


Abstract
This study, which was based on a large series of consecutive patients imaged by 111In-pentetreotide SPECT for a neuroendocrine tumor, evaluated variability in reconstruction parameters in relation to patient body weight and the body region imaged, looking for the possibility of standardizing such parameters. Methods: One hundred twenty-four patients underwent 111In-pentetreotide scintigraphy: 4- and 24-h whole-body and planar scans and a 24-h SPECT examination. All patients were injected with 140–150 MBq of 111In-pentetreotide at least 1 wk after somatostatin analogs had been discontinued. SPECT images were systematically acquired at the levels of the head, chest, and abdomen. SPECT was performed using a dual-head γ-camera with medium-energy collimators, step-and-shoot method, no circular orbit, a 64 × 64 matrix, and 30 s per view for a total of 64 views. Two reconstruction procedures were compared: the iterative method using 10 iterations and the filtered backprojection method using a Butterworth filter with different cutoffs and orders. Results: Optimal SPECT images were obtained by applying the Butterworth filter. The reconstruction parameters could be standardized for the head and chest but were more variable for the abdomen, mainly because 111In-pentetreotide is physiologically trapped in different intestinal areas and varies over time, especially in the liver, spleen, bowel, and urinary tract. Conclusion: Filtered backprojection using a Butterworth filter appears adequate for standardizing the reconstruction parameters for 111In-pentetreotide SPECT of the head and chest. Processing of abdominal images is more operator-dependent. A 150-MBq dose of 111In-pentetreotide is recommended when planning multiple SPECT acquisitions in the same patient.
In recent years, SPECT has gained an important role in scintigraphic evaluations because it is accurate and allows precise localization of the depth of radioactive lesions. At present, SPECT studies using radiotracers labeled with 99mTc-pertechnetate are well standardized, mainly because the radioisotope is characterized by optimal energy and high-statistic count rates for acquisitions with currently available γ-cameras (1,2). In contrast, the choice of reconstruction parameters for medium-energy radioisotopes such as 111In is more difficult, mainly because they are characterized by a relatively low-statistic count rate (3,4).
This study, which was based on a large series of consecutive patients imaged by 111In-pentetreotide SPECT for a neuroendocrine tumor, evaluated variability in reconstruction parameters in relation to patient body weight and the body region imaged, looking for the possibility of standardizing such parameters.
MATERIALS AND METHODS
At our center from January 2005 to December 2006, 124 consecutive patients affected by a clinically and biochemically proven neuroendocrine tumor were enrolled in the study. All patients were injected with 140–150 MBq of 111In-pentetreotide at least 1 wk after somatostatin analogs had been discontinued and underwent 4- and 24-h whole-body and spot planar imaging. Moreover, a 24-h SPECT acquisition of the head, chest, and abdomen was also systematically obtained.
The SPECT images were acquired on a dual-head γ-camera (E-CAM; Siemens) using medium-energy collimators, a step-and-shoot acquisition protocol with no circular orbit, a 64 × 64 matrix, and 30 s per view for a total of 64 views. Two different reconstruction procedures were compared: first, an iterative method using ordered-subset expectation maximization (OSEM) with 10 iterations, like the method used in some previous studies on 99mTc-technetium–labeled compounds (5); and second, filtered backprojection using a conventional technique previously described (6), with application and comparison of a variety of commercially available filters.
Scintigraphic images were examined in a masked fashion by 2 skilled nuclear medicine physicians. In cases of discrepancy, the diagnosis was reached by consensus.
Among the different reconstruction protocols used, we found the Butterworth filter to be most satisfactory in regard to spatial resolution, contrast, and image definition, producing a global improvement in image quality. Different orders and cutoffs were applied using this filter.
The patients were divided into 2 groups according to body weight (49 patients weighed more than 70 kg; 65 weighed 70 kg or less), and the SPECT images of the 3 body regions (head, chest, and abdomen) of each patient were compared.
