


Abstract
In infants, brain 18F-FDG PET often requires sedation. To keep the sedation mild, the PET acquisition time should be kept short. Therefore, calculated attenuation correction is often preferred to measured attenuation correction. In addition, the infant should be positioned as comfortably as possible. Here, we report a case in which the infant's fist was near her head, resulting in severe artifacts when calculated attenuation correction was applied. Brain 18F-FDG PET was performed for localization of a focus in an 11-mo-old girl with West's syndrome. After injection of 120 MBq of 18F-FDG, a 20-min emission scan was obtained. Then, a 7-min hot transmission scan was acquired with 3 rotating 68Ge/68Ga rod sources. Attenuation was corrected both by calculated attenuation correction and by measured attenuation correction using the transmission scan. Images reconstructed with calculated attenuation correction showed apparently increased 18F-FDG uptake in the skin of the neck. The fist was not visible on the images because it was outside the reconstructed field of view. The lesion of increased 18F-FDG uptake was not immediately recognizable as an artifact. It might have been misinterpreted as an active process, such as inflammation, in the skin. However, the lesion showed up neither on images reconstructed with measured attenuation correction nor on images without attenuation correction. Detailed analysis of each step in the calculated attenuation correction revealed that the fist caused the boundary detection algorithm to detect not the boundary of the head but a strongly extended boundary enclosing the fist and large “air areas” between the fist and the head. The result was a significant overestimation and overcorrection of attenuation, particularly in the region of skin near the fist.
Because infants are unable to cooperate, they often require sedation during brain 18F-FDG PET to reduce movement artifacts. However, because the sedation needs to be kept short and mild, the total time of the PET study needs to be kept short. Therefore, calculated attenuation correction is often preferred to measured attenuation correction, which is based on a separate transmission scan with positron-emitting sources and adds up to 10 min to the total acquisition time. A further advantage of calculated attenuation correction over measured attenuation correction is that it avoids artifacts that might occur because of movements between the emission and the transmission scans (1).
In addition to keeping the acquisition time short, one should position infants as comfortably as possible on the bed of the PET system in order not to awaken them during the procedure. However, overly considerate positioning might result in the presence of other parts of the body besides the head (e.g., a fist) in the field of view of the PET acquisition.
This case report demonstrates that the use of calculated attenuation correction might result in severe and hard-to-recognize artifacts when other parts of the body, such as a fist, are positioned within the field of view of the brain PET acquisition.
CASE REPORT
Subject
Brain 18F-FDG PET was performed to localize a putative focus in an 11-mo-old girl (height, 73 cm; weight, 12 kg) who had been experiencing 1–2 epileptic seizures per day (West's syndrome (2)).
PET
PET was performed on a full-ring system (ECAT EXACT 921/47; Siemens/CTI) in 2-dimensional mode (3). This system covers an axial field of view of 16.2 cm by collecting 47 transverse slices 3.4 mm thick. After having been kept fasting for 4 h, the infant received 120 MBq of 18F-FDG intravenously, followed by a 48-min resting period with intravenous infusion of NaCl. A seizure occurred during the rest period, 38 min after the 18F-FDG injection. Therefore, sedation with prothipendyl hydrochloride was required to ensure optimal imaging conditions. After the resting period, a 20-min emission scan of the head was obtained, followed by a 7-min hot transmission scan acquired with 3 rotating 68Ge/68Ga rod sources (4–6). The sinograms were corrected for random coincidences, radioactive decay, dead time, varying detector efficiency, attenuation, and nonuniform sampling (geometric arc correction). No scatter correction was applied. Forty-seven transaxial slices of 128 × 128 voxels were reconstructed by filtered backprojection using a Hanning window with a cutoff at the Nyquist frequency. Thereafter, the images were 3-dimensionally smoothed by application of a 5 × 5 × 3 binomial kernel. The voxel size was 1.7 × 1.7 × 3.4 mm, and spatial resolution was about 9 mm in full width at half maximum.
Attenuation Correction
Calculated attenuation correction was applied using the algorithm implemented in the scanner software (ECAT version 6.5B) (7,8). Because this method is expected to be reliable, it is routinely used in our department. The method is based on a simplified model consisting of a uniform brain surrounded by a uniform skull.
