


Abstract
The aim of this study was to see whether oral administration of 18F-FDG could be substituted—without significant loss of information—for intravenous injection of 18F-FDG in patients with difficult intravenous access of any cause, such as that often seen in cancer patients after many cycles of chemotherapy. Methods: PET after both oral and intravenous administration of 18F-FDG was performed on 2 healthy volunteers and 7 patients. An interval of 48 h was maintained between the oral administration and the intravenous administration. All scans were visually analyzed. Semiquantitative analysis of specific areas was done by calculating standardized uptake values (SUVs). Scanning was performed 60 min after intravenous tracer administration and 90 min after oral tracer administration. Results: All lesions seen after intravenous administration were visualized on the oral study as well. SUVs were lower on the oral study than on the intravenous study. Conclusion: Oral 18F-FDG can successfully be substituted for intravenous 18F-FDG in patients with difficult intravenous access. However, because of the large amount of 18F-FDG retained in the gut, careful interpretation will be required when disease of the gastrointestinal tract is being evaluated.
PET with 18F-FDG has become an important and well-established functional imaging modality over the past decade in the detection, staging, and monitoring of the response to chemotherapy of cancer. Increasingly, 18F-FDG PET has also been used in benign states, as in determining viable myocardium, evaluating neuropsychiatric conditions, and monitoring infections. Every center performing PET scans has experienced situations involving difficult intravenous access, particularly in patients receiving chemotherapy. An extravasated injection leads to a poor 18F-FDG concentration in tissue and consequently an unreadable scan. Repeated studies in patients with poor intravenous access often result in a multiplicity of unsatisfactory studies, which are a burden both on the patient and on the center doing the studies. Stray reports (1) have indicated that oral administration may meet the needs of PET imaging. We therefore undertook a study of a diversity of cases to determine whether the lesions detected after oral administration of 18F-FDG might be identical to those detected after intravenous administration and whether oral administration might thus be an adequate substitute for intravenous.
MATERIALS AND METHODS
