


Article Figures & Data
Figures
- FIGURE 1.
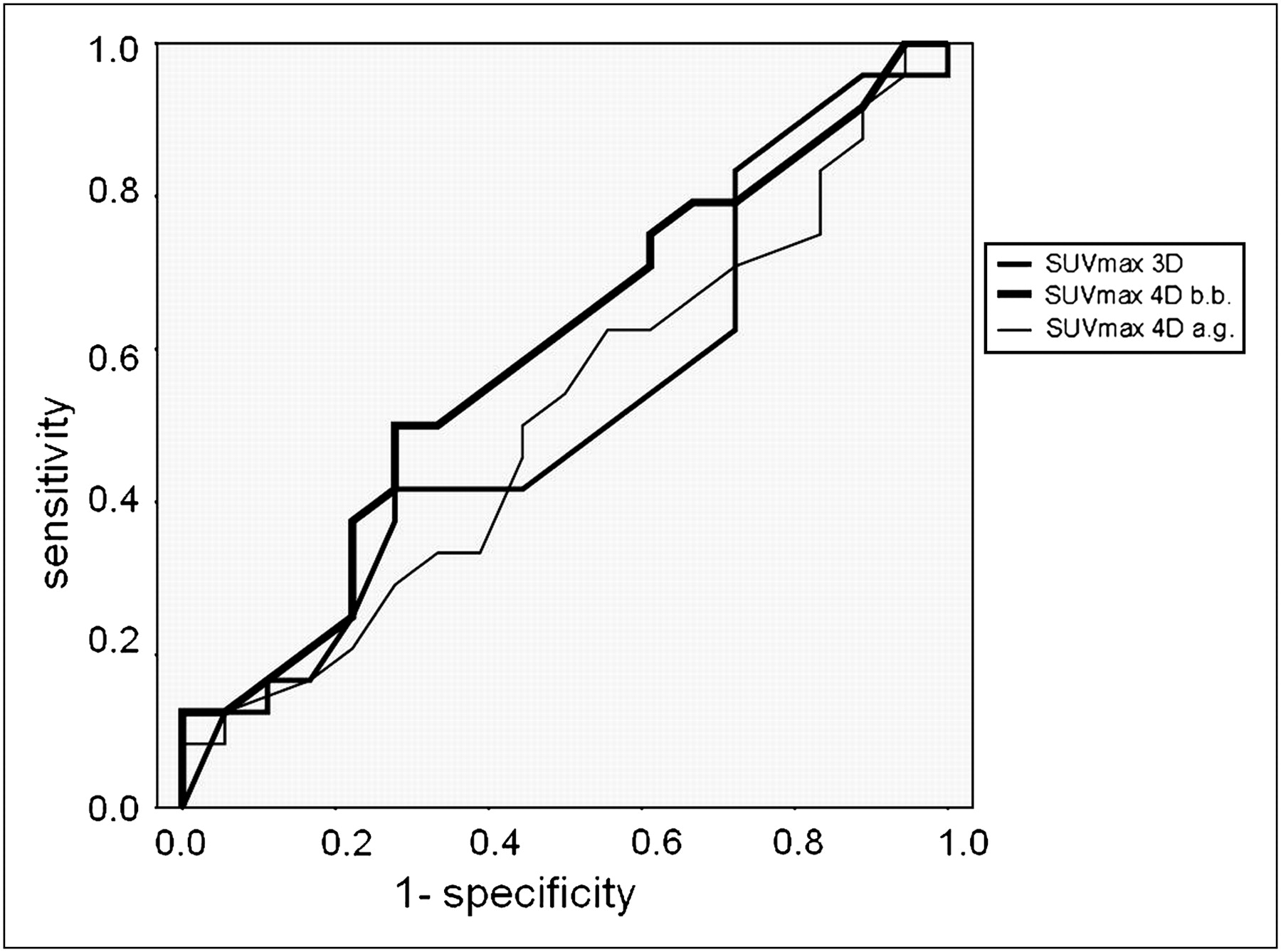
ROC curves of 3D and 4D (best bin and average gated) statistical parameters. Area under curve was 0.5185 for 3D, 0.5938 for 4D best bin, and 0.5093 for 4D average gated. 4D best bin showed best value, with no statistically significant differences from the other techniques. a.g. = average gated; b.b. = best bin.