Visual inspection of the images reconstructed with calculated attenuation correction revealed an apparent increase in 18F-FDG uptake in the skin on the left side of the neck (Fig. 1A). The lesion was not immediately recognizable as an artifact. However, because this finding was unexpected, reconstruction was repeated with measured attenuation correction based on the transmission scan (4,5). Reconstruction without attenuation correction was also performed.
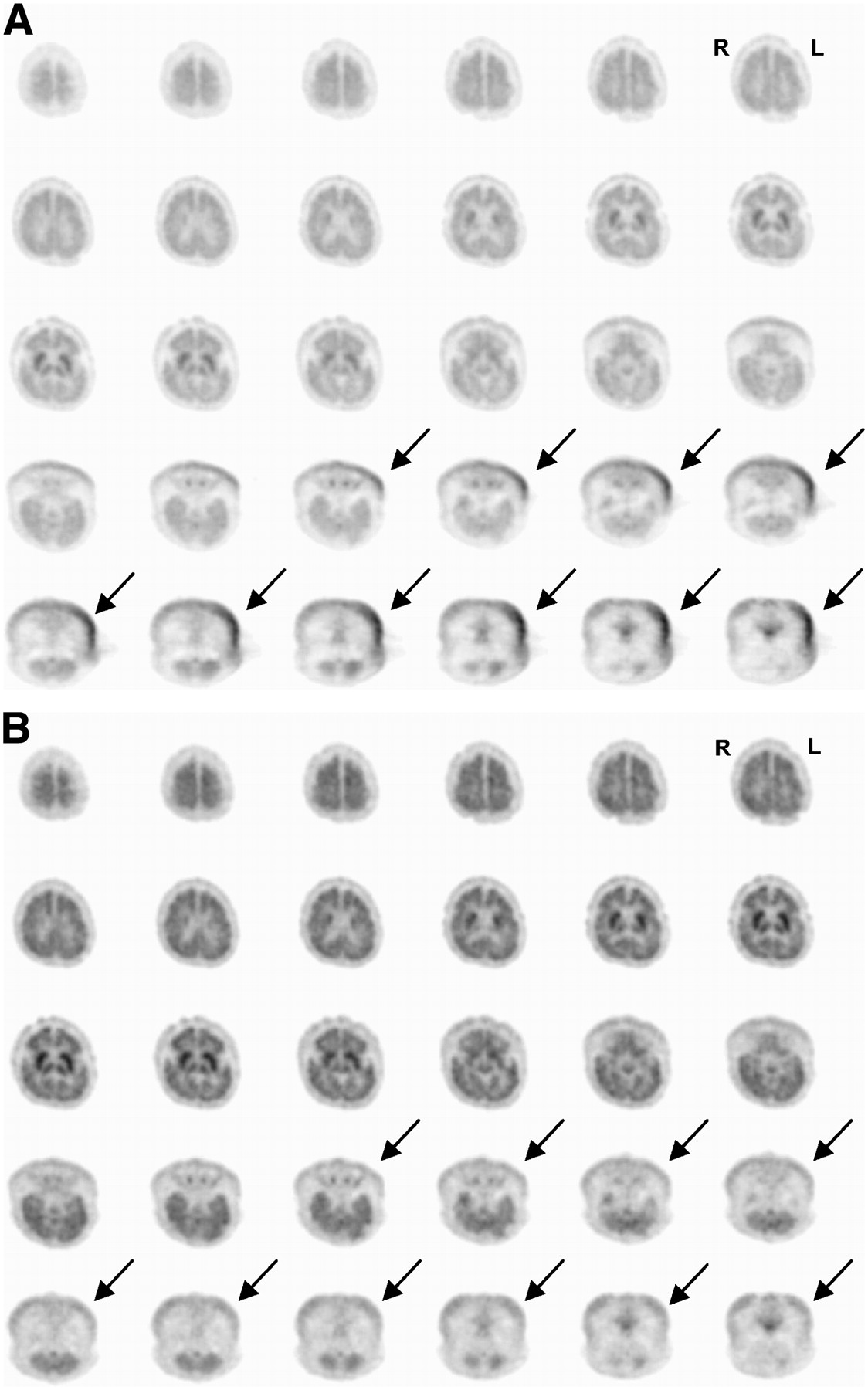
Transverse slices of brain 18F-FDG PET study of 11-mo-old girl with epileptic seizures. Attenuation correction was performed using method for calculated attenuation correction provided by scanner software (A) and using postinjection transmission scan (measured attenuation correction) (B). Calculated attenuation correction showed lesion of apparent hypermetabolism at level of skin on left side of neck (arrows). Comparison with measured attenuation correction, which did not show hypermetabolism at neck, suggested that this finding was artifact related to calculated attenuation correction.
