


Abstract
99mTc-labeled red blood cell scintigraphy is a powerful detection and localization tool that may be confounded by false-positive and false-negative findings. Subtraction scintigraphy has been used in the evaluation of acute lower gastrointestinal tract hemorrhage (LGIH) to reduce the impact of interpretive confounders. The aim of this investigation was to evaluate the cost-effectiveness of the addition of subtraction scintigraphy in the evaluation of patients with acute LGIH. Methods: The clinical phase of this research was a retrospective clinical study with a repeated-measures design including randomized control and experimental groups. A total of 49 patient studies were included in the sample. Studies were randomized and interpreted by 4 independent physicians. Decision-tree analysis was used to model direct costs and the potential risks of procedures for 2 diagnostic strategies for patients with acute LGIH: conventional scintigraphy alone and conventional scintigraphy combined with subtraction scintigraphy. The transition probabilities (or branching fraction at each decision node) for scintigraphy were based on the clinical results of this investigation. All other transition probabilities were derived from previously cited data. Results: Combining subtraction techniques with conventional scintigraphy reduced the overall costs of procedures for patients with acute LGIH by $74 per patient and reduced deaths by 17.6% and complications by 15.7%. For conventional scintigraphy alone, 8.8% of patients presenting for scintigraphic evaluation of acute LGIH would undergo unnecessary angiograms, and 2.8% would have unnecessary surgery. These figures were reduced to just 5.4% and 1.8%, respectively, with the addition of subtraction scintigraphy. Conclusion: The use of subtraction scintigraphy as an adjunct to conventional scintigraphy for patients with acute LGIH may provide both cost and outcome benefits.
Despite the difficulties confronting the diagnostic evaluation of acute lower gastrointestinal tract hemorrhage (LGIH), accurate localization of the site of bleeding is crucial for treatment and case management (1,2). Although the diagnostic evaluation of acute LGIH has improved significantly over the last 25 y, there is currently no gold standard because of the intermittent nature of the bleeding (2–4). 99mTc-labeled red blood cell (RBC) scintigraphy is a powerful detection and localization tool that may be confounded by false-positive and false-negative findings.
Subtraction scintigraphy has been used in the evaluation of acute LGIH (5). Subtraction scintigraphy should allow the elimination of background activity, providing high target-to-background images of the extravasated blood. In short, a dataset that theoretically offers the advantages of both conventional 99mTc-sulfur colloid scintigraphy and 99mTc-labeled RBC scintigraphy is produced (5).
The aim of this investigation was to compare the cost-effectiveness of interpretation of conventional scintigraphy with that of conventional scintigraphy combined with subtraction scintigraphy in the evaluation of patients with acute LGIH.
MATERIALS AND METHODS
The clinical phase of this research was a retrospective clinical study with a repeated-measures design including randomized control and experimental groups. A total of 49 patient studies were included in the sample. Acquisition parameters for all datasets included a 128 × 128 matrix and a continuous dynamic acquisition of 60 s per frame. Studies were generally performed with RBCs labeled with 99mTc in vitro by use of a commercially available kit.
The 49 original raw patient datasets were displayed conventionally without subtraction (conventional scintigraphy [CS]), with reference subtraction scintigraphy (RSS), and with alternate sequential subtraction scintigraphy (ASSS). Studies were randomized and interpreted by 4 independent physicians initially as CS data only. The CS, RSS, and ASSS studies were subsequently combined and randomized for reinterpretation. Although studies were randomized within each of the 2 pools of data, CS data were reported before combined CS and subtraction data to remove possible bias. The clinical phase of this research was approved by the Charles Sturt University Ethics in Human Research Committee.