- FIGURE 2.
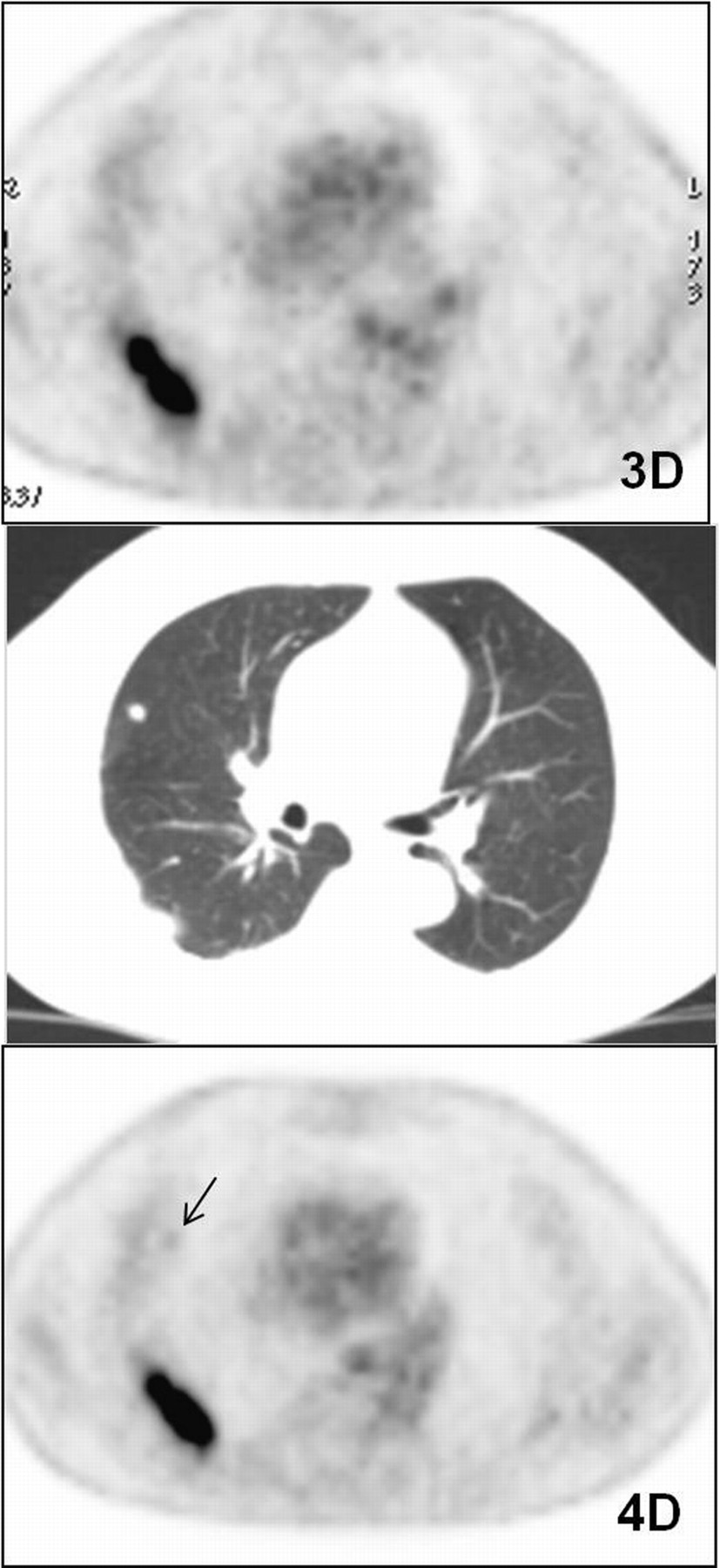
Example of lesion that cannot be visualized on 3D axial image but is detectable on 4D best-bin axial image. Study is of patient 11, who had small cell lung cancer with 2 pulmonary lesions. CT image (center) shows one lesion in right lower lobe (maximum diameter, 4 cm) and another in right upper lobe (8 mm). Larger lesion has high avidity for 18F-FDG (SUVmax in 3D and in best bin of 4D, 8.4 and 11.1, respectively), whereas smaller lesion (arrow) is detectable only in 4D study (SUVmax, 1.1).
- FIGURE 3.