Two healthy volunteers and 7 patients were evaluated by PET after both oral and intravenous administration of 18F-FDG. An interval of 48 h was maintained between the oral administration and the intravenous administration. Both healthy volunteers were male, but this selection was not intentional. Of the 7 patients, 4 were men and 3 were woman. They ranged in age from 18 to 60 y. Before undergoing 18F-FDG PET, all patients underwent a clinical examination, and all gave informed consent to participate. Pregnant and lactating women were excluded from the study.
PET scans were obtained on a dedicated whole-body scanner (Advance; GE Healthcare), using attenuation correction. All patients fasted for 6 h before the study. Image acquisition began 40–60 min after intravenous administration and 90 min after oral administration. In both cases, 370 MBq of 18F-FDG were administered. All patients had a blood glucose level of less than 140 mg/dL. All scans were visually analyzed. Semiquantitative analysis was done for specific areas by calculating standardized uptake values (SUVs).
RESULTS
Three of the 7 patients had a primary tumor in the lung, with metastatic lesions elsewhere. Two patients had non-Hodgkin's lymphoma and were being evaluated after treatment. One patient was being assessed for myocardial viability. The seventh patient had a solitary thyroid nodule.
Patient 1
A 59-y-old man with non–small cell cancer of the right lung underwent 18F-FDG PET for pretreatment evaluation (Fig. 1). The intravenous study showed an area of intense 18F-FDG uptake in the mid zone of the right lung and 2 ipsilateral hilar lymph nodes. The oral study, done 2 days later, showed both the primary lesion and the ipsilateral hilar lymph nodes. However, the SUVs of lesions on the oral study were about 20%–30% lower than those on the intravenous study.
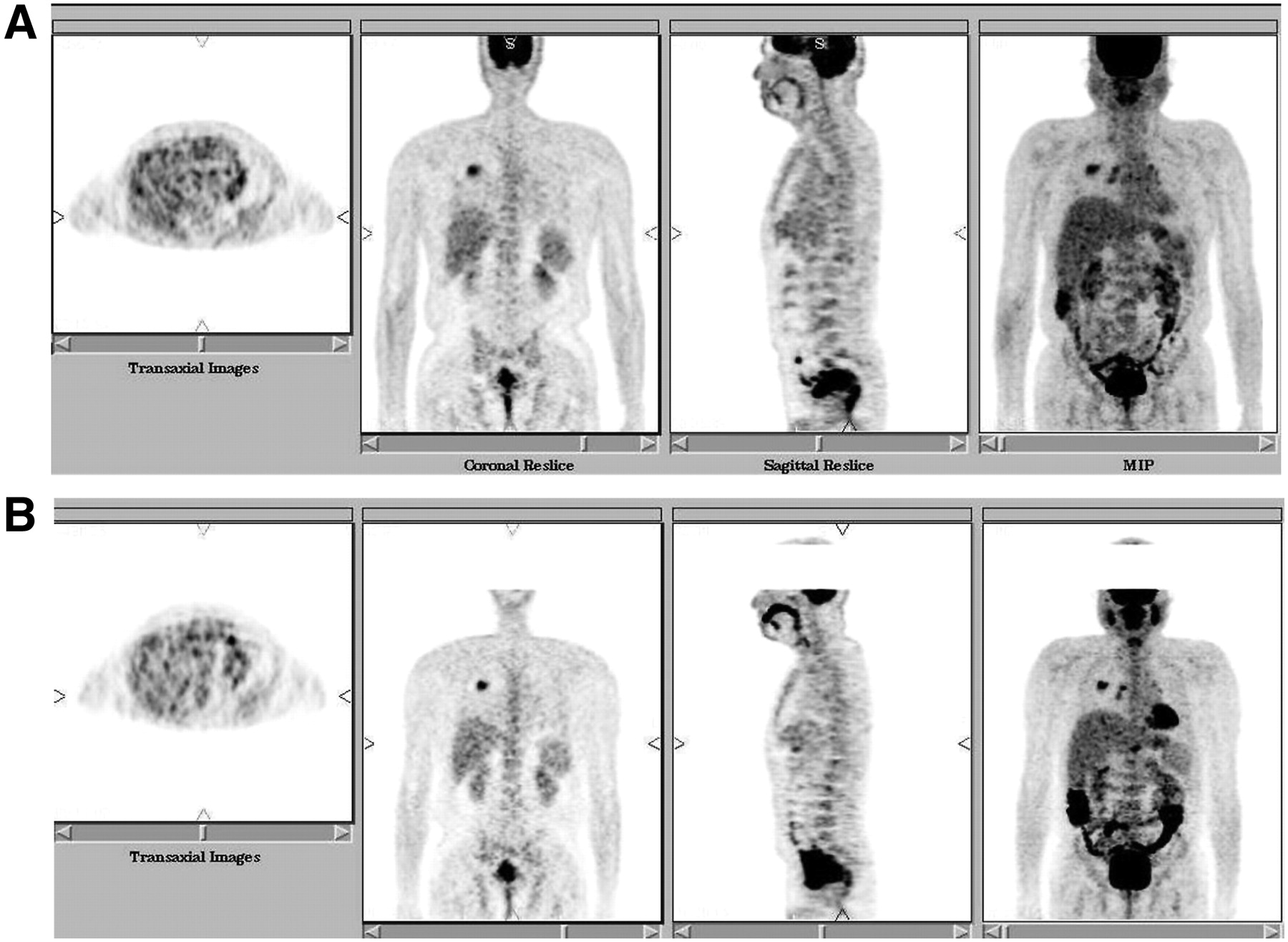
Patient 1, 59-y-old man with right lung carcinoma. Both intravenous (A) and oral (B) studies show right-mid-zone mass and right hilar lymph node. MIP = maximum intensity projection.
Patient 2
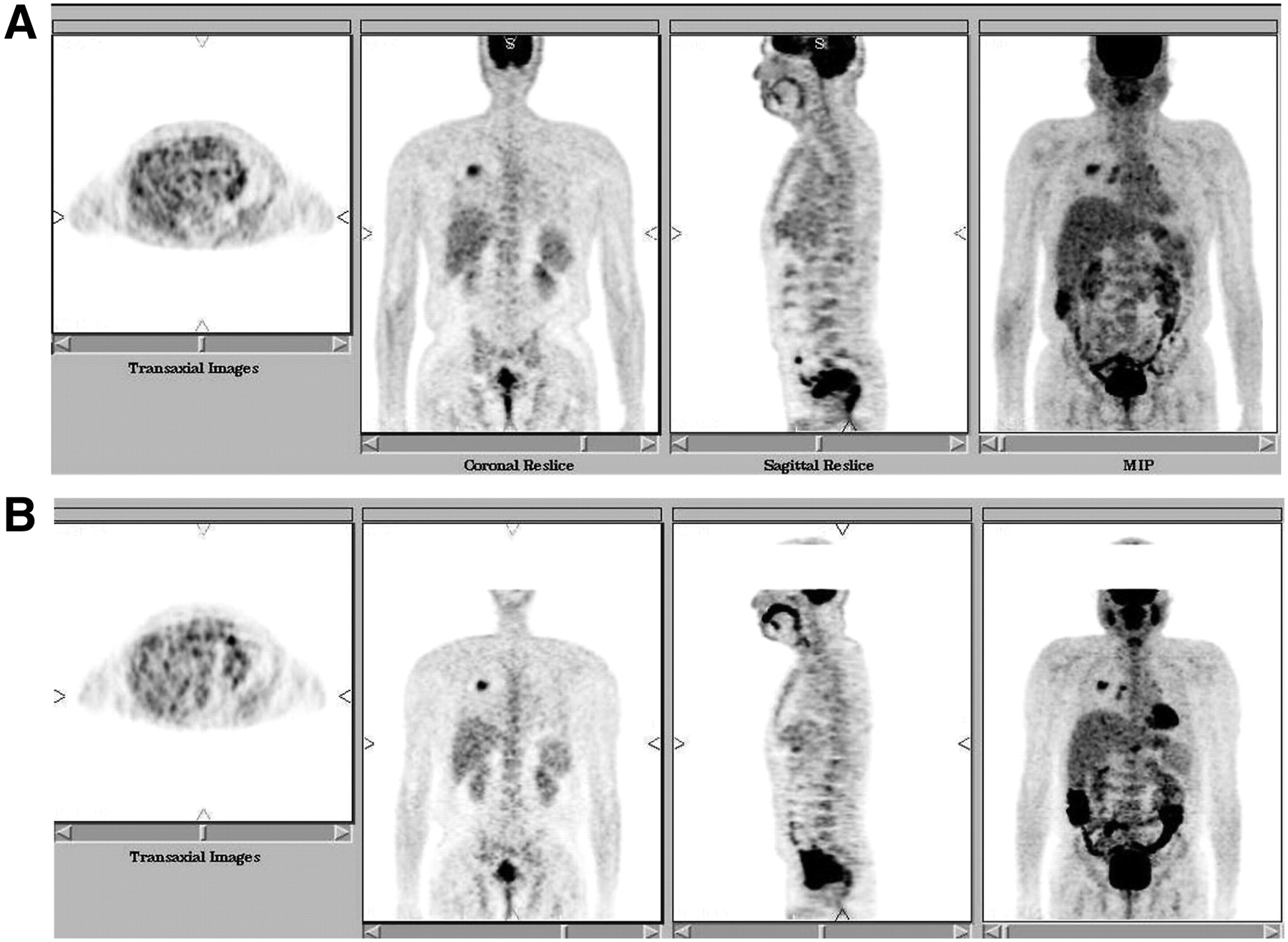
A 60-y-old man with carcinoma of the right lung showed, on the intravenous study, a large mass with intense 18F-FDG uptake in the upper zone of the right lung (Fig. 2). In addition, multiple areas of uptake were seen in the vertebrae, right shoulder, iliac bone, and both femurs. The oral study showed all these lesions, except an area in the left cubital fossa seen on the intravenous study because of extravasation of 18F-FDG. The SUVs of the lesions on the oral study were 50%–60% of those on the intravenous study.