RESULTS
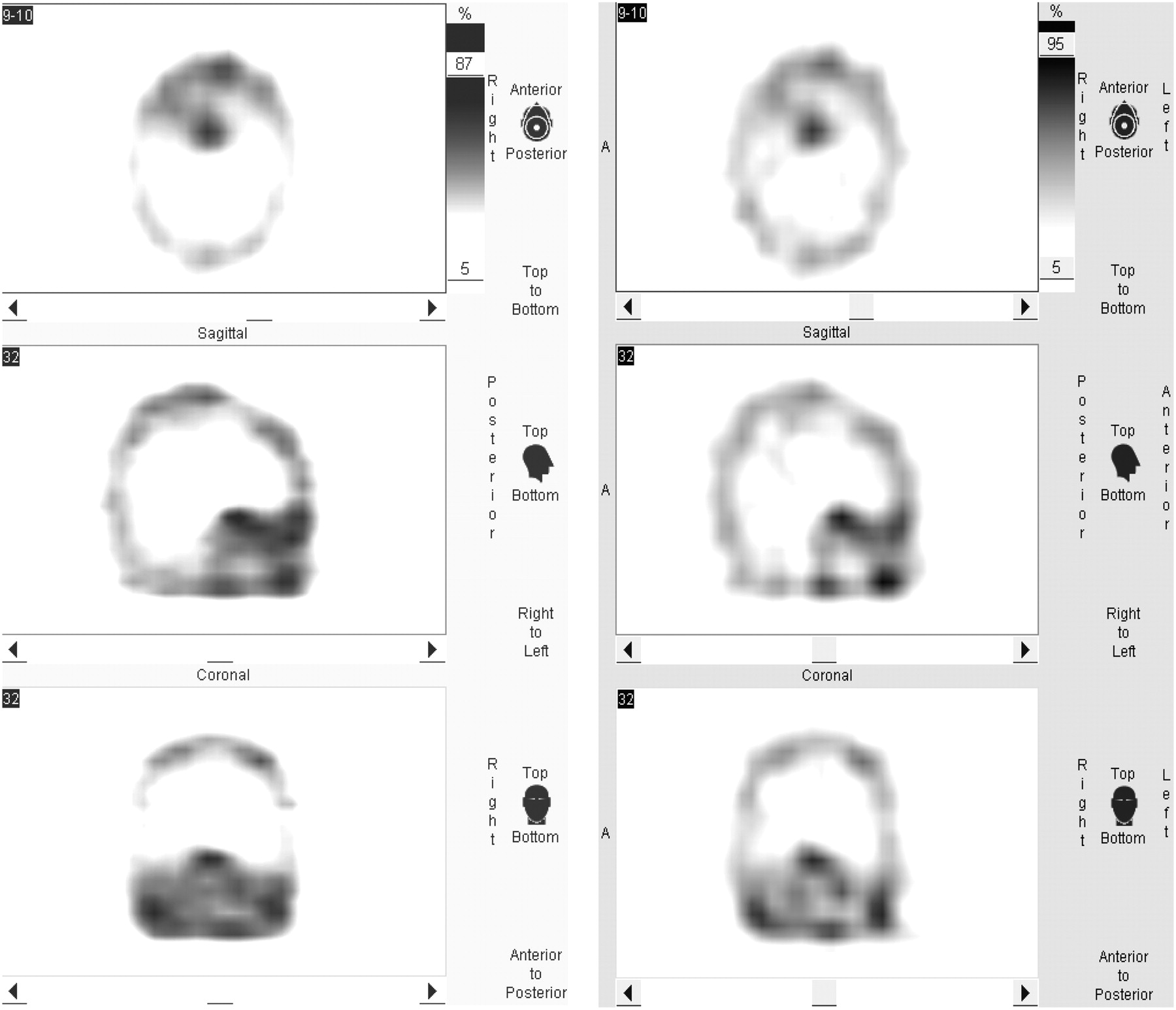
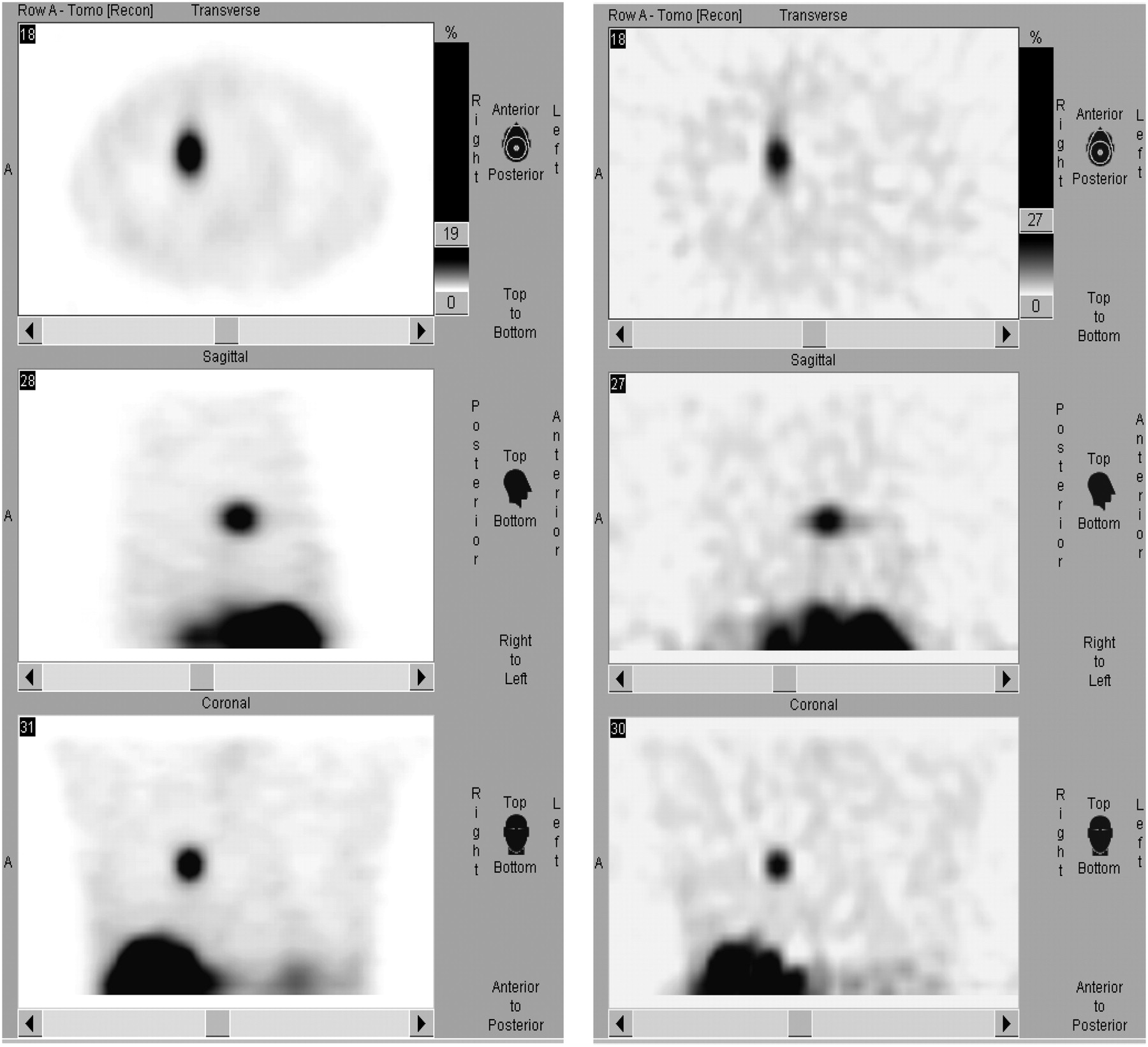
Table 1 summarizes our results, and Figures 1–3⇓⇓ show examples of head, chest, and abdominal images obtained using the iterative and filtered backprojection methods. Image shape seemed slightly smoother with the iterative method, whereas the global quality of SPECT images was better defined with filtered backprojection with the Butterworth filter.
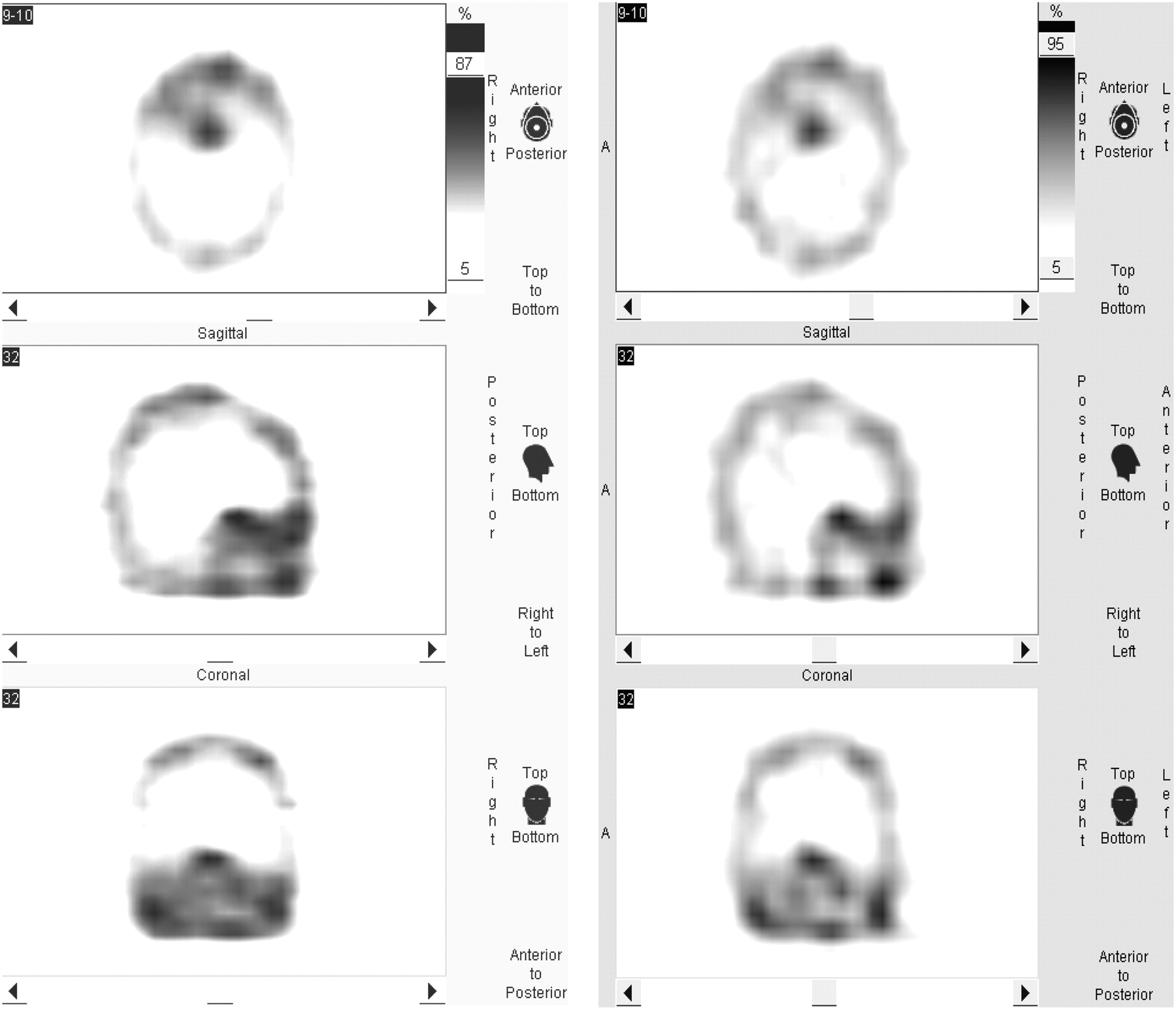
SPECT of head in patient with pituitary adenoma. Body weight was 74 kg. (Left) Reconstruction by OSEM iterative method (from top to bottom: axial, sagittal, and coronal views). (Right) Reconstruction by filtered backprojection using Butterworth filter, with cutoff of 0.35 and order of 8.
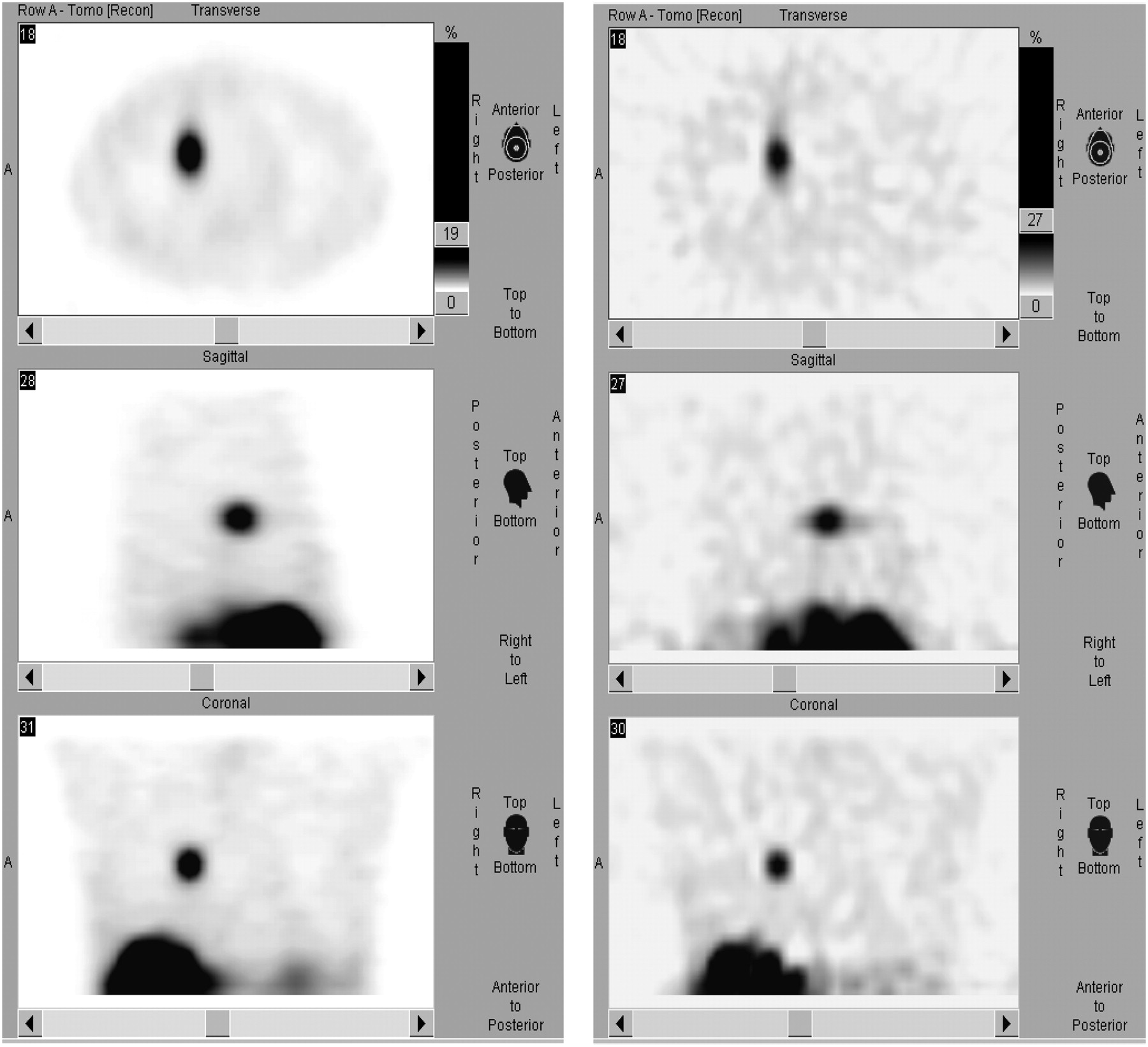