The skin lesion seen with calculated attenuation correction showed up neither with measured attenuation correction (Fig. 1B) nor without attenuation correction. Therefore, the lesion was suspected to be an artifact of calculated attenuation correction, and the process for that correction in the current subject was analyzed in detail.
The sinograms corresponding to the transverse slices containing the skin lesion on calculated attenuation correction images showed an extracranial hot object within the field of view (Fig. 2). The object had not been visible on the reconstructed images because of the reconstruction zoom.
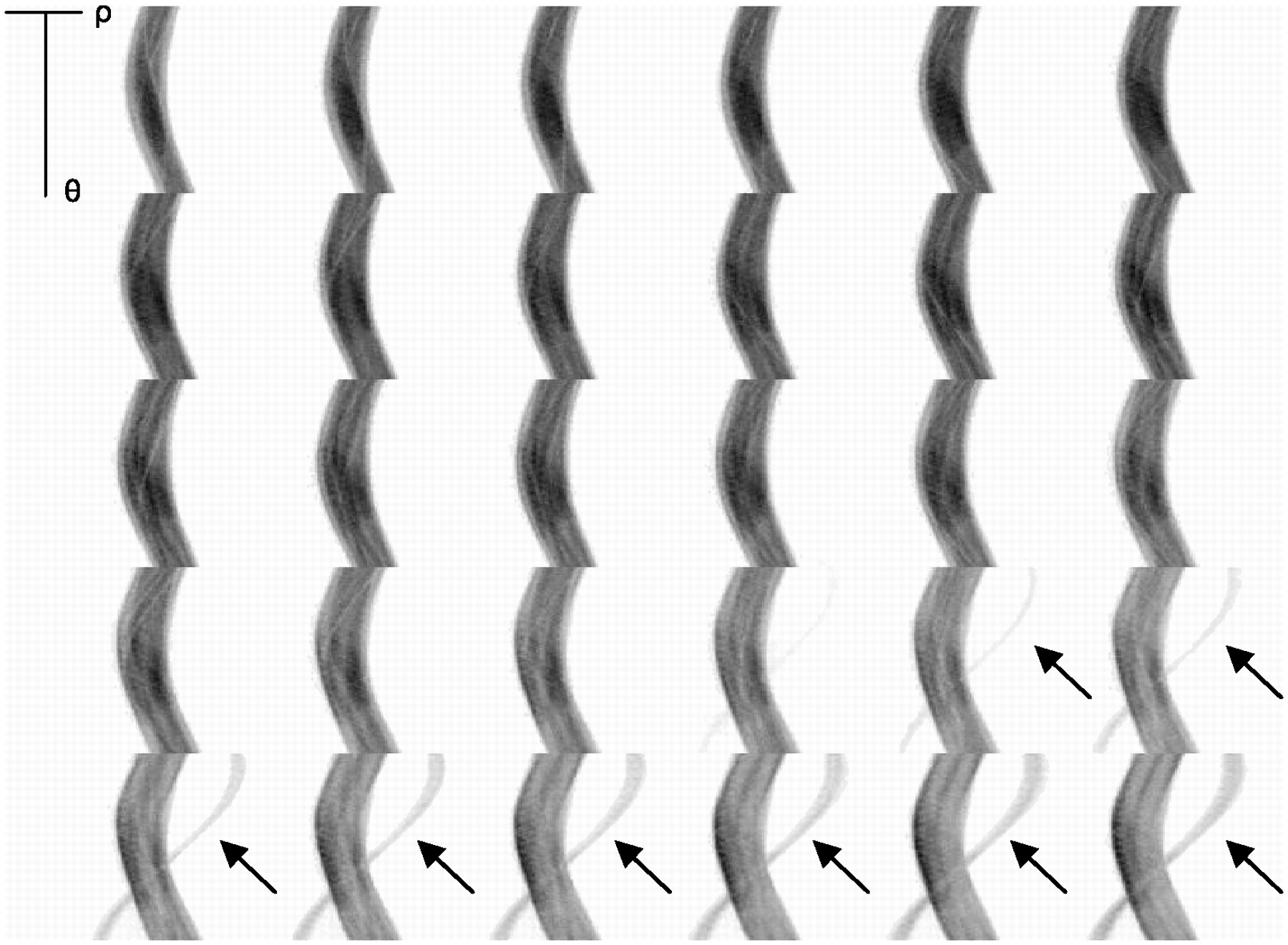
Sinograms corresponding to transverse slices in Figure 1. Sinograms are corrected for varying detector efficiency (normalized) but not for attenuation. Obvious extracranial hot object is seen within field of view at level of calculated attenuation correction lesion in neck (arrows). Object is assessed more easily on projection images (Fig. 3).
