


Visual Abstract
Abstract
Intestinal 18F-FDG uptake is variable in whole-body PET/CT. In cancer patients, particularly those suspected of relapse or metastasis, 18F-FDG absorption might interfere with scan interpretation. This study evaluated the effect of diet on intestinal 18F-FDG absorption. Methods: In total, 214 patients referring for oncologic 18F-FDG PET/CT participated. They were randomly divided into 2 groups and asked to follow either a routine diet (RD) or a low-carbohydrate, high-fat diet (LCHFD) for 24 h before the study. The small bowel and different parts of the colon (the cecum; the ascending, transverse, and descending segments; and the hepatic and splenic flexures) were evaluated and visually interpreted by nuclear medicine experts. Bowel uptake was graded through comparison with that in the liver as absent, mild, moderate, or severe. Results: Significantly higher 18F-FDG uptake in the descending colon (P = 0.001) and small intestine (P = 0.01) was observed in the RD group than in the LCHFD group. After patients with bowel cancer were omitted from the statistical analysis, no significant differences in the final results were seen. Conclusion: An LCHFD for 24 h before 18F-FDG PET imaging resulted in lower 18F-FDG uptake in the descending colon and small bowel than did an RD, assisting the interpreting physician by reducing the intestinal activity interference for more accurate diagnostic interpretation.
PET/CT is one of the most useful imaging modalities for metabolism studies at the cellular and molecular levels. Among imaging procedures, PET/CT is substantially superior for diagnosis, staging, restaging, and prognostic evaluation of oncologic patients. 18F-FDG is the most common radioisotope used worldwide for PET/CT in malignant diseases (1), but a normal distribution of 18F-FDG distribution based on glucose metabolism can also be seen in other organs, including brain, myocardium, kidneys, urinary bladder, and bowel (1,2).
Methods for suppressing myocardial 18F-FDG uptake in oncologic patients have been previously reported (3–5). To our knowledge, however, no study has been conducted to determine the effects of diet on bowel 18F-FDG uptake, the importance of which cannot be underestimated in the interpretation of PET/CT results for the abdomen and pelvis.
Previous researchers attempted to minimize physiologic 18F-FDG uptake throughout the body by focusing mainly on reducing myocardial 18F-FDG uptake through a low-carbohydrate high-fat diet (LCHFD) or prolonged fasting (4,5). The few studies that have been performed to control bowel 18F-FDG uptake have focused on the effect of bowel preparation (6) and on classification of uptake and its potential interference with scan interpretation for abdominal–pelvic (mainly colon) cancer (7,8). Therefore, we decided to design a study to evaluate the effect of an LCHFD diet on intestinal 18F-FDG uptake.
MATERIALS AND METHODS
In total, 214 patients older than 18 y (107 men and 107 women; age range, 18–84 y) with suspicion of, or proven, malignancies were enrolled. The protocol was evaluated and approved by the Institutional Research Ethics Committee, and the study plan was fully explained to the patients and written informed consent was obtained from all. PET/CT was requested at different stages of the disease. Exclusion criteria included a serum glucose level of more than 200 mg/dL at the time of radiotracer injection, failure to fast, known bowel disease, or pathologic bowel 18F-FDG uptake interfering with physiologic bowel activity.
Patients were randomly assigned into 2 groups, with one group taking a routine diet (RD) and the other an LCHFD for 24 h before the 18F-FDG PET/CT scan. All patients received the required details about their diet and were instructed to fast for at least 6 h before the study. Foods in the LCHFD included boiled eggs, grilled beef, fried chicken, and vegetables, and for 24 h before the study any carbohydrate-containing beverages or meals were avoided. PET/CT was performed on a Biograph TruePoint 6 (Siemens) approximately 60 min after intravenous administration of 392 ± 63 MBq (10.6 ± 1.7 mCi) of 18F-FDG according to body weight (5.2 MBq/kg [0.14 mCi/kg]). The PET image reconstruction protocol included 4 iterations per 21 subsets, a 5-mm gaussian postsmoothing filter, and a 168 × 168 matrix, using the point-spread-function–based reconstruction algorithm TrueX. The protocol was set at 3 min/bed position as the default and 4 min/bed position in patients with a body mass index of more than 35. Low-dose CT (50 mA, 110 − 130 kV) was applied for attenuation correction.