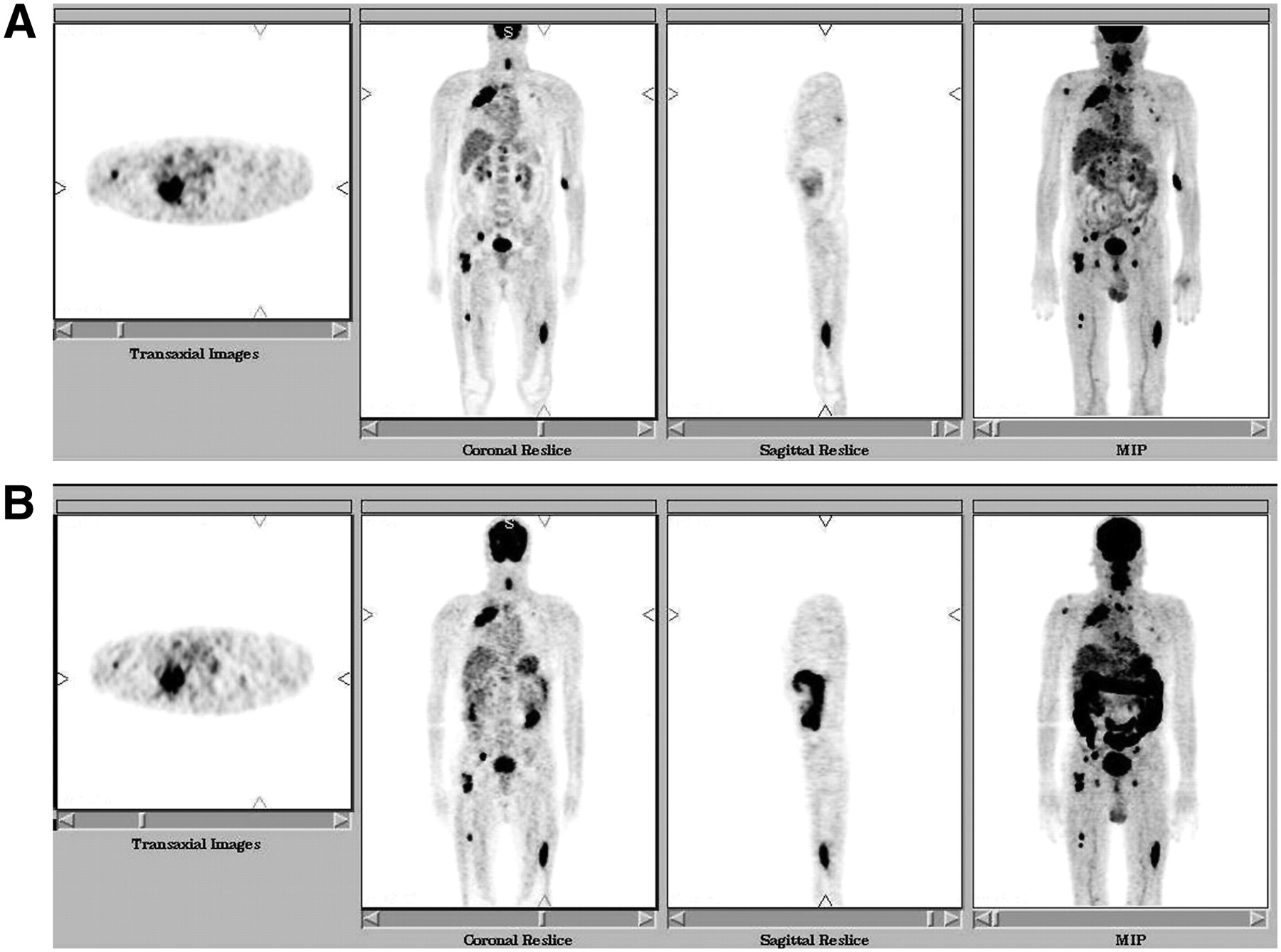
Patient 2, 60-y-old man with right lung carcinoma and multiple skeletal metastases. Both intravenous (A) and oral (B) studies show right-upper-lobe lesion, with metastases in vertebrae, right shoulder, pelvic bone, and both femurs. MIP = maximum intensity projection.