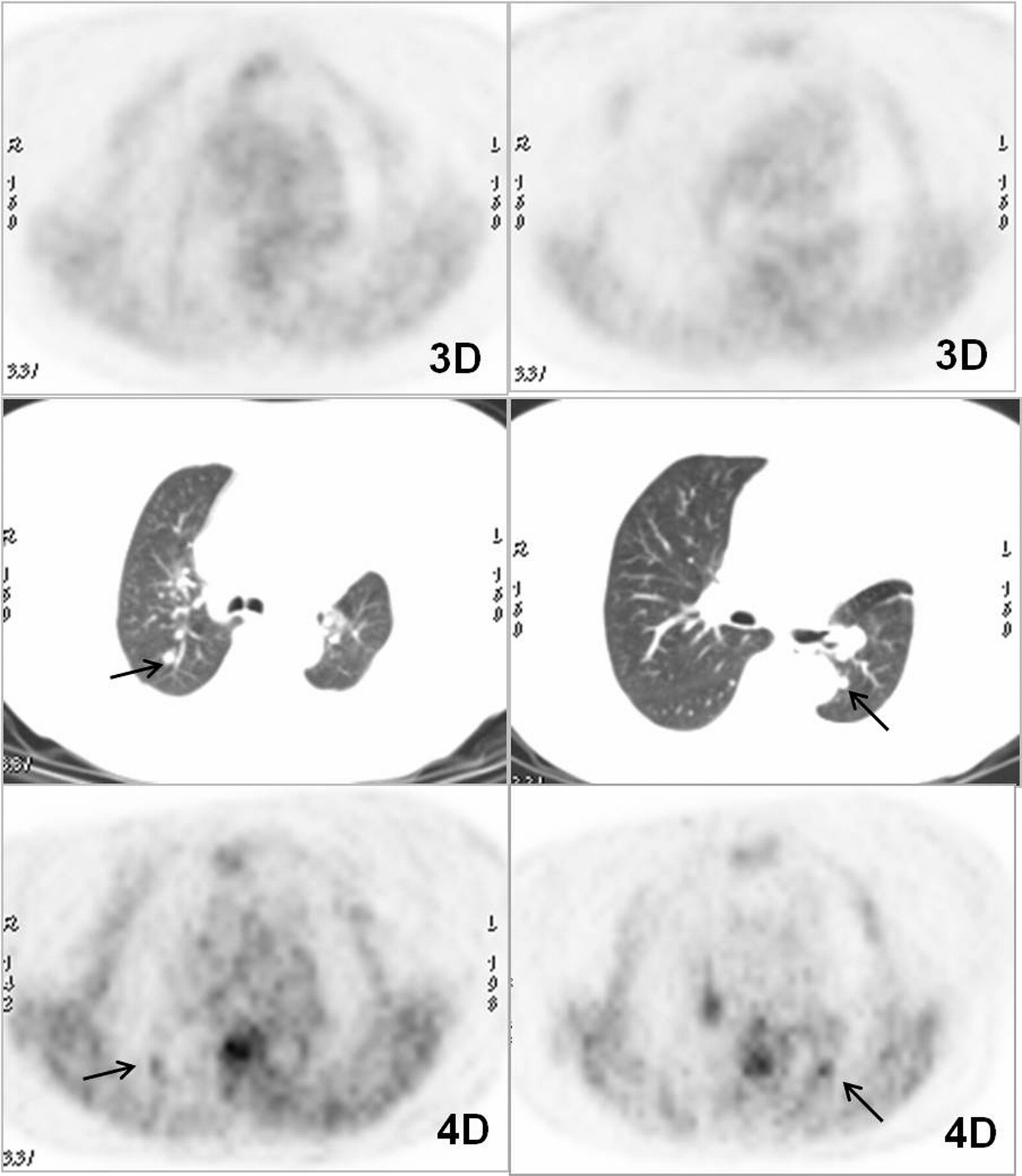
Example of higher lesion contrast with respect to background lung activity in 4D study than in 3D study in patient with 2 pulmonary lesions smaller than 1 cm. Study is of patient 26, who had history of treated non–small cell lung cancer. CT images (center) show one lesion in right upper lobe (maximum diameter, 8 mm) and another in left lower lobe (8 mm). Both (arrows) show faint uptake on 3D axial images (SUVmax, 0.8 and 1.4, respectively) that improves in best-bin 4D images (SUVmax, 1.9 and 2.9, respectively).