RSS
In an acquisition with n consecutive image frames and with each individual image frame given by F(f), where f equals (1,2,3,………….,n), any subtracted image in the sequence is given by the following equation: For example,
For example,
ASSS
In an acquisition with n consecutive image frames and with each individual image frame given by F(f), where f equals (1,2,3,………….,n), any subtracted image in the sequence is given by the following equation: For example,
For example,
Decision-Tree Analysis
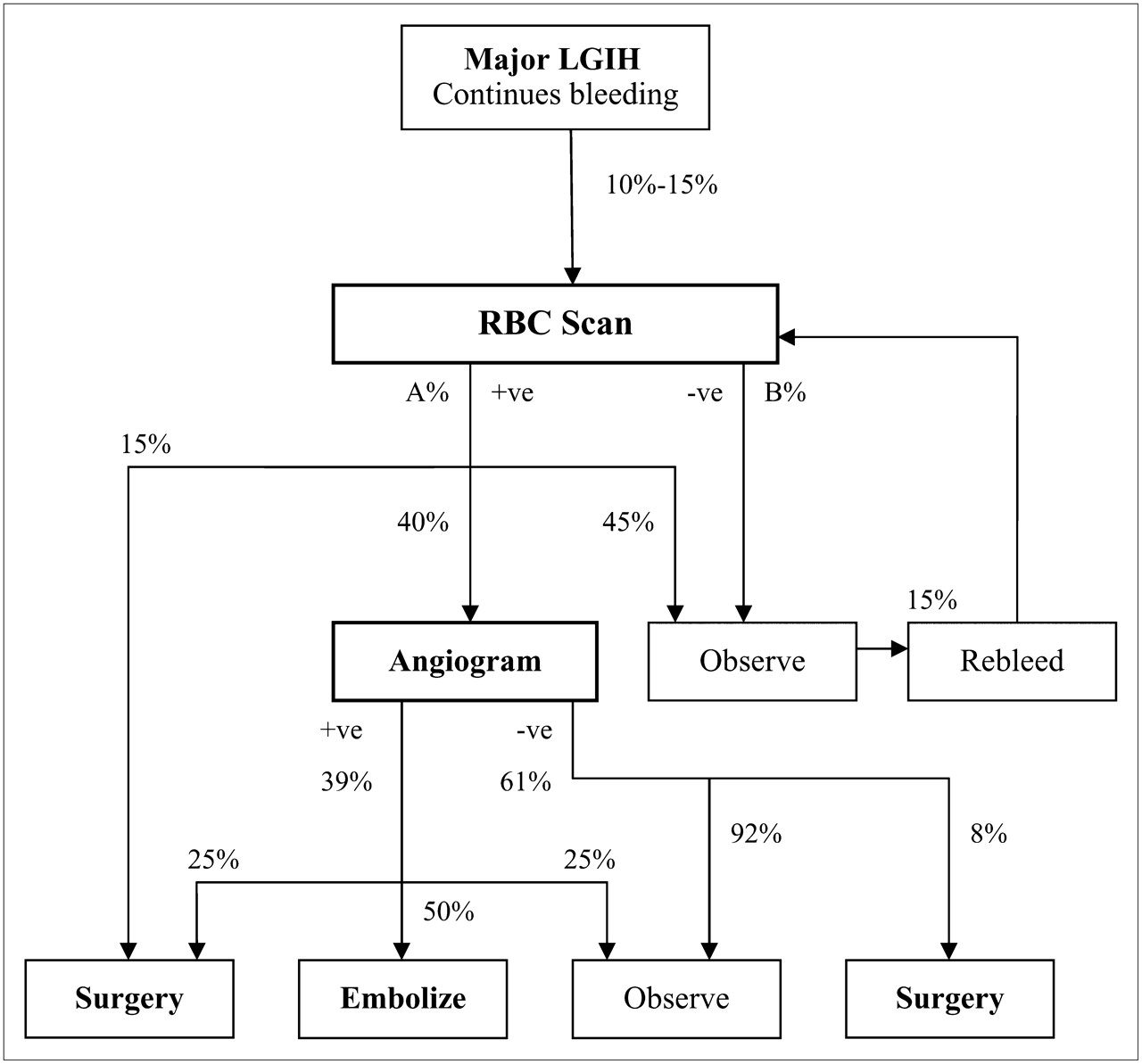
Decision-tree analysis was used to model direct costs and the potential risks of procedures for 3 diagnostic strategies for patients with acute LGIH: CS alone, CS combined with subtraction scintigraphy RSS and ASSS, and CS combined with ASSS only. All diagnostic strategies were based on the diagnostic algorithm depicted in Figure 1.

Composite diagnostic algorithm for patients with LGIH. A% and B% represent alternative diagnostic strategies. +ve = positive; −ve = negative.
The decision-tree analysis was based on a hypothetical population of 3,000 patients presenting for scintigraphic evaluation of acute LGIH. Each of 3 diagnostic strategies was used to evaluate 1,000 randomly allocated patients with a homogeneous distribution of variables. The transition probabilities (A% and B% in Fig. 1) for scintigraphy were based on the clinical results outlined here. All other transition probabilities (branching fractions at decision nodes) were derived from previously cited data (Table 1). Complication rates and mortality rates were also derived from previously cited data (Table 1). Costs were estimated by use of the Australian Government Medicare Benefits Schedule (6) and are reported in Australian dollars. Table 1 and Table 2 provide an overview of the key information used in the decision-tree analysis and the cost-effectiveness analysis.