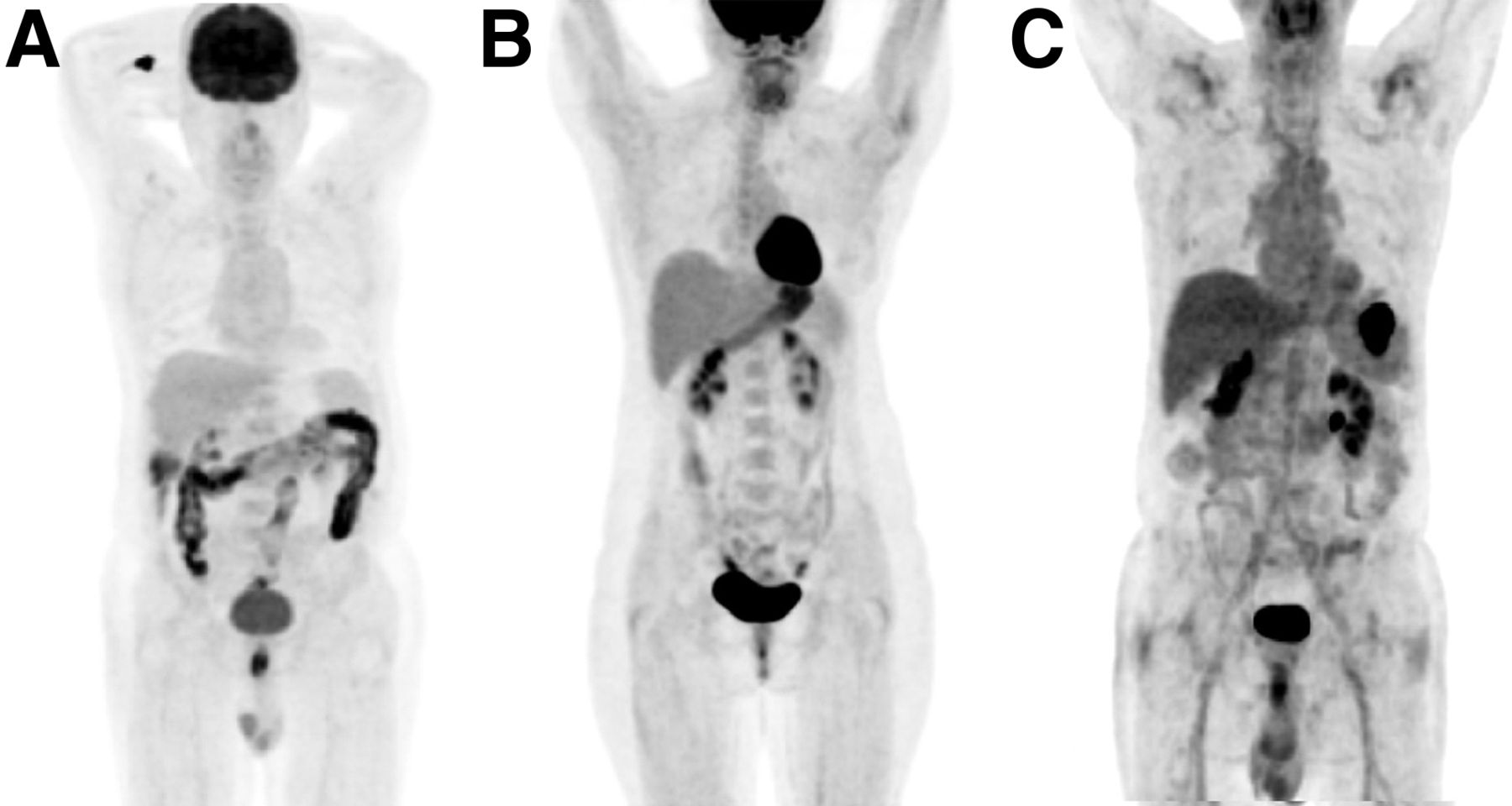
18F-FDG uptake was visually evaluated by 2 nuclear medicine physicians, who graded the uptake in the small intestine and different parts of the large bowel, including the ascending, transverse, and descending segments; the cecum; and the hepatic and splenic flexures. In cases of disagreement, a third specialist’s opinion was the criterion for decision making. The intensity of uptake in the small intestine and in the various colon segments, in comparison to liver uptake (Fig. 1), was classified as absent, mild (less than liver), moderate (equal to liver), or severe (more than liver).

Grading bowel uptake by comparing it with that of liver as severe (more than liver) (A), moderate (equal to liver) (B), or mild (less than liver) (C).