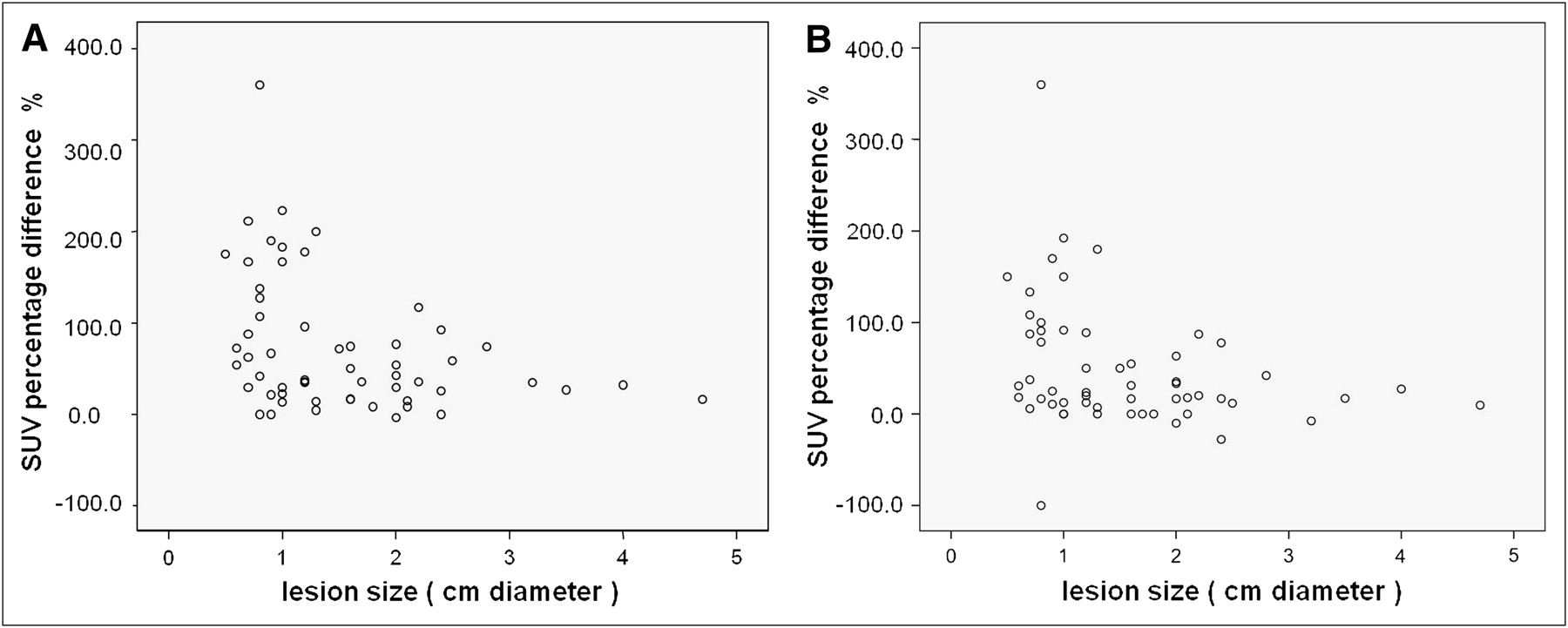
- FIGURE 4.