Summary of Data Used in Analysis
Summary of Clinical Results Used in Analysis
Several assumptions were made during this analysis. First, apart from the 15% of positive scintigraphy studies that led to surgery without angiography, the remaining positive scintigraphy studies all led to angiography. In theory, this scenario is entirely plausible, given the role of scintigraphy in directing patients to undergo angiography, although in practice as many as 45% of patients with positive scintigraphy studies are simply observed (20). Second, the analysis included a single iteration for cases recirculating in the diagnostic algorithm after an initial negative scintigraphy study. There seemed no tangible benefit of continuing this analysis (negative scintigraphy study–rebleed cycle) ad infinitum. Third, when complication rates and mortality rates were reported in the literature as ranges, with no obvious best value or most recent application, a conservative approach of using the lowest value was taken.
RESULTS
The mean age of the study population was 68.9 y (95% confidence interval: 64.0–73.9 y), with a range of 18.8–92.8 y and a median of 71.8 y. Women represented 61.2% (30/49) of the study population, and men represented 38.8% (19/49), although no statistically significant variation in the sex distribution was noted (P = 0.11). No statistically significant difference between the sexes was noted for mean age (P = 0.50). Just 7 patient studies (14.3%) were positive for gastrointestinal tract bleeding, as determined by expert panel consensus. The remaining 42 patient studies were not positive for active bleeding at detectable bleeding rates during the data acquisition.
