not eat or drink the morning of the 18F-FDG PET/CT procedure, except for a vegetable oil drink (ClearScan; E-Z Em Inc.). In 20 of 32 patients (63%), myocardial 18F-FDG suppression was good; in 15 patients, pathologic 18F-FDG uptake in 1 or more coronary segments could be identified, in correlation with angiography results suggestive of vulnerable (inflamed) coronary plaque (8).
Several methods to decrease myocardial 18F-FDG uptake have been investigated. Caffeine is known to elevate free fatty acid blood levels, creating a shift from glucose to free fatty acid metabolism in myocytes. However, no influence of caffeine on uptake of 18F-FDG in the myocardium was found (9,10). Other investigated factors such as age and fasting time did not seem to influence 18F-FDG physiologic uptake in the myocardium (1).
Our results are concordant with those of Williams and Kolodny, who found an obvious suppression of myocardial standardized uptake value after patient preparation with a high-fat, low-carbohydrate diet, eaten as a meal 3–6 h before 18F-FDG injection (11). The average maximal standardized uptake value in the myocardium was 8.8 ± 5.7 for the fasting group and 3.9 ± 3.6 for the group that ate the high-fat, low-carbohydrate meal.
The underlying mechanism of suppression of myocardial 18F-FDG uptake is likely the result of the Randle cycle, which has established that fatty acid loading suppresses glucose metabolism in a variety of tissues, including myocardium (12). Furthermore, a report described that elevated blood levels of free fatty acids decreased myocardial glucose uptake (13). Free fatty acids were also reported to inhibit glucose transporter 4 expression in cardiac muscle (14).
In support of the mechanism of the Randle cycle operating in myocardium is a recent study on rodents separated into 3 dietary groups: low (0.1% of total energy), intermediate (52%), and high (78%) carbohydrate content. A diet consisting of 4 wk of carbohydrate restriction resulted in marked and reproducibly reduced myocardial 18F-FDG uptake, whereas glucose, insulin, and glucagon did not differ among the 3 rodent groups. Ketone bodies were increased by 6- to 7-fold and provided an alternative substrate to glucose (15).
The optimal composition of a preparatory diet is not yet defined. Allowing the use of oil and butter to fry or bake fish and meat and the consumption of (usually full-fat Dutch) cheese in our patient preparation is probably just as effective in suppressing myocardial 18F-FDG uptake as the use of a vegetable oil drink. The use of a vegetable oil drink has advantages, however, such as an increase in compliance and knowledge of the exact intake. Lack of patient compliance with any diet is a known problem and probably also played a role in our patient group. Eighteen of the 100 patients had a diffuse high myocardial uptake despite the carbohydrate-restricted diet. Although we did not use a questionnaire, noncompliance with the diet is a probable cause.
CONCLUSION
A fat-allowed, carbohydrate-restricted diet starting the day before the 18F-FDG administration suppresses myocardial 18F-FDG uptake satisfactorily. There have been only a few retrospective studies using a carbohydrate-restricted diet to prepare patients for 18F-FDG imaging, and to our knowledge, ours was the first study that compared the effect of a fat-allowed and carbohydrate-restricted diet on myocardial 18F-FDG uptake in daily routine in large patient groups between 2 hospitals. Because retrospective studies may potentially suffer from various forms of bias, of which selection bias probably is the most important, future prospective randomized studies are needed.
APPENDIX
Low-Carbohydrate, Fat- and Protein-Permitted Diet
Permitted:
Fatty unsweetened chicken, turkey, fish, meat, meat-only sausages, fried eggs, bacon, butter or margarine
Liquids (coffee or tea) without sugar
Milk products with a maximum of 3 portions per day (milk, yogurt, cheese)
Vegetables (e.g., green salad, no beans)
Sugar substitutes
Not permitted:
Bread, bagels, cereals, soup with vermicelli, potatoes, rice, cookies, toast, crackers, muffins, peanut butter, jam, nuts, fruit juice, candy, chewing gum, mints, cough drops, beans, alcohol
Acknowledgments
We thank Hester Bruinsma and Hielke Roosjen for bringing the concept from Washington, DC, to Leeuwarden, and we thank John Buijs for mentoring 3 of us (Evelien Hut, Thomas Pol, and Freerk-Jan Fokstra). No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 27, 2011.
REFERENCES
- Received for publication February 18, 2010.
- Accepted for publication April 4, 2011.





{kind=link}
{kind=link}