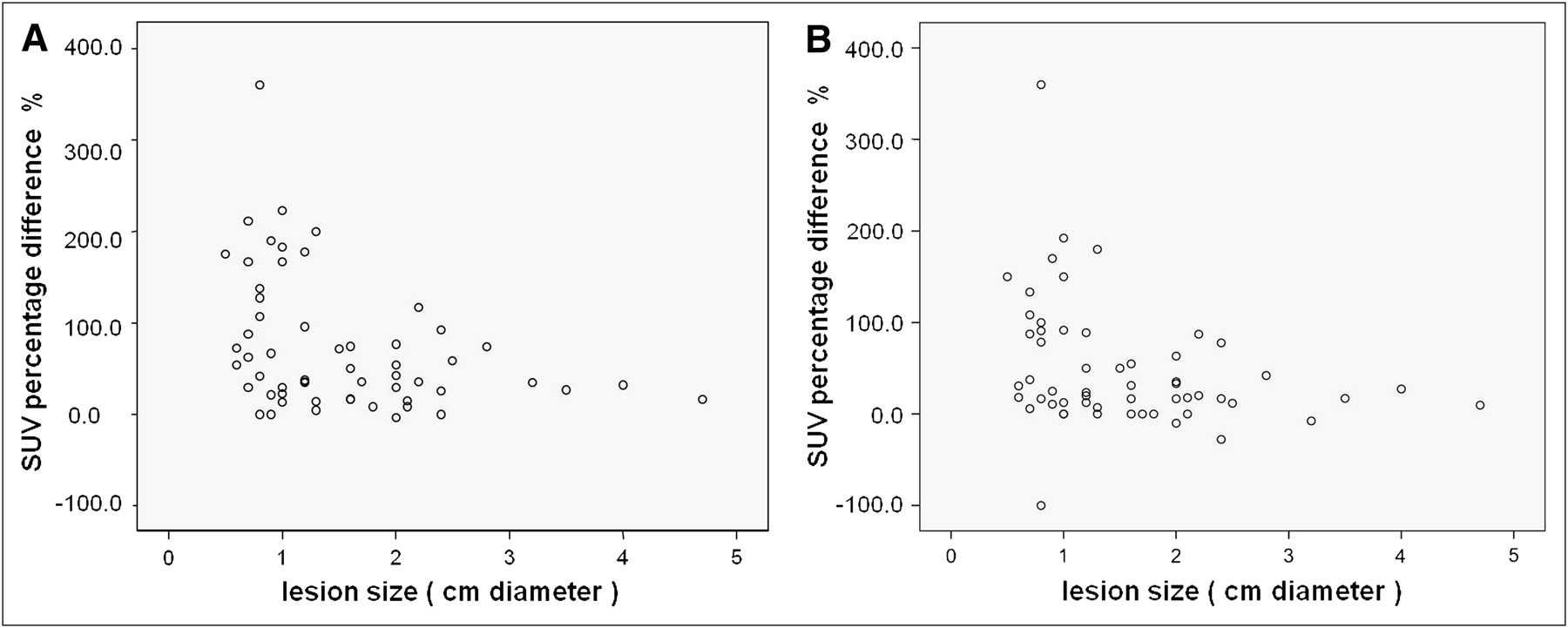
Correlation between lesion size and SUVmax percentage difference between 3D and best-bin 4D studies (A) and between 3D and average gated 4D studies (B). Both graphs show statistically significant (P < 0.05) higher increase in SUVmax in smaller lesions than in larger ones.


Tables
Classification Imaging result Les no. Pt no. Sex Age (y) NB LC Hy NB Diam (cm) Location SUVmax 3D (A) SUVmax BB 4D (B) Bin % Dif (B − A) SUVmax AG 4D (C) % Dif (C − A) 3D BB 4D AG 4D Hy 3D BB 4D AG 4D 1 1 M 73 — — 1.0 LUL 2.4 3.1 2 29.2 2.7 12.5 B M M TN FP FP 2 1 1.3 LUL 1.4 1.6 1 14.3 1.5 7.1 B B B TN TN TN 3 2 F 71 Y — Testicular 2.1 LUL 17.4 21.5 2 14.9 20.5 17.8 M M M Mts melanoma TP TP TP 4 3 F 54 — — 2.8 LUL 1.9 3.3 6 73.7 2.7 42.1 B M M Hamartoma TN FP FP 5 4 M 68 Y — Prostate 2.0 RLL 6.8 9.7 6 42.6 9.2 35.2 M M M NSCLC TP TP TP 6 5 M 78 Y — Melanoma 2.5 LUL 1.7 2.7 5 58.8 1.9 11.7 B M B FN TP FN 7 6 F 54 — — 1.3 LUL 2.2 2.3 2 4.5 2.2 0 B B B TN TN TN 8 7 M 60 — — 1.0 LLL 1.8 2.2 3 22.2 1.8 0 B B B Epidermal FN FN FN 9 8 M 70 Y — Larynx 3.5 LUL 4.1 5.2 3 26.8 4.8 17.0 M M M TP TP TP 10 8 2.0 RUL 3.0 2.9 2 −3.3 2.7 −10.0 M M M TP TP TP 11 8 1.7 Lingula 1.7 2.3 2 35.3 1.7 0 B B B FN FN FN 12 9 M 80 — — 1.6 RUL 1.2 1.4 1 16.6 1.4 16.7 B B B TN TN TN 13 9 0.8 Lingula 1.2 1.7 1 41.6 1.4 16.7 B B B TN TN TN 14 10 M 80 Y Y NSCLC 3.2 LUL 22.5 30.3 4 34.7 20.8 −7.6 M M M Adenoca TP TP TP 15 10 2.0 LUL 2.4 3.1 2 29.2 2.8 16.7 B M M Adenoca FN TP TP 16 11 M 51 Y Y SCLC 4.0 RLL 8.4 11.1 2 32.1 10.7 27.4 M M M SCLC TP TP TP 17 11 0.9 RUL — 1.1 1 — 1.0 — B B B SCLC FN FN FN 18 12 M 52 Y Y NSCLC 2.1 RUL 2.4 2.6 1 8.3 2.4 0 B M B Adenoca FN TP FN 19 13 M 71 Y — Colorectal 0.7 ML 0.8 1.5 2 87.5 1.5 87.5 B B B TN TN TN 20 13 0.7 RLL 1.7 2.2 3 29.4 1.8 5.9 B B B TN TN TN 21 14 M 73 Y — HD 1.8 RUL 1.2 1.3 1 8.3 1.2 0 B B B TN TN TN 22 15 F 73 Y — Colorectal 2.4 RLL 10.1 12.7 5 25.7 11.8 16.8 M M M TP TP TP 23 16 M 84 Y Y