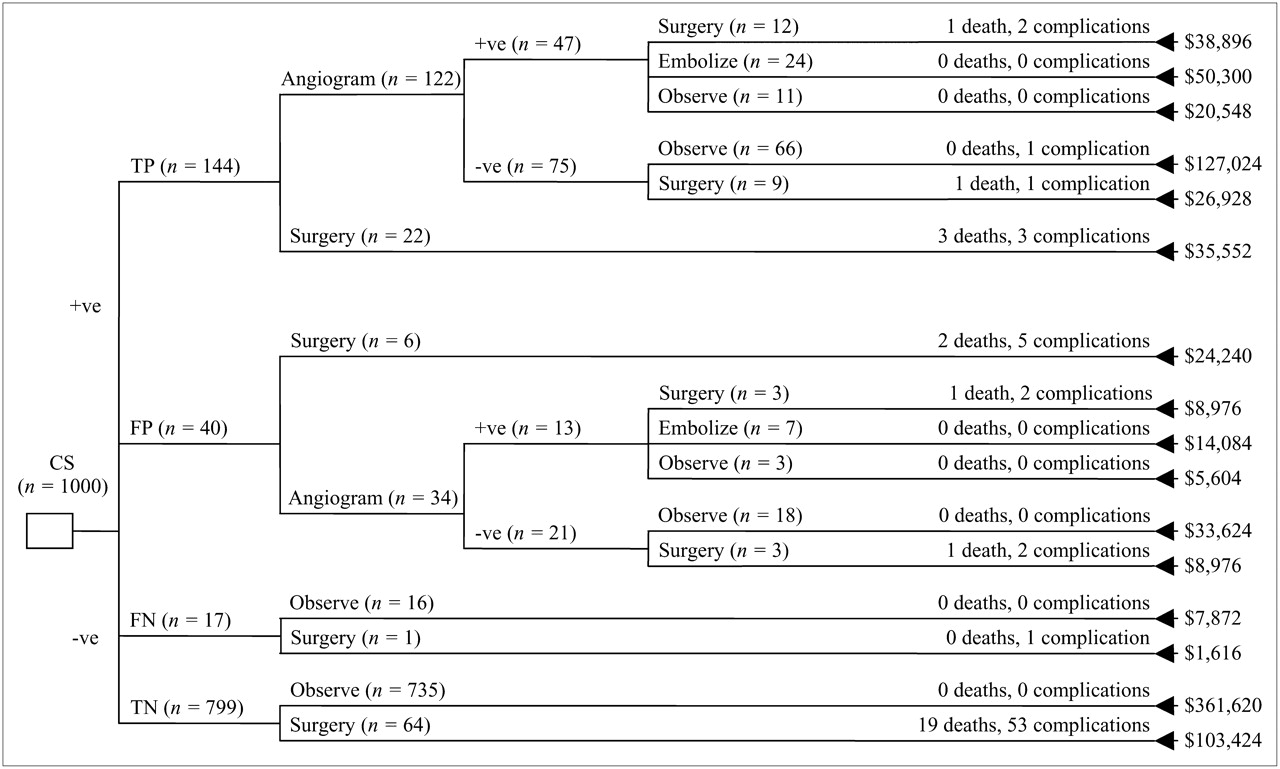
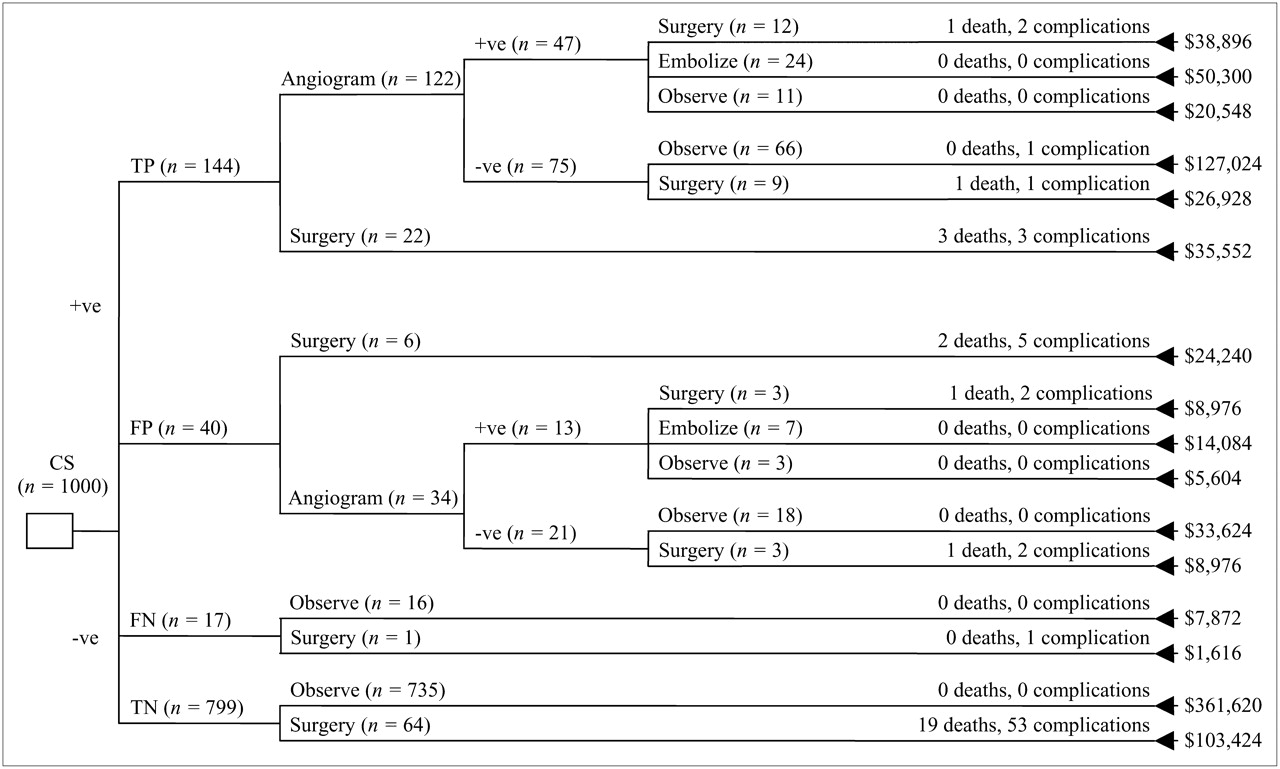
The decision-tree analysis for 1,000 patients evaluated with CS alone (Fig. 2) demonstrated totals of 34 deaths and 83 complications and a total cost of $943,128. Eighteen deaths and 49 complications were attributed to blind surgery (i.e., surgery performed without guidance from the results of a diagnostic procedure) being performed on patients with true-negative scintigraphy studies. Further complications were associated with blind surgery being performed on patients with false-negative scintigraphy studies. More importantly, 10 deaths and 25 complications were associated with unnecessary procedures being performed on patients with false-positive study results. These findings were associated with an additional cost burden of $157,256, which reflects the increase in per-patient cost from $492 (true-negative results) to $2,019 (false-positive results). The larger cohort with true-positive results had 6 deaths and 8 complications.

Decision-tree analysis for CS alone, with totals of 34 deaths and 83 complications and total cost of $943,128. FN = false-negative results; FP = false-positive results; TN = true-negative results; TP = true-positive results; +ve = positive; −ve = negative.