Patient 3
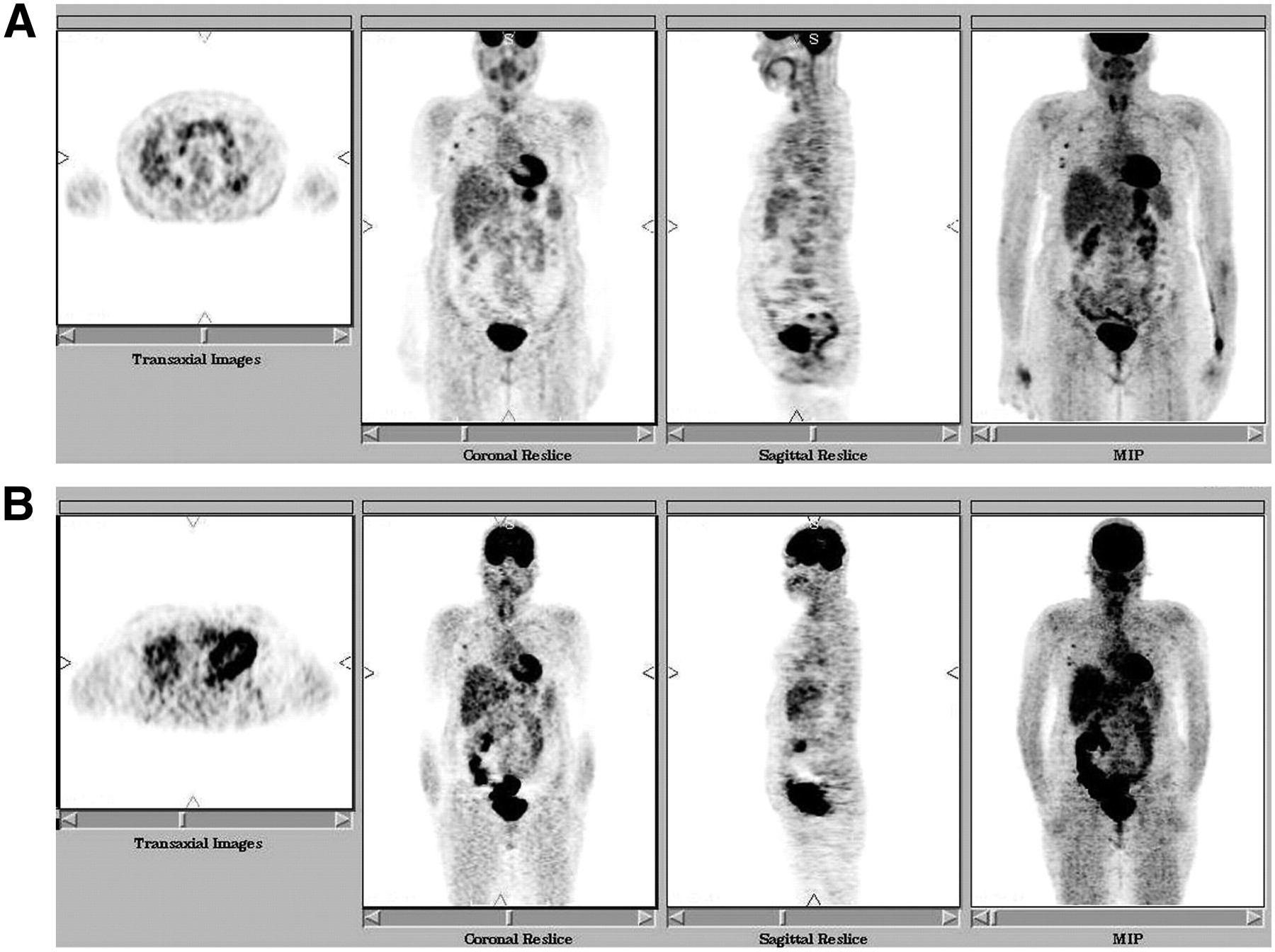
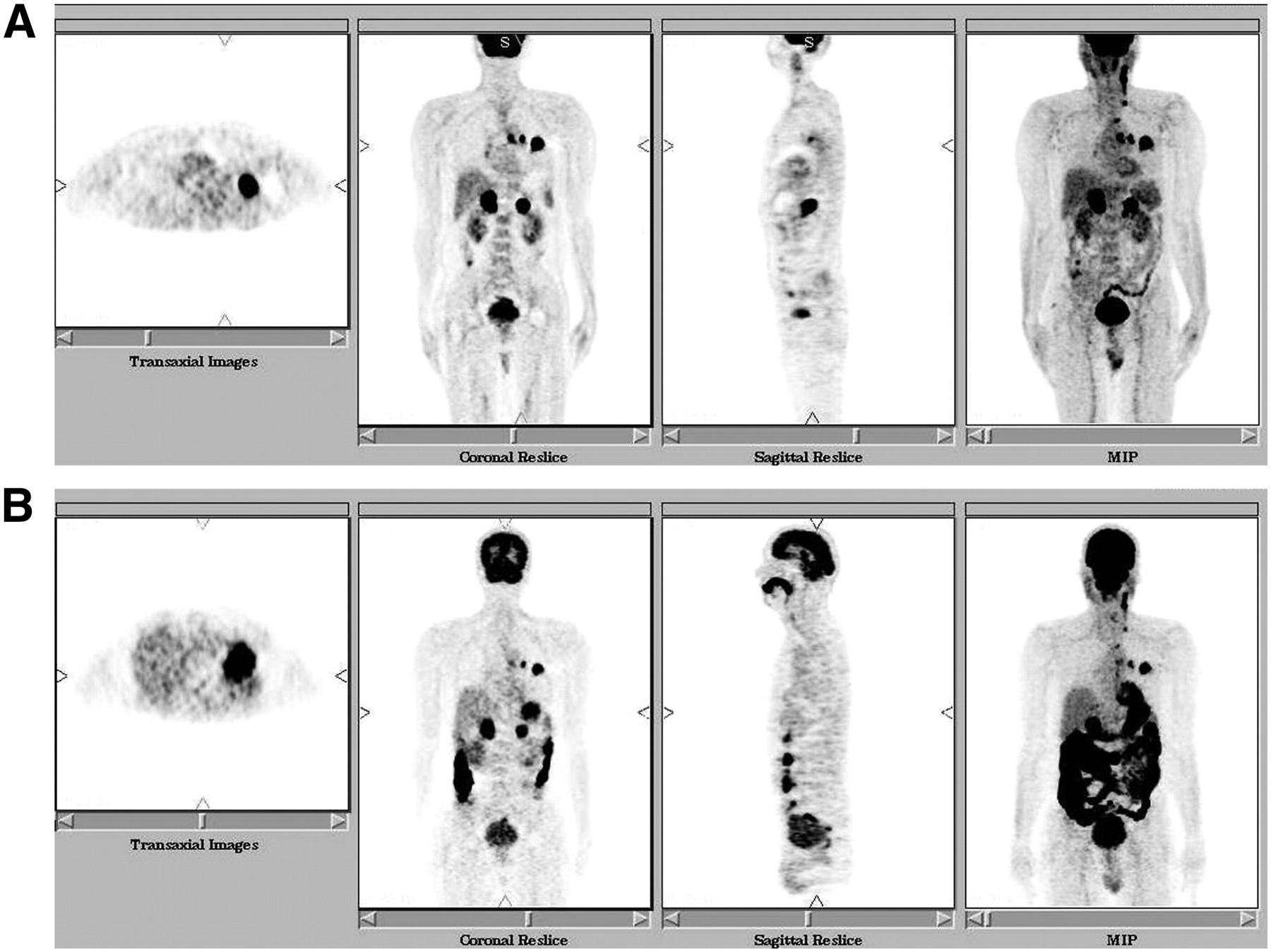
In a patient with carcinoma of the left lung and metastases to both adrenals, the intravenous study showed the primary site and intense 18F-FDG uptake in the left lung (Fig. 3). Hypermetabolic areas were seen in the mediastinal and ipsilateral hilar lymph nodes. Both adrenal glands also showed intense 18F-FDG uptake. The oral study showed the hypermetabolic areas in the left lung, mediastinal and hilar lymph nodes, and both adrenal glands. The adrenal metastases were clearly seen on the coronal slice but were difficult to see on the maximum-intensity-projection image because of extensive tracer in the gastrointestinal tract.