Epidermoid 1.6 RLL 3.2 4.8 3 50.0 4.2 31.2 M M M Epidermoid TP TP TP 24 17 F 50 Y — Ovarian 0.6 RUL 1.3 2.0 1 53.8 1.7 30.8 B B B TN TN TN 25 18 M 58 Y — Renal 0.8 RUL 0.5 2.3 2 360.0 2.3 360.0 B B B Negative TN TN TN 26 18 1.0 RUL 1.2 3.2 1 166.7 3.0 150.0 B M M Negative TN FP FP 27 18 2.0 RUL 1.8 2.6 4 53.8 2.4 33.3 B M B Negative TN FP TN 28 18 0.8 ML 0.4 0.4 — — — — B B B Negative TN TN TN 29 19 M 73 Y — Colorectal 2.0 LUL 3.0 5.3 6 76.7 4.9 63.3 M M M TP TP TP 30 19 0.9 LUL 1.2 2.0 1 66.7 1.5 25.0 B B B FN FN FN 31 19 0.7 RUL 0.8 1.3 1 62.5 1.1 37.5 B B B FN FN FN 32 20 M 65 — — 0.5 RUL 0.4 1.1 6 175.0 1.0 150.0 B B B TN TN TN 33 21 F 61 Y — Melanoma 1.3 Lingula 0.5 1.5 3 200.0 1.4 180.0 B B B TN TN TN 34 22 M 70 Y — Colorectal 0.9 LLL 2.8 3.4 2 21.4 3.1 10.7 M M M TP TP TP 35 23 M 70 Y — Colorectal 0.6 LLL 1.1 1.9 4 72.7 1.3 18.2 B B B FN FN FN 36 23 1.2 RLL 0.9 2.5 4 177.7 1.7 88.9 B M B FN TP FN 37 24 M 57 Y — Epidermoid 1.6 RLL 3.1 5.4 1 74.2 4.8 54.8 M M M TP TP TP 38 24 1.2 Lingula 2.0 2.7 3 35.0 2.4 20.0 B M B FN TP FN 39 25 F 61 Y — Endometrial 0.7 RUL 0.9 2.8 2 211.1 2.1 133.3 B M B FN TP FN 40 25 0.9 RUL 1.0 2.9 1 190.0 2.7 170.0 B M M FN TP TP 41 25 1.2 RLL 2.4 4.7 1 95.8 3.6 50.0 B M M FN TP TP 42 26 F 67 Y Y NSCLC 0.8 RUL 0.8 1.9 3 137.5 1.6 100.0 B B B TN TN TN 43 26 0.8 LLL 1.4 2.9 5 107.1 2.5 78.6 B M M TN FP FP 44 27 M 69 Y — Colorectal 1.2 LLL 0.8 1.1 1 37.5 0.9 12.5 B B B FN FN FN 45 27 1.0 RLL 1.5 1.7 1 13.3 1.5 0 B B B FN FN FN 46 28 M 41 Y — Testicular 1.5 RLL 1.4 2.4 5 71.4 2.1 50.0 B B B Negative TN TN TN 47 29 F 68 Y — Colorectal 0.8 RUL 1.1 2.5 2 127.3 2.1 90.9 B M B FN TP FN 48 29 1.0 RLL 1.2 3.4 2 183.3 2.3 91.7 B M B FN TP FN 49 29 0.7 RLL 1.2 3.2 2 166.6 2.5 108.3 B M M FN TP TP 50 30 F 79 Y — Renal 2.4 LLL 1.8 1.8 2 0 1.3 −27.8 B B B Mts FN FN FN 51 31 M 58 — — 2.2 RLL 10.9 14.8 1 35.8 13.1 20.2 M M M Epidermoid TP TP TP 52 32 F 57 Y — Cervix 1.2 RLL 1.7 2.3 2 35.3 2.1 23.5 B B B FN FN FN 