The decision-tree analysis for CS, RSS, and ASSS combined (Fig. 3) demonstrated totals of 28 deaths and 70 complications and a total cost of $869,284. Nineteen deaths and 53 complications were attributed to blind surgery being performed on patients with true-negative scintigraphy studies. CS, RSS, and ASSS combined reduced deaths in the group with false-positive results from 10 for CS alone to 4 for CS, RSS, and ASSS combined. Furthermore, a corresponding reduction in complications was noted for the group with false-positive results: from 25 to just 9. Although the cost per patient in the false-positive group changed only marginally, reflecting the effects of rounding to whole patient numbers, the total reduction in cost for patients with false-positive results was $112,428. The addition of subtraction techniques decreased the overall cost by $73,844 ($74 per patient).
Decision-tree analysis for CS, RSS, and ASSS combined, with totals of 28 deaths and 70 complications and total cost of $869,284. FN = false-negative results; FP = false-positive results; TN = true-negative results; TP = true-positive results; +ve = positive; −ve = negative.
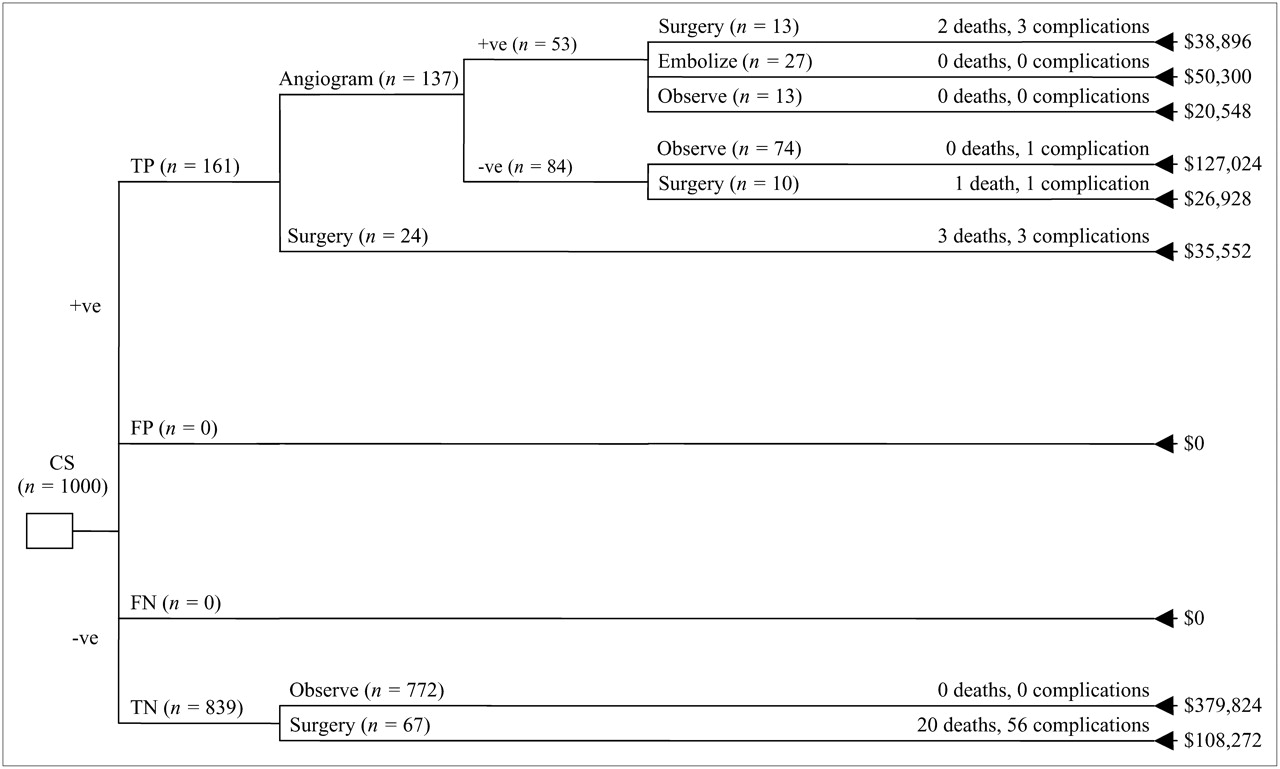
The decision-tree analysis for CS and ASSS combined, in which study results were considered positive only when ASSS provided supporting evidence (Fig. 4), demonstrated totals of 26 deaths and 64 complications and a total cost of $787,344. These changes reflected the elimination of false-positive findings and provided a cost saving over CS alone of $155,784 ($156 per patient).