Patient 3, 47-y-old man with left lung carcinoma. Also seen are mediastinal lymph nodes and bilateral adrenal metastases. The lesions match on both intravenous (A) and oral (B) studies. MIP = maximum intensity projection.
Patient 4
In a patient with non-Hodgkin's lymphoma after treatment, both the intravenous study and the oral study showed no abnormalities.
Patient 5
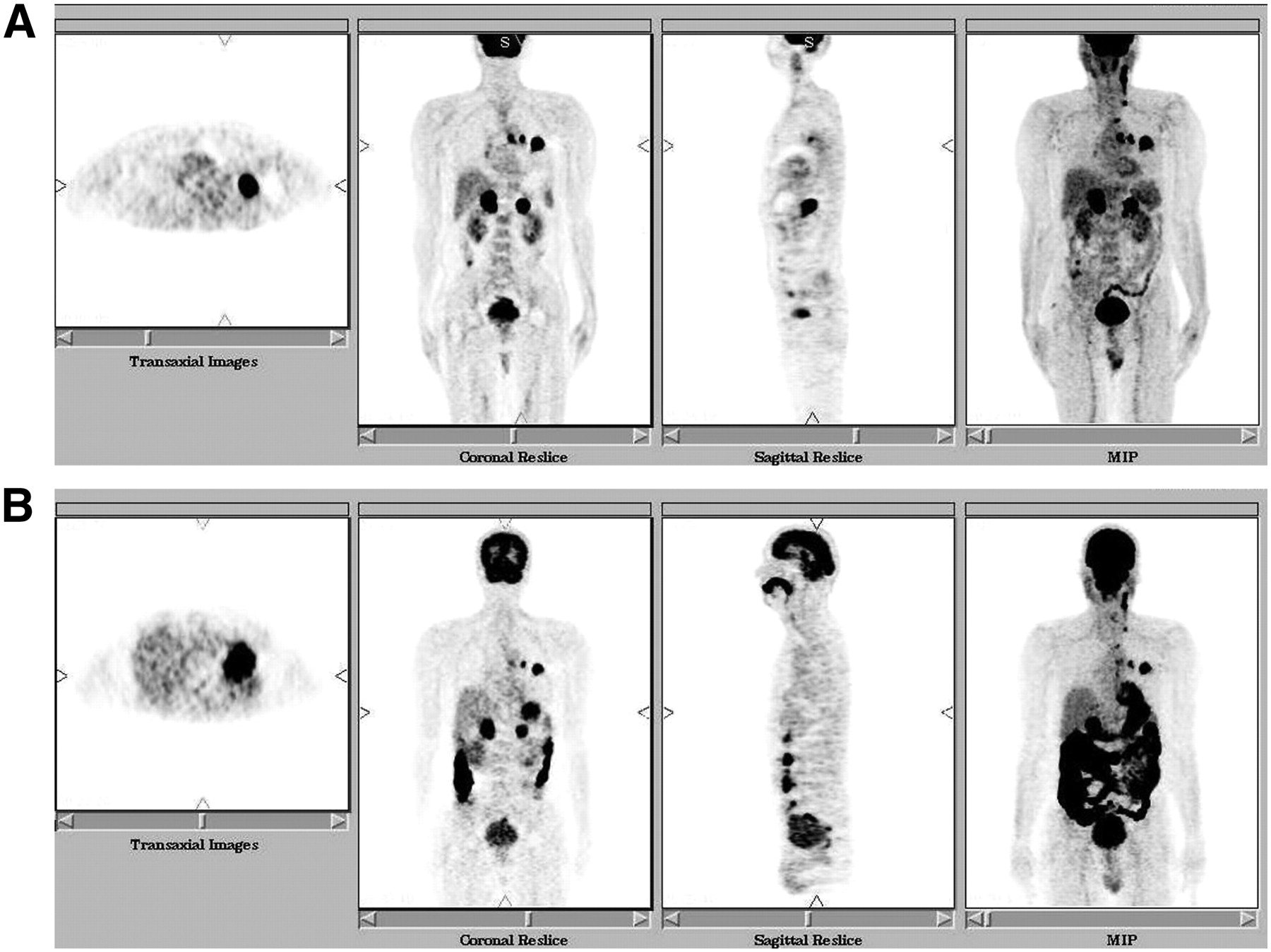
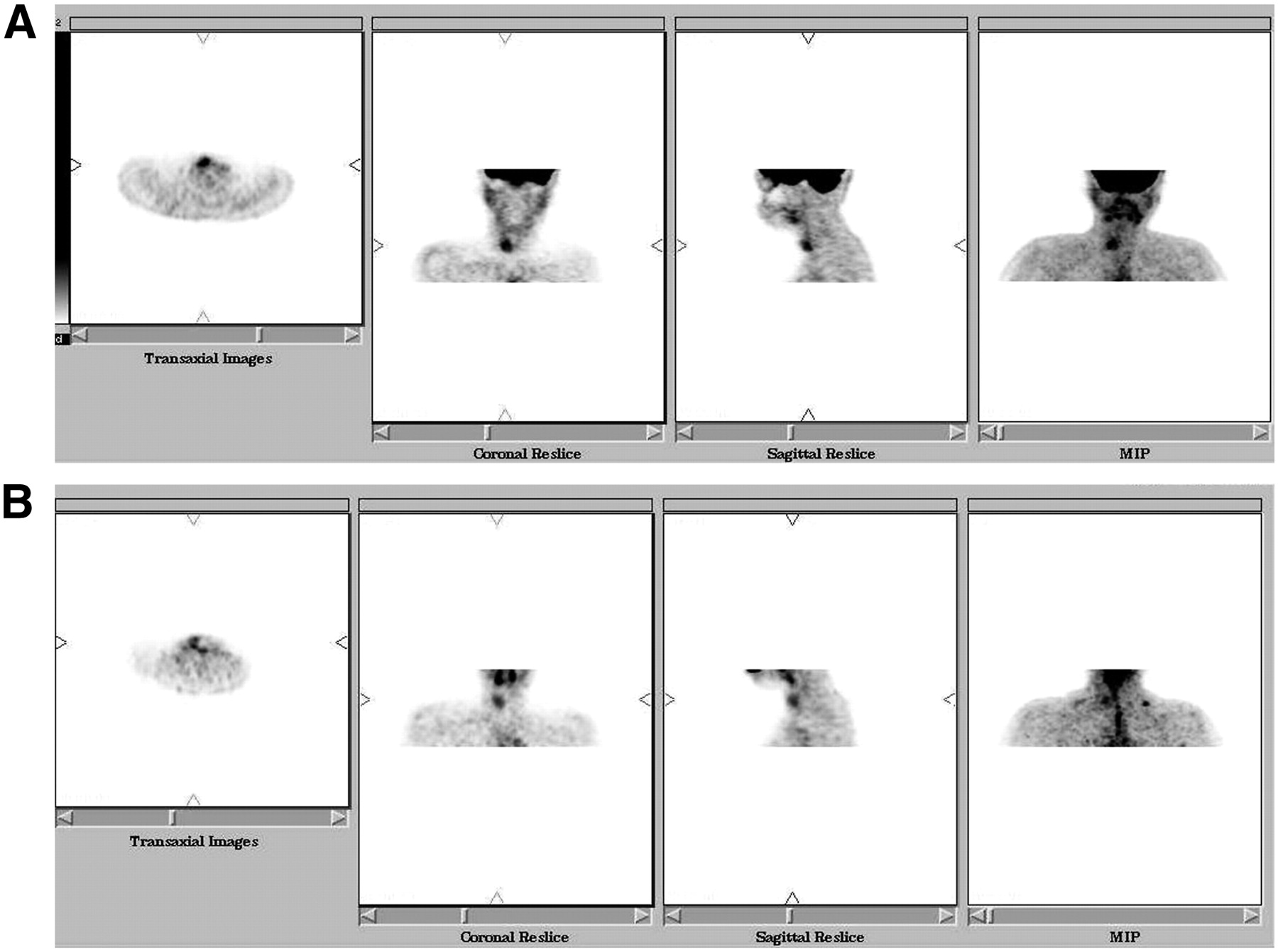
A 55-y-old woman with non-Hodgkin's lymphoma in the left axillary lymph nodes underwent PET for postchemotherapy evaluation (Fig. 4). The intravenous study showed tiny lymph nodes along the right axillary chain. All were clearly identified on the oral scan as well. The thyroid lobes were also seen on both studies. This cause of this finding was later confirmed to be thyroiditis due to raised antimicrosomal antibody titers.
Patient 5, 55-y-old woman with non-Hodgkin's lymphoma after treatment. Intravenous study (A) shows tiny right axillary lymph nodes, which are identifiable on oral study too (B). MIP = maximum intensity projection.