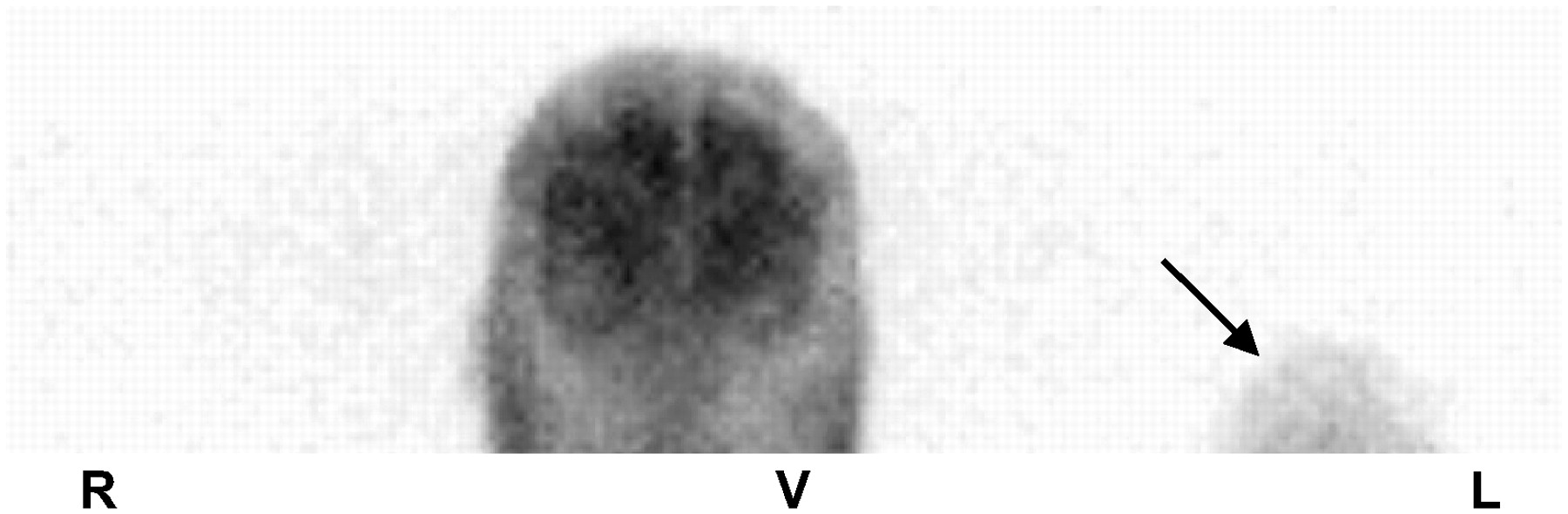
Using the ventral projection image, obtained by reordering the sinograms, we identified the hot object to be the infant's left fist (Fig. 3). Positioning the infant as comfortably as possible had resulted in the fist ending up close to the head, within the field of view of the PET acquisition.