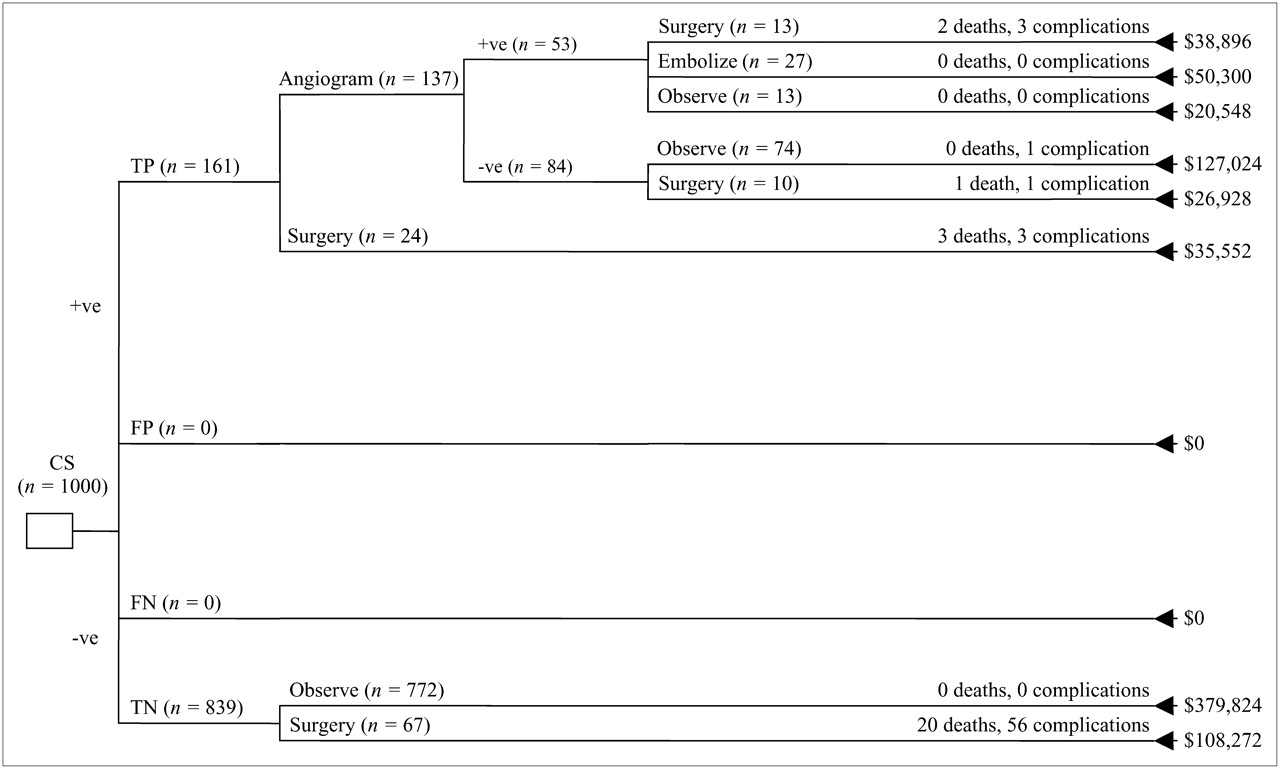
Decision-tree analysis for CS and ASSS combined, with totals of 26 deaths and 64 complications and total cost of $787,344. FN = false-negative results; FP = false-positive results; TN = true-negative results; TP = true-positive results; +ve = positive; −ve = negative.