Patient 6
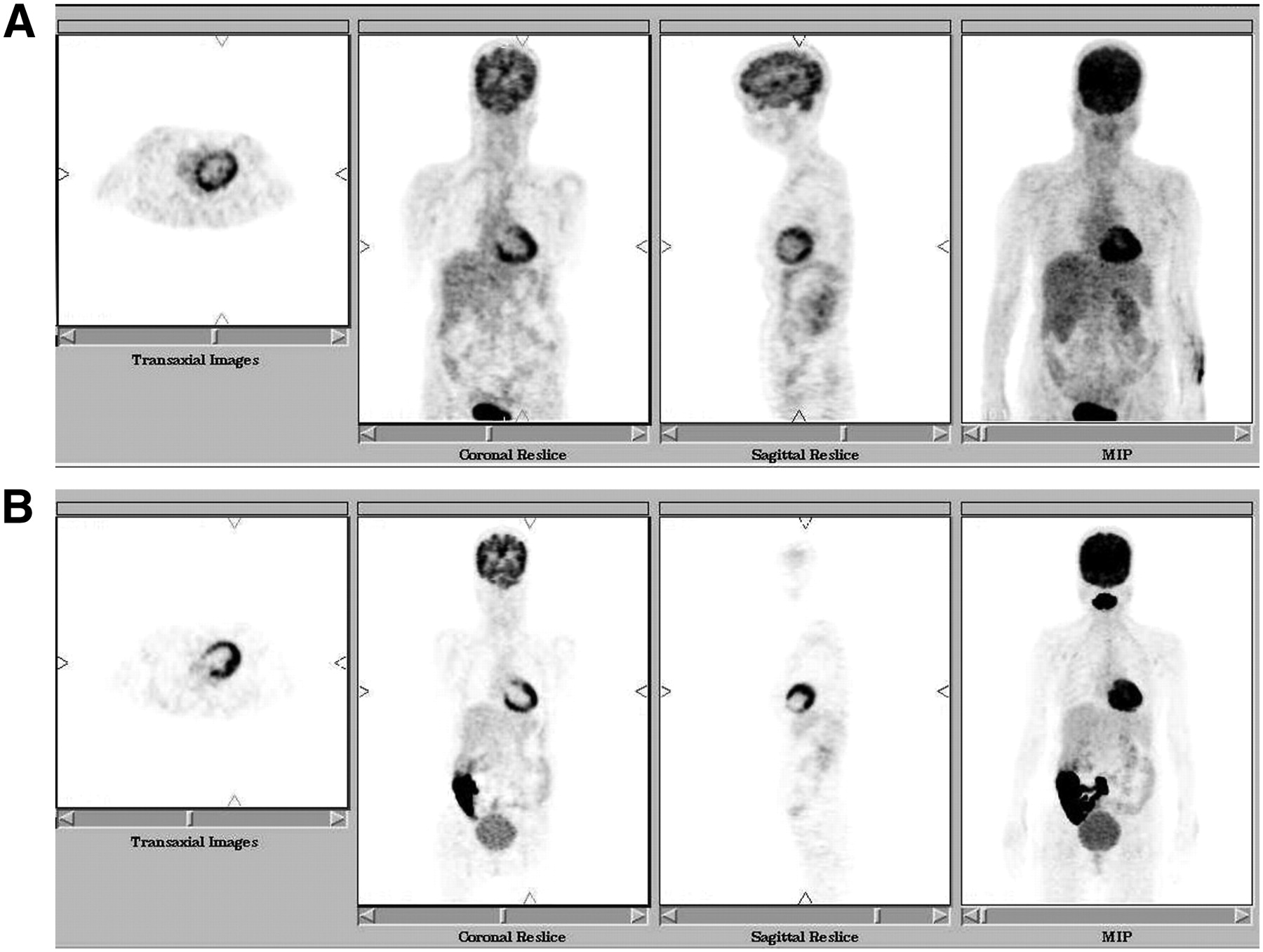
A 45-y-old woman with a fixed defect in the apical region on a 99mTc-tetrofosmin myocardial perfusion study underwent a 18F-FDG PET viability study after a glucose load (Fig. 5). The study showed absence of tracer uptake in the apex—that is, a match between the perfusion defect and the metabolic defect—indicating the defect to be a scar. Like the intravenous study, the oral study allowed good visualization of the myocardium; the apical defect persisted, leading to the conclusion that the defect indicated a scar.

Patient 6, 45-y-old woman in whom myocardial viability was being assessed. Both intravenous (A) and oral (B) studies show similar results. MIP = maximum intensity projection.
Patient 7
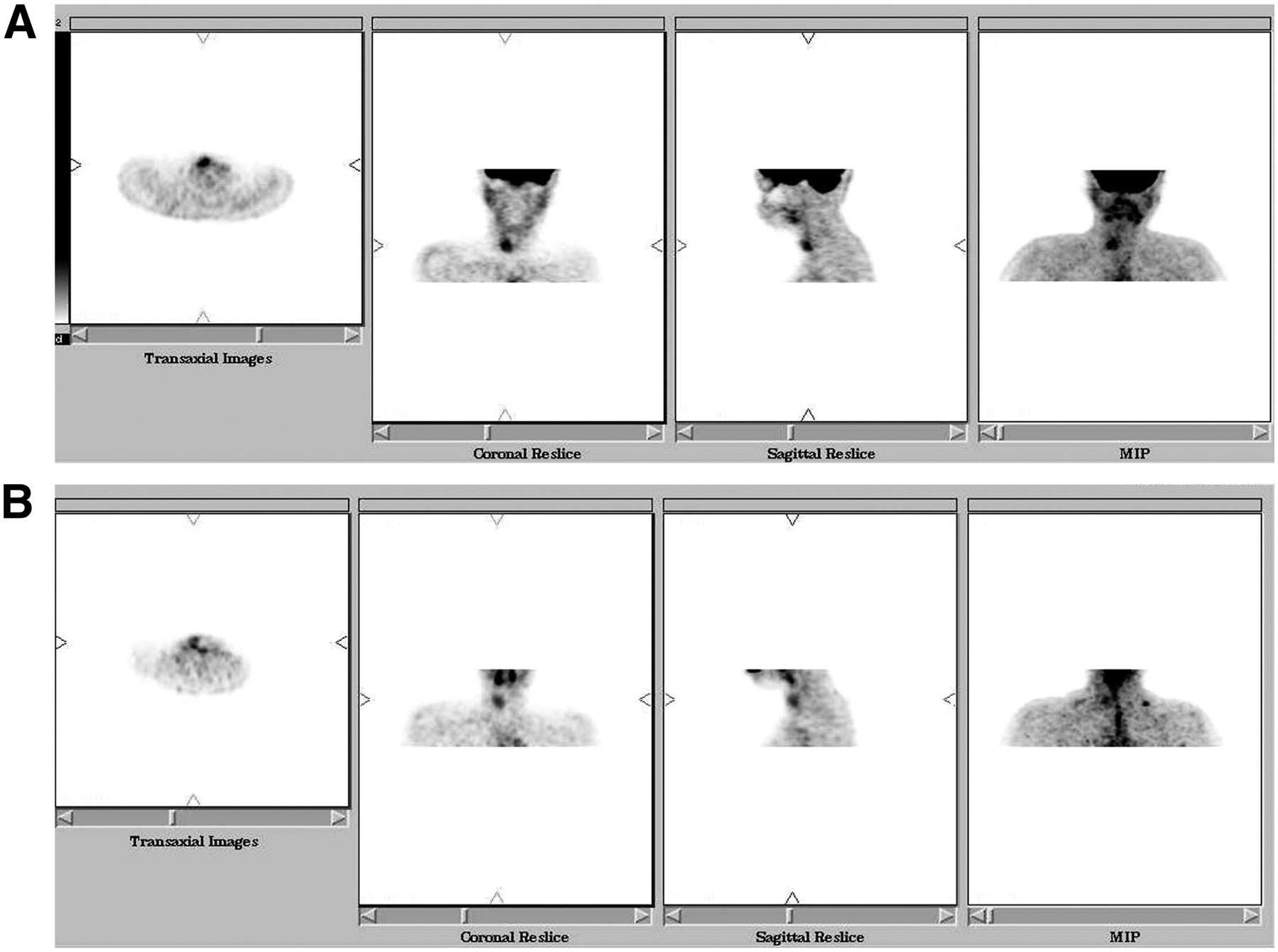
A 16-y-old girl with a nodule in the right lobe of the thyroid shown to be cold on a 99mTc-pertechnetate scan underwent subsequent 18F-FDG PET after intravenous injection of 18F-FDG (Fig. 6). Uptake within this nodule was moderate. The repeated oral study showed similar 18F-FDG uptake in the nodule. The SUV of this lesion on the oral study was about 40% of that on the intravenous study.
Patient 7, 16-y-old girl with solitary thyroid nodule in right lobe. 18F-FDG uptake is seen on both intravenous (A) and oral (B) studies. MIP = maximum intensity projection.
In the healthy volunteers, the intravenous and oral scans were compared both visually and by calculating the SUVs over the brain, liver, heart, and spleen. SUV at all sites was less on the oral study than on the intravenous study, and the upper threshold for the oral studies therefore needed to be lowered to obtain the images. Both the oral and the intravenous studies looked identical, indicating that the route of administration did not cause a problem in reading the scans.
DISCUSSION
Intravenous access may be difficult in many patients. In cancer patients after multiple cycles of chemotherapy, this problem is common because of inflammation or thrombosis, but any patient may present with difficult intravenous access. In such patients, it is important to know if oral administration of 18F-FDG can be an acceptable alternative that does not result in a loss of information. The problem of extravasated tracer leading to poor uptake of 18F-FDG in the body is well known. Multiple attempts at gaining intravenous access are no guarantee of success, and at times the patient may return to the physician without having undergone an adequate scan.
Our study showed that all lesions seen with intravenous administration were seen with oral administration as well. The SUVs of the lesions and of normal structures were, however, clearly lower on the oral studies. The SUVs of a particular individual varied by the same amount, showing that the decrease was due to a common factor—for example, the absorption of 18F-FDG from the intestines. Uptake time may be prolonged after oral administration, but we did not find the extra time inconvenient. The lower SUVs after orally administered 18F-FDG required that the upper threshold be lowered to allow visualization of tiny foci of reduced uptake, but lowering the threshold did not constitute a problem.