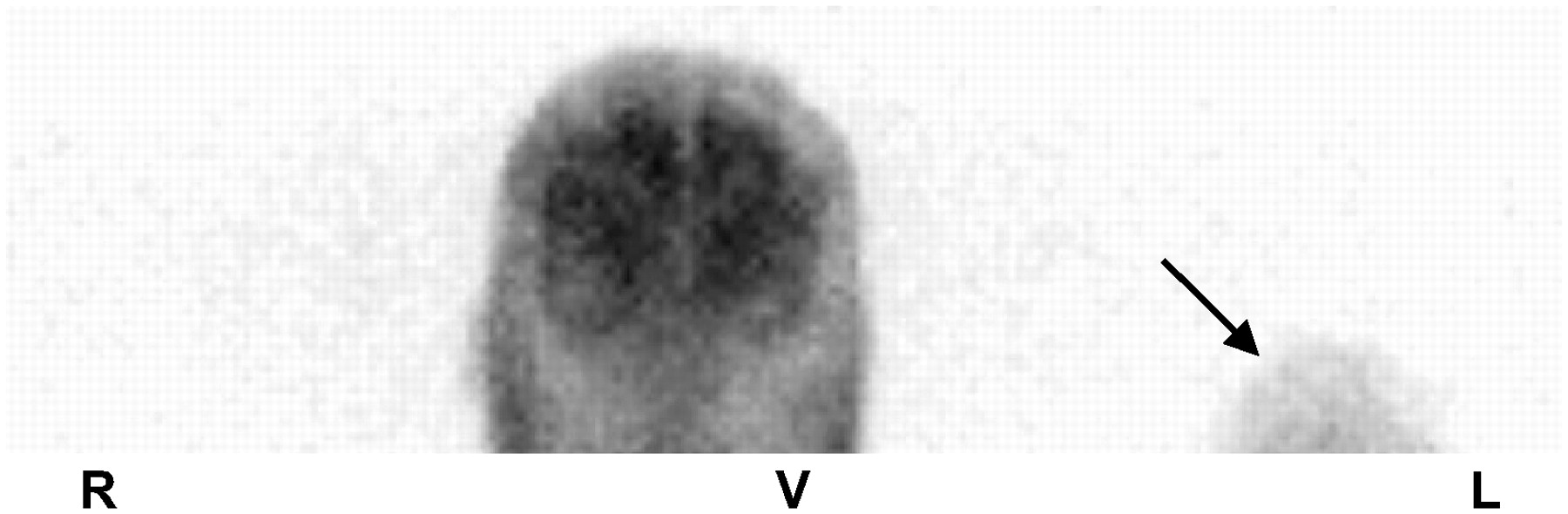
Ventral (V) projection of brain 18F-FDG PET shown in Figure 1. Hot object to left of head most likely is infant's left fist.
The fist had caused the boundary-detection algorithm of calculated attenuation correction to detect not the boundary of the head but a strongly extended boundary enclosing the fist and large “air areas” between the fist and the head (Fig. 4). The result was a significant overestimation of the attenuation, because the attenuation correction was calculated with the assumption that the included air areas were actually tissue. In turn, a significant overestimation of 18F-FDG uptake resulted, particularly in the region of skin near the fist.
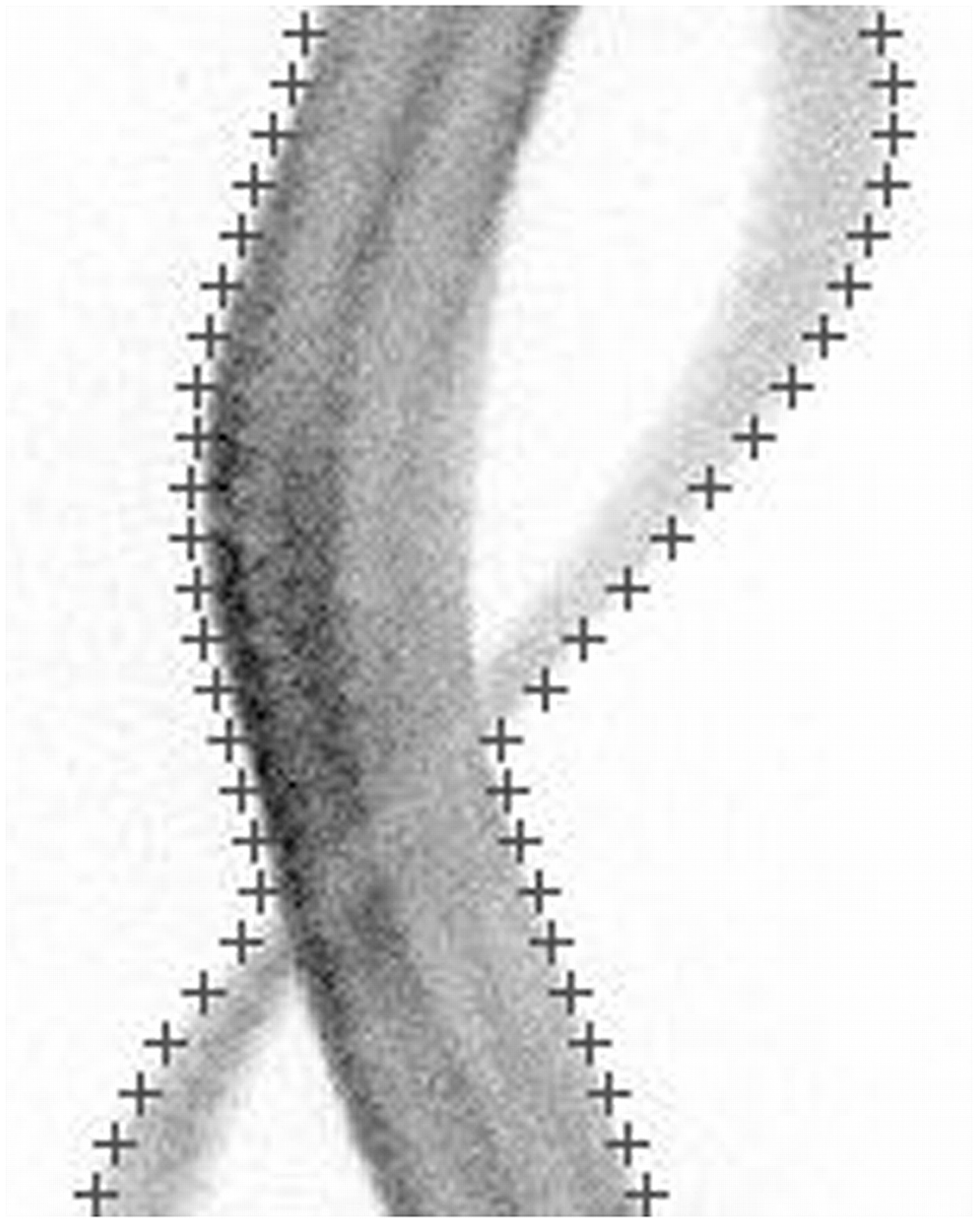
Sinogram corresponding to fourth slice from the end in Figure 1. Crosses indicate boundary detected by calculated attenuation correction method. Method assumes that detected boundary defines surface of skull, skull has constant thickness and homogeneous attenuation coefficient, and medium under skull has homogeneous attenuation coefficient characteristic of brain tissue. Hot object to left of head caused calculated attenuation correction to significantly overestimate size of head and, thus, to overestimate attenuation factors. This overestimation resulted in overcorrection of 18F-FDG uptake, predominantly in areas close to hot extracranial object.
DISCUSSION
The present case report demonstrates that hot objects in the field of view, such as a patient's fist or arm, might cause severe artifacts that might not be immediately recognizable as such on brain 18F-FDG PET images reconstructed with calculated attenuation correction.