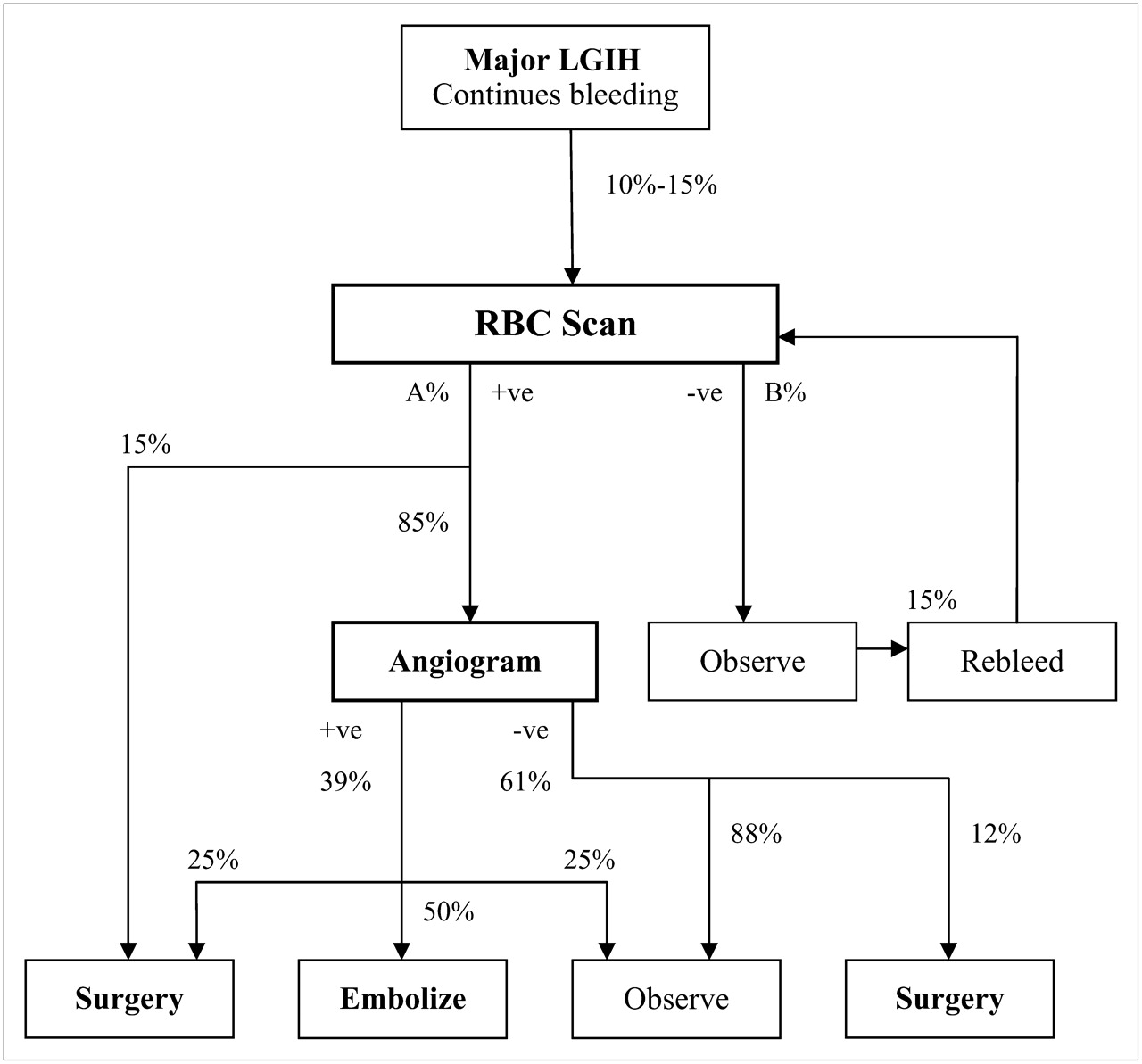
Sensitivity analysis is a technique used in economic analysis to assess the robustness of calculations. In cost-effectiveness analysis, sensitivity analysis repeats calculations on the basis of worst-case and best-case scenarios to determine whether the conclusions are valid within a broader clinical window. In this cost-effectiveness analysis, sensitivity analysis was used to assess the impact of the variability of proportions reported in Figure 1. The conservative nature of the original analysis virtually provides a worst-case scenario; however, some minor adjustments to proportions in the diagnostic algorithm might negatively affect the diagnostic integrity of scintigraphy (Fig. 5). A best-case scenario can be accomplished by being less conservative with the variables in Table 1. Table 3 provides a summary of the key variables used in the sensitivity analysis.
Composite diagnostic algorithm for patients with LGIH, with minor adjustments to proportions. A% and B% represent alternative diagnostic strategies. +ve = positive; −ve = negative.
Summary of Data Used in Sensitivity Analysis
The decision-tree analysis for 1,000 patients evaluated with CS alone as a worst-case scenario demonstrated totals of 28 deaths and 70 complications and a total cost of $757,588. Six deaths and 16 complications were associated with unnecessary procedures being performed on patients with false-positive study results. The worst-case scenario decision-tree analysis for CS, RSS, and ASSS combined demonstrated totals of 26 deaths and 67 complications and a total cost of $725,342. These data corresponded to no changes in deaths or complications in the group with false-positive results compared with that group evaluated with CS alone. The addition of subtraction techniques reduced the overall cost by $32,246 ($32 per patient). The worst-case scenario decision-tree analysis for CS and ASSS combined demonstrated totals of 25 deaths and 63 complications and a total cost of $692,480. These changes reflected the elimination of false-positive findings and provided a cost saving over CS alone of $65,108 ($65 per patient).