SPECT of chest in patient with typical bronchial carcinoid. Body weight was 68 kg. (Left) Reconstruction by OSEM iterative method (from top to bottom: axial, sagittal, and coronal views). (Right) Reconstruction by filtered backprojection using Butterworth filter, with cutoff of 0.40 and order of 9.

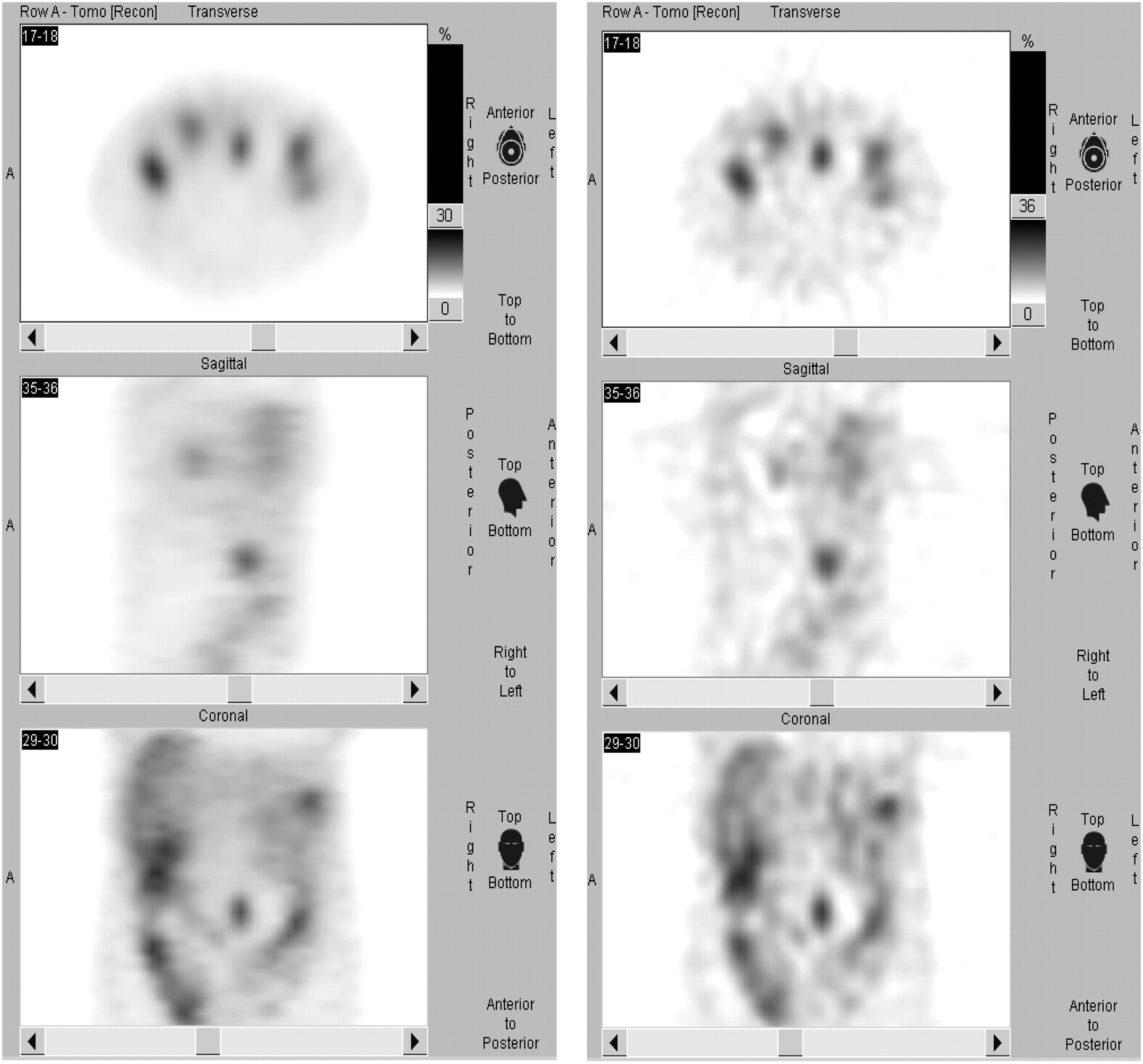
SPECT of abdomen in patient with ileal VIPoma (left periumbilical region). Body weight was 72 kg. (Left) Reconstruction by OSEM iterative method (from top to bottom: axial, sagittal, and coronal views). (Right) Reconstruction by filtered backprojection using Butterworth filter, with cutoff of 0.65 and order of 9.
111In-Pentetreotide SPECT Reconstruction Parameters in Relation to Body Weight and Body Region
DISCUSSION