53 33 M 81 Y — Colorectal 1.0 LUL 1.3 4.2 4 223.1 3.8 192.3 B M M FN TP TP 54 34 M 65 Y — Renal 1.6 LUL 1.2 1.4 6 16.7 1.2 0 B B B FN FN FN 55 35 M 61 Y — SCLC 2.2 RLL 4.7 10.2 4 117.0 8.8 87.2 M M M SCLC TP TP TP 56 36 M 62 Y — Larynx 4.7 RUL 18.6 21.6 3 16.1 20.4 9.7 M M M Positive TP TP TP 57 37 M 80 — — 2.4 RUL 2.7 5.2 3 92.6 4.8 77.8 M M M FP FP FP Les = lesion; Pt = patient; NB = neoplastic background; LC = lung cancer; Hy = histopathology; Diam = diameter; BB = best bin; Dif = difference; AG = average gated; NSCLC = non–small cell lung cancer; SCLC = small cell lung cancer; HD = Hodgkin disease; RUL: right upper lobe; LUL = left upper lobe; RLL = right lower lobe; LLL = left lower lobe; ML = middle lobe; B = benign; M = malignant; Mts = metastases; adenoca = adenocarcinoma; TN = true negative; FP = false positive; TP = true positive; FN = false negative.
3D Best-bin 4D Index (%) Total >1 cm ≥1.5 cm AG 4D total Total >1 cm ≥1.5 cm Sensitivity 37.8 52.2 68.4 51.3 70.3 79.2 84.2 Specificity 95 90 83.3 75 70 66.7 50 Positive predictive value 93 92.3 92.9 79.2 81.2 90.5 84.2 Negative predictive value 45 45 45.4 45.4 56 54.5 50 Accuracy 57.9 63.6 72 59.6 70.2 75.7 76 AG = average gated.
Mean SUVmax ± SD SUVmax percentage difference ± SD Lesion location Lesion distribution 3D BB 4D AG 4D 3D vs. BB 4D 3D vs. AG 4D RUL 17 2.29 ± 4.28 3.45 ± 4.78 3.17 ± 4.53 98.60 ± 99.19 84.37 ± 95.08 LUL 13 4.82 ± 6.84 6.61 ± 8.83 5.48 ± 6.83 51.48 ± 56.92 30.62 ± 52.03 RLL 15 3.63 ± 3.33 5.71 ± 4.32 4.96 ± 4.02 79.86 ± 59.25 47.42 ± 34.72 LLL 6 2.59 ± 2.64 3.49 ± 3.44 3.08 ± 3.44 41.86 ± 36.23 17.08 ± 32.28 Lingula 4 1.35 ± 0.65 2.05 ± 0.55 1.72 ± 0.47 77.97 ± 81.40 54.17 ± 84.34 ML 2 0.60 ± 0.28 0.95 ± 0.78 0.75 ± 1.06 43.75 ± 61.87 −6.25 ± 132.58 RUL = right upper lobe; LUL = left upper lobe; RLL = right lower lobe; LLL = left lower lobe; ML = middle lobe; BB = best bin; AG = average gated.





{kind=link}
{kind=link}
{kind=link}
{kind=link}