The decision-tree analysis for 1,000 patients evaluated with CS alone as a best-case scenario demonstrated totals of 38 deaths and 103 complications and a total cost of $943,128. Sixteen deaths and 34 complications were associated with unnecessary procedures being performed on patients with false-positive study results. The best-case scenario decision-tree analysis for CS, RSS, and ASSS combined demonstrated totals of 30 deaths and 83 complications and a total cost of $869,284. CS, RSS, and ASSS combined reduced deaths in the group with false-positive results from 16 for CS alone to 7 for CS, RSS, and ASSS combined. Furthermore, a corresponding reduction in complications was noted for the group with false-positive results: from 34 to just 11. The addition of subtraction techniques reduced the overall cost by $73,844 ($74 per patient). The best-case scenario decision-tree analysis for CS and ASSS combined demonstrated totals of 24 deaths and 75 complications and a total cost of $787,344. These changes reflected the elimination of false-positive findings and provided a cost saving over CS alone of $155,784 ($156 per patient).
DISCUSSION
The decision trees were burdened by large mortality and complication rates associated with blind surgery being performed for patients with true-negative scintigraphic findings. This finding highlights the role that subtraction scintigraphy might play in improving the negative predictive value of scintigraphy: reducing blind surgery. Nonetheless, the impact of subtraction scintigraphy in reducing the costs and consequences of case management when false-positive results are obtained is highlighted by this analysis.
Combining subtraction techniques with CS not only reduced the overall costs of procedures for patients with acute LGIH but also reduced mortality and morbidity. Combining CS, RSS, and ASSS reduced deaths by 6 (0.6%) and complications by 13 (1.3%) while providing a net saving of $73,844 over CS alone. Thus, subtraction scintigraphy for patients with acute LGIH provided a saving of $74 per patient while saving 6 lives or, on average, 69.6 life years. These data translate to a cost saving of $12,307 per life or $1,061 per life year.
Combining CS and ASSS reduced deaths by 8 (0.8%) and complications by 19 (1.9%) while providing a net saving of $155,784 over CS alone. Thus, ASSS for patients with acute LGIH provided a saving of $156 per patient while saving 8 lives or, on average, 92.8 life years. These data translate to a cost saving of $19,473 per life or $1,679 per life year.
These findings were shown to be robust under the scrutiny of sensitivity analysis, with subtraction scintigraphy offering cost, complication, and mortality reductions even in the worst-case scenario (Table 4). The sensitivity analysis indicated that, with respect to cost reductions at least, the cost-effectiveness of CS, RSS, and ASSS combined was close to that of the best-case scenario, whereas that of CS and ASSS combined was close to that of the worst-case scenario. Thus, the cost benefit of the former may not be fully realized in a clinical model, whereas the latter may afford greater cost savings in a clinical model. It should be noted that “best-case scenario” and “worst-case scenario” refer to the diagnostic integrity of scintigraphy rather than patient outcomes.
Results of Sensitivity Analysis of Decision-Tree Data Obtained with Various Subtraction Techniques
In the cohort of patients modeled (clinical-phase data), 8.8% of the patients presenting for scintigraphic evaluation of acute LGIH would undergo unnecessary angiograms, and 2.8% would have unnecessary surgery. The former is associated with significant cost and radiation burdens, whereas the latter is associated with significant mortality and morbidity. Combining CS with RSS and ASSS in the clinical phase of this research allowed unnecessary angiograms to be reduced to just 5.4% of the cohort and unnecessary surgery to be reduced to just 1.8%. Exploiting the distinctive competencies of ASSS in collaboration with CS interpretation and eliminating potential false-positive findings associated with RSS eradicated unnecessary angiograms and surgery altogether. This strategy may introduce a small number of false-negative study results, although this possibility was not revealed in this evaluation. It should be noted that unnecessary surgery and angiography were defined by those procedures performed in cases in which false-positive results were obtained rather than simply those with negative outcomes.
CONCLUSION
This gastrointestinal tract hemorrhage study with 99mTc-labeled RBCs demonstrated that false-positive or false-negative findings may confound interpretation. False-positive findings may lead to a patient unnecessarily undergoing more expensive and higher-risk procedures. Generally, a cost-effectiveness analysis is used to make decisions about the implementation of strategies that add costs while justifying the additional costs with improved outcomes. In this study, subtraction scintigraphy not only improved outcomes but also reduced costs. Subtraction scintigraphy used as an adjunct to conventional scintigraphy for patients with acute LGIH may provide both cost and outcome benefits. Moreover, decision-tree analyses demonstrated the superior cost-effectiveness of CS and ASSS combined over CS alone and over CS, RSS, and ASSS combined. These data reflect the high rate of false-positive findings associated with RSS.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 26, 2006.
- Accepted for publication January 29, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.