Glucose is absorbed by the epithelial lining of the small intestine. Enzymes in the brush border of cells lining the intestinal lumen digest the disaccharides such as lactose, sucrose, and maltose. Monosaccharides such as glucose are immediately absorbed into the portal blood. Thus, even after oral intake, 18F-FDG is absorbed in a similar manner by the small intestine and finally enters the portal blood and thus the circulation (2).
Even abnormal adrenal uptake was clearly visualized after oral administration of 18F-FDG, by scrolling through the coronal images; the gut was well to the front of the adrenals and did not hamper visualization. Lesions located amid the gut would obviously be hard to delineate on an oral study, and it remains to be seen if bowel-cleansing maneuvers might assist in this situation. But in all cases of extraabdominal disease, and in retroperitoneal cases of intraabdominal disease, oral administration of 18F-FDG can allow accurate visualization of disease.
This study did not include only cases of cancer. Although chemotherapy is a prominent reason for poor vein access in cancer patients, poor access can occur in other patients as well. The aim here was to demonstrate that in every instance, absorption through the oral route was sufficient to provide images identical to those obtained by the intravenous route. In the cardiac patient who had matching perfusion and metabolic defects in the apex of the left ventricle, after oral 18F-FDG, too, similar images of the heart were obtained. So, too, in the patient with a solitary thyroid nodule was evidence of 18F-FDG uptake into this nodule the same after both intravenous and oral administration.
Oral 18F-FDG can thus be substituted for intravenous 18F-FDG in patients who have difficult intravenous access, with the following caveat: the identification of abdominal lesions may at times be rendered difficult by an intense concentration of 18F-FDG in the intestines. This problem may partly be overcome by asking the patient to drink approximately 1–1.5 L of water after the oral dose, so as to flush out activity from the small intestine—the major hurdle in scan reading for abdominal lesions. However, by scrolling the images and by identifying the continuity of the bowel loops, one can identify even the abdominal lesions. The demonstration of adrenal metastases on oral studies despite bowel uptake is a case in point. Obviously, the viewing of predominantly abdominal disease after oral administration of 18F-FDG would be disadvantageous.
CONCLUSION
All lesions that showed uptake of 18F-FDG on the intravenous study also showed uptake on the oral study, but of lower intensity. The oral study cannot, however, be used to evaluate diseases of the gastrointestinal tract because of the large amount of 18F-FDG retained in the gut.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
- Received for publication August 29, 2006.
- Accepted for publication January 30, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}