Statistical analyses were conducted using SPSS, version 22 (IBM), and an independent-sample t test, χ2 test, or Fisher exact test was used to assess the relationship between the type of diet and the investigated outcome, including the intensity of 18F-FDG uptake in the various bowel regions. A P value of less than 0.05 was considered statistically significant.
RESULTS
In total, 214 patients were enrolled, randomly divided into 2 groups. One group followed the RD, whereas the other thoroughly followed a 24-h LCHFD. Baseline data analysis of heart rate, blood pressure, and fasting blood sugar, besides demographic characteristics consisting of sex, age, height, and weight, was done to ensure proper randomization of potential confounders in the study groups, and the demographic and baseline characteristics were balanced between the groups (Table 1).
Demographics and Baseline Characteristics of Subjects
The intensity of 18F-FDG uptake in the different segments of colon is presented in the Table 2. Significantly higher 18F-FDG uptake was observed in the descending colon and small intestine after the RD than after the LCHFD.
18F-FDG Distribution Patterns in Bowel Regions
Thirty-four patients with a history of colon cancer were removed from the statistical analysis. The intensity of 18F-FDG uptake in the descending colon and small intestine was lower in the LCHFD group than in the RD group, whereas no remarkable difference in 18F-FDG uptake in other segments of the colon was noted between the 2 groups (Table 3).
18F-FDG Distribution Patterns in Bowel Regions after Exclusion of Patients with History of Colon Cancer
As shown in Table 2, significantly higher 18F-FDG uptake in the descending colon and small intestine was observed in the RD group than in the LCHFD group.
DISCUSSION
Epidemiologic studies have shown that colon cancer is the third most lethal cancer in the world, after prostate and lung cancer in men and after breast and lung malignancies in women (9,10).
The choice of colon cancer treatment depends on multiple factors, including the patient’s basic health status and the size, location, and extent of the tumor. Surgery is the most commonly used therapy, depending on the size and extent of the tumor (9,10). PET/CT is an appropriate diagnostic tool for evaluating the regional or distant tumor extension and, accordingly, has a vital clinical effect on patients’ management at different stages of the disease. In cases of suspected tumor recurrence or liver metastasis, PET/CT is effective in deciding the feasibility of surgery. PET/CT is also much more useful than conventional imaging in decision making during monitoring of the response to a given therapy.
Physiologic 18F-FDG absorption in the small and large intestines can interfere with accurate interpretation and may mask true lesions or, conversely, cause a misdiagnosis and false-positive results. Control of intestinal 18F-FDG uptake is expected to reduce possible false-positive and false-negative results.
After our previous study leading to success in suppressing myocardial 18F-FDG uptake by an LCHFD (5), we were encouraged to test the effect of diet on intestinal 18F-FDG absorption. Interestingly, the application of an LCHFD versus an RD resulted in a significant reduction in 18F-FDG uptake in the descending colon and small intestine. To the best of our knowledge, no study has yet been conducted on the effect of an LCHFD on intestinal absorption. Considering the significant prevalence of colon cancer and the role of PET/CT in its management, the results of such a study ought to be extremely valuable in improving the quality of images of the abdominopelvic cavity in particular. The goal of our study was to investigate the effect of diet on reducing 18F-FDG uptake in the bowel.
In this well-controlled randomized trial, we attempted to illustrate changes in 18F-FDG uptake in the intestinal system when an LCHFD was used for patients’ preparation. The LCHFD might not be suitable for vegetarians, but because the focus of the assessment was on carbohydrate restriction along with an LCHFD, plant protein foods (e.g., soy) can be used as a substitute for animal proteins in the given food list.
A significant statistical relationship was found between diet and 18F-FDG distribution in the descending colon and small intestine, and diet can be an effective controllable factor to reduce bowel 18F-FDG uptake.
Of the patients in the LCHFD group, 78.5% had no 18F-FDG absorption or had only mild uptake in the descending colon, and 94.4% also had no 18F-FDG uptake or mild absorption in the small intestine. Moderate to severe 18F-FDG absorption (equal to or greater than the liver activity) was present in 36.4% of patients in the RD group but only 21.5% in the LCHFD group. In general, moderate to severe intestinal 18F-FDG absorption was reported in 16.8% of patients in the RD group and 5.6% in the LCHFD group (P = 0.01).