Our analysis of a large group of homogeneously studied patients showed that filtered backprojection using a Butterworth filter produced images of better resolution than did the iterative method. With the Butterworth filter, the reconstruction parameters were easily standardized for the head and chest but were variable for the abdomen, especially in patients weighing more than 70 kg. This finding is explained by the presence of organs and tissues in the abdomen (such as the liver, spleen, bowel, and kidneys) characterized by moderate to high physiologic 111In-pentetreotide uptake (3,4). Some investigators believe that a late, 72-h, SPECT acquisition may partly overcome these interfering artifacts (7).
Regarding our finding that filtered backprojection using a Butterworth filter produced better images than did the OSEM iterative method, it has been reported that, for SPECT images with low count rates, the iterative method may ameliorate image quality (especially the shape of the lesion), providing smoother images (8). On the other hand, we obtained more defined SPECT images through filtered backprojection using a Butterworth filter, as might be explained by our injecting a relatively higher dose of 111In-pentetreotide—up to 150 MBq per patient—than has been used in other reported studies. Of course, a higher radiotracer dose is likely to produce a higher counting rate.
Thus, our data show that, in clinical practice, filtered backprojection using a Butterworth filter appears to be a good image-processing method for multiple (head, chest, and abdomen) 111In-pentetreotide SPECT examinations in the same patient.
Reconstruction parameters, although easily standardized for head and chest images, are not so easily standardized for images of the abdomen, where there are many time-related interfering factors. Thus, in the case of abdominal images, reconstruction parameters can vary widely and depend on the skill of the operator.
CONCLUSION
Filtered backprojection using a Butterworth filter appears adequate for standardizing reconstruction parameters for 111In-pentetreotide SPECT of the head and chest. Processing of abdominal images is more operator-dependent. For a triple-SPECT examination (head, chest, and abdomen) in the same patient, administration of a 150-MBq dose of 111In-pentetreotide is recommended.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 2, 2007.
- Accepted for publication May 7, 2007.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.