Aspects of image processing that do not directly interfere with attenuation correction, such as scatter correction or reconstruction algorithms (spatial resolution), are not expected to significantly affect the degree to which the artifacts are perceived.
Reconstruction without attenuation correction might be useful for clarifying unexpected findings. Unexpected findings that are present on attenuation-corrected images but not on non–attenuation-corrected images most likely are artifacts. In fact, one might recommend that non–attenuation-corrected images always be inspected in addition to attenuation-corrected images, not only in whole-body PET but also in brain PET.
The artifact described here is related to the use of calculated attenuation correction. Therefore, the artifact is independent of whether a stand-alone PET system or a PET/CT system is used for the emission scan. However, measured attenuation correction based on a low-dose CT scan of the head might be preferred over calculated attenuation correction in PET/CT. In contrast to a transmission scan obtained with external positron emitters, a CT scan takes only a few seconds. In addition, because the radiation exposure from low-dose CT of the head is rather small, measured attenuation correction with low-dose CT might be recommended also for children.
CONCLUSION
Placement of hot objects, such as the patient's fist or arm, in the field of view should be avoided when calculated attenuation correction is used in brain 18F-FDG PET. Artifacts due to calculated attenuation correction might be detected by inspection of non–attenuation-corrected images.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 16, 2006.
- Accepted for publication September 5, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.