The results of the study showed that an LCHFD regimen for 24 h before the scan shifted the 18F-FDG uptake by the small intestine and descending colon from moderate or severe to mild or absent. In a 2015 study, background bowel 18F-FDG uptake was evaluated in 326 female breast cancer patients who underwent 18F-FDG PET for primary staging, none of whom had hypertension or diabetes. Colon absorption was categorized (as low or high) on the basis of visual and quantitative assessments, and the average SUVmax in 8 segments of the intestine (duodenum, jejunum, ileum, cecum, hepatic flexure, splenic flexure, descending colon, and sigmoid) was reported as total-bowel SUVmax. Age, fasting blood sugar, body mass index, triglycerides, cholesterol, high-density lipoprotein, and low-density lipoprotein were considered cardiometabolic related factors. Total-bowel SUVmax had a positive relationship with age, body mass index, triglycerides, cholesterol, and low-density lipoprotein and a negative relationship with high-density lipoprotein. Multivariate analysis represented that body mass index and triglycerides were independent factors associated with bowel 18F-FDG uptake. According to these results, high bowel 18F-FDG uptake on the PET scan could be due to changes in lipid metabolism and an increased risk of cardiometabolic disease in nondiabetic and nonhypertensive patients (11), whereas in our study, the limited use of glucose and increased lipid levels in the diet resulted in a significantly reduced 18F-FDG uptake in the small intestine and descending colon.
The first study on factors potentially influencing intestinal 18F-FDG absorption was conducted in 1998. In that study, age, sex, and bowel habits had an effect on 18F-FDG absorption; no relationship, however, was found between free fatty acid level and bowel 18F-FDG uptake. Moreover, female sex, older age, and constipation were associated with higher 18F-FDG uptake (12).
Insulin increases glucose uptake by enterocytes and consequently increases bowel absorption in diabetic patients (13–15). However, a wide range of intestinal 18F-FDG uptake was observed in nondiabetic subjects. Another study concluded that hypoglycemic oral agents such as metformin were considered a factor causing higher 18F-FDG uptake, to a significant extent in the colon and to a lesser extent in the small intestine (13–18). Furthermore, a study in 2017 revealed that metformin consumption remarkably increased colonic 18F-FDG absorption, but this increased absorption was independent of an increase in energy expenditure or core body temperature. In other words, there was no relationship between maximal colonic 18F-FDG uptake and energy expenditure or core body temperature (19).
With discontinuation of metformin 48 h before the scan in the diabetic patients of this study, the effect of metformin interference on bowel 18F-FDG uptake was eliminated and only the effect of diet on bowel uptake was investigated.
Recently, the probability that intestinal bacteria have a role in luminal 18F-FDG uptake has been raised, and treatment with rifaximin before PET has been proposed to reduce luminal 18F-FDG uptake. Rifaximin is likely to cause different degrees of 18F-FDG uptake through changing the population of the intestinal bacteria and by the altering the flora and host metabolism (20). Another study evaluated the effect of administering N-butylscopolamine to decrease bowel artifacts during 18F-FDG PET. The results revealed that N-butylscopolamine could potentially improve the quality of PET images and their reporting as well (21).
The Randle cycle describes a biochemical mechanism that maintains a cellular fuel metabolism balance between glucose and free fatty acid oxidation by which glucose oxidation is decreased in the presence of free fatty acids. The significance of the glucose–fatty acid cycle is that it may introduce a new aspect to more precise hormonal control by adding a nutrient-mediated modification (22). This fact has been proven in that the consumption of each nutrient (glucose vs. fatty acid) inhibited the use of the other in isolated myocardial and skeletal muscle (23), but no corresponding data exist to justify the effect of a nutrient shift on the smooth muscles of the intestine. The result of our previous study, about the factors affecting myocardial 18F-FDG uptake, demonstrated that in 107 patients with LCHFD, there was a significant statistical relationship between descending colon 18F-FDG absorption and myocardial 18F-FDG uptake (P = 0.001) (5). However, despite a meaningful shift in 18F-FDG absorption by the descending colon and small intestine, 18F-FDG did not show a significant shift from moderate or high to mild or absent uptake.
CONCLUSION
Management of physiologic bowel 18F-FDG uptake can play a key role in accurately identifying colon diseases by effectively deterring the occurrence of false-positive or false-negative results. Patient preparation using an LCHFD for 24 h before 18F-FDG PET imaging resulted in lower 18F-FDG uptake in the descending colon and small intestine and consequently better-quality images, in particular for precise characterization and interpretation of abdominopelvic findings.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online July 9, 2021.
REFERENCES
- Received for publication September 30, 2020.
- Accepted for publication March 26, 2021.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.