


Abstract
When body position changes from erect to supine, the effect of gravity on the organs also changes and is a possible underlying mechanism for upward creep of the heart during SPECT acquisitions. We hypothesized that if we provide enough time for the organs to settle after a positional change, the range of this vertical motion causing reconstruction artifacts can be decreased. Our aim was to evaluate the effect that a 5-min bed rest on the imaging table before both rest and stress SPECT acquisitions would have on upward creep of the heart. Methods: Before both stress and rest SPECT acquisitions, the first 101 consecutive patients (group A) had a 5-min bed rest and the remaining 99 patients (group B) did not have any bed rest after they were positioned on the imaging table. Upward creep was detected by comparing the distance between the lower edge of the image and the lowest part of the heart silhouette on the last projection image of detector 2 and the first projection image of detector 1. Results: Upward creep was found in 53% (54/101) and 55% (56/101) of patients in group A and in 89% (88/99) and 86% (85/99) of patients in group B in stress and rest SPECT studies, respectively. Upward creep of the heart was decreased prominently in group A, and this decrease was statistically significant (p < 0.001). Conclusion: We conclude that before SPECT acquisition, at least a 5-min bed rest on the imaging table significantly decreases vertical motion of the heart.
When the projection images of a myocardial perfusion SPECT study recorded by a dual-head γ-camera in cine mode are reviewed, a vertical change in position of the heart is usually noticed between the last frame of detector 2 and the first frame of detector 1. Although these 2 datasets recorded by 2 different detectors are theoretically accepted as consecutive images, there is actually an interval between them during which repositioning of the heart occurs. This phenomenon, the so-called upward creep of the heart, was first described by Friedman at al (1). It characterizes a gradual upward shift of the heart.
Artificial perfusion defects can be triggered by patient motion on myocardial SPECT scans (2–4). Upward creep of the heart during SPECT acquisitions may also cause reconstruction artifacts and, therefore, false-positive reversible defects (1,5–7). It has been reported that movement by even 1 pixel can provoke reconstruction errors and create artifacts that resemble anterior and posterior perfusion defects (8–10). It has also been reported that visual artifacts were more detectable and quantitative abnormalities more frequent as the distance of movement increased (11).
Diaphragmatic movement in the supine position is greater than that in the sitting position, especially in the posterior part of the diaphragm (12). When body position changes from erect to supine, the effect of gravity on the organs also changes. Intraabdominal organs move upward, the heart comes into close physical contact with the diaphragm, the weight of the heart on the diaphragm decreases, the muscles of the abdominal wall get involved in the respiration process, the diaphragm relaxes, and the lung volume decreases (13–16). These adaptive changes require a certain time frame. We hypothesized that if we provide enough time for the heart to adapt to the change in gravitational direction, the range of vertical motion of the heart during SPECT acquisitions could be decreased. The aim of this prospective study was to evaluate the effect that a 5-min bed rest on the imaging table before both rest and stress SPECT acquisitions would have on upward creep of the heart.
MATERIALS AND METHODS
Study Population
Two hundred consecutive patients referred for myocardial perfusion imaging to evaluate known or suspected coronary artery disease were included in this prospective study. The patients were divided into a study group and a control group. The study group (group A), consisting of the first 101 consecutive patients (65 men and 36 women; age range, 12–80 y), had a 5-min bed rest after they were positioned on the imaging table before both stress and rest SPECT acquisitions. In the control group (group B), consisting of the next 99 patients (57 men and 42 women; age range, 21–78 y), both stress and rest SPECT acquisitions were initiated immediately after the patient had been positioned on the imaging table, without any prior bed rest.
A structured interview was performed, the clinical history was taken, and cardiac risk factors were assessed before nuclear testing. Exclusion criteria were any surgery involving the heart, lungs, or great vessels; known obstructive airway disease; and diseases involving the diaphragm and phrenic nerves (6,17–19). Patients who moved for any reason during the SPECT acquisition were also excluded from the study. All vasoactive medications were withheld for at least 24 h before the patients underwent SPECT. All patients were informed about the procedure and consented to it orally beforehand. The hospital ethics committee approved the study protocol.
Technique, Acquisition Protocol, and Instrumentation
All patients underwent a 2-d (stress–rest 99mTc-methoxyisobutylisonitrile [MIBI]) protocol of stress myocardial perfusion imaging. After symptom-limited treadmill exercise using the standard Bruce protocol, 740–925 MBq (20–25 mCi) of 99mTc-MIBI (Cardio-SPECT; Medi-Radiopharma) were injected intravenously at peak stress and on the following day for rest SPECT. Acquisitions were initiated 30 ± 15 min (mean ± SD) after the injection of 99mTc-MIBI while the patients were supine. For the second phase of the investigation, a dynamic sequence (1 min/frame for 5 min) was acquired for group A to evaluate upward creep of the liver during bed rest before both stress and rest SPECT.
Quality control of the γ-camera was performed routinely before the first study of each day. SPECT images were acquired with a dual-head dedicated cardiac γ-camera (Optima; GE Healthcare) fitted with low-energy high-resolution collimators. Sixty-four projections were acquired at 28 s per projection over 180° (from 45° right anterior oblique to 45° left posterior oblique). A 15% window was centered over the 140-keV photopeak. Data were stored in a 64 × 64 matrix, and a 1.33 zoom was applied. No attenuation or scatter correction was used. Filtered backprojection reconstruction used a ramp filter followed by 2-dimensional Butterworth filtering (order, 5; cutoff frequency, 0.52 cycle per pixel). Any motion was documented visually using cinematic display of the projection datasets.
Image Evaluation
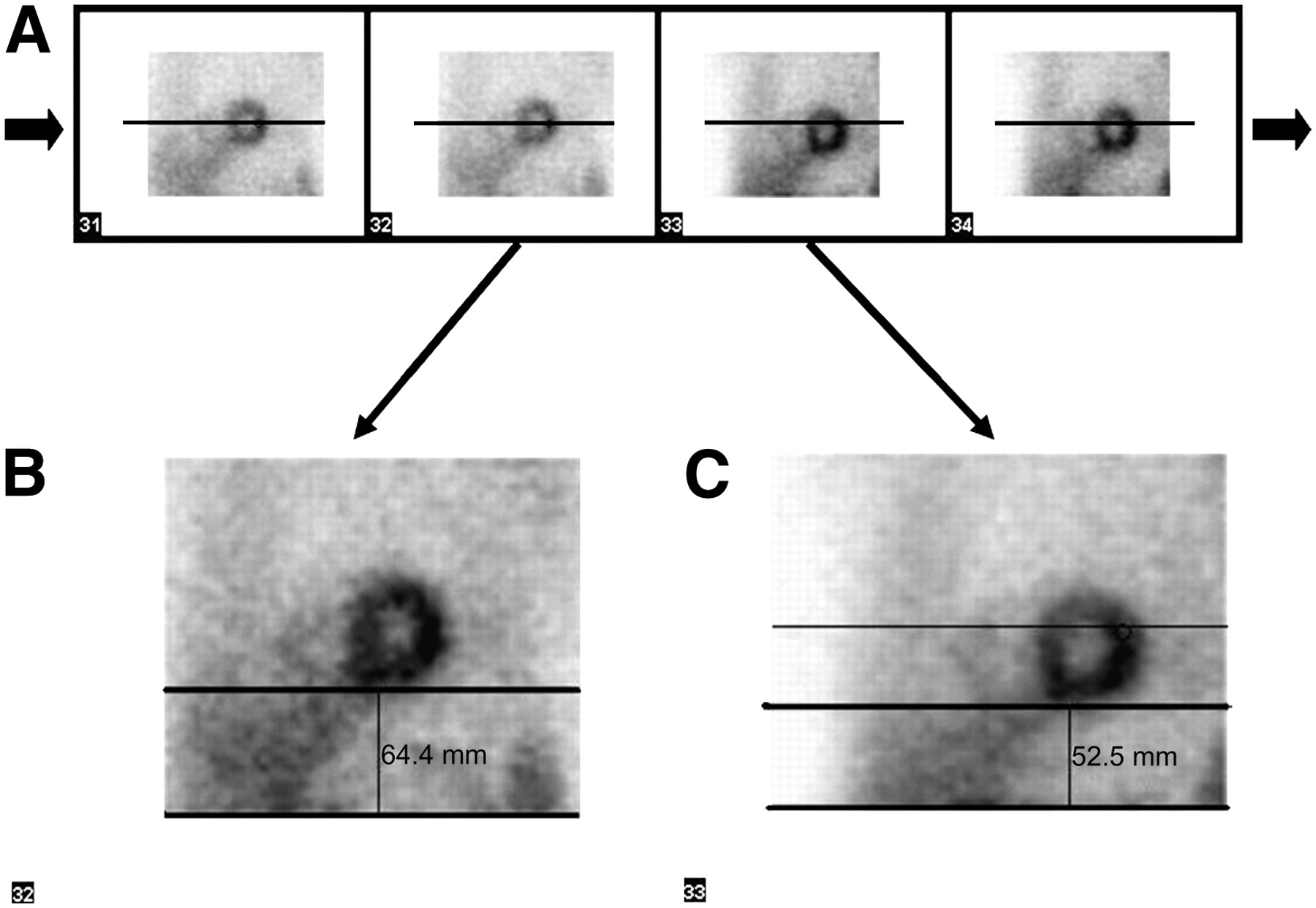
Upward creep can easily be detected by comparing the levels of the lower border of the heart silhouette on consecutive projection images. The distance between a straight line fitted to the lower border of the heart and the lower edge of the image on both the 32nd and the 33rd projections was measured in both stress and rest studies (Figs. 1 and 2). Using this technique, a vertical translation as small as 1 mm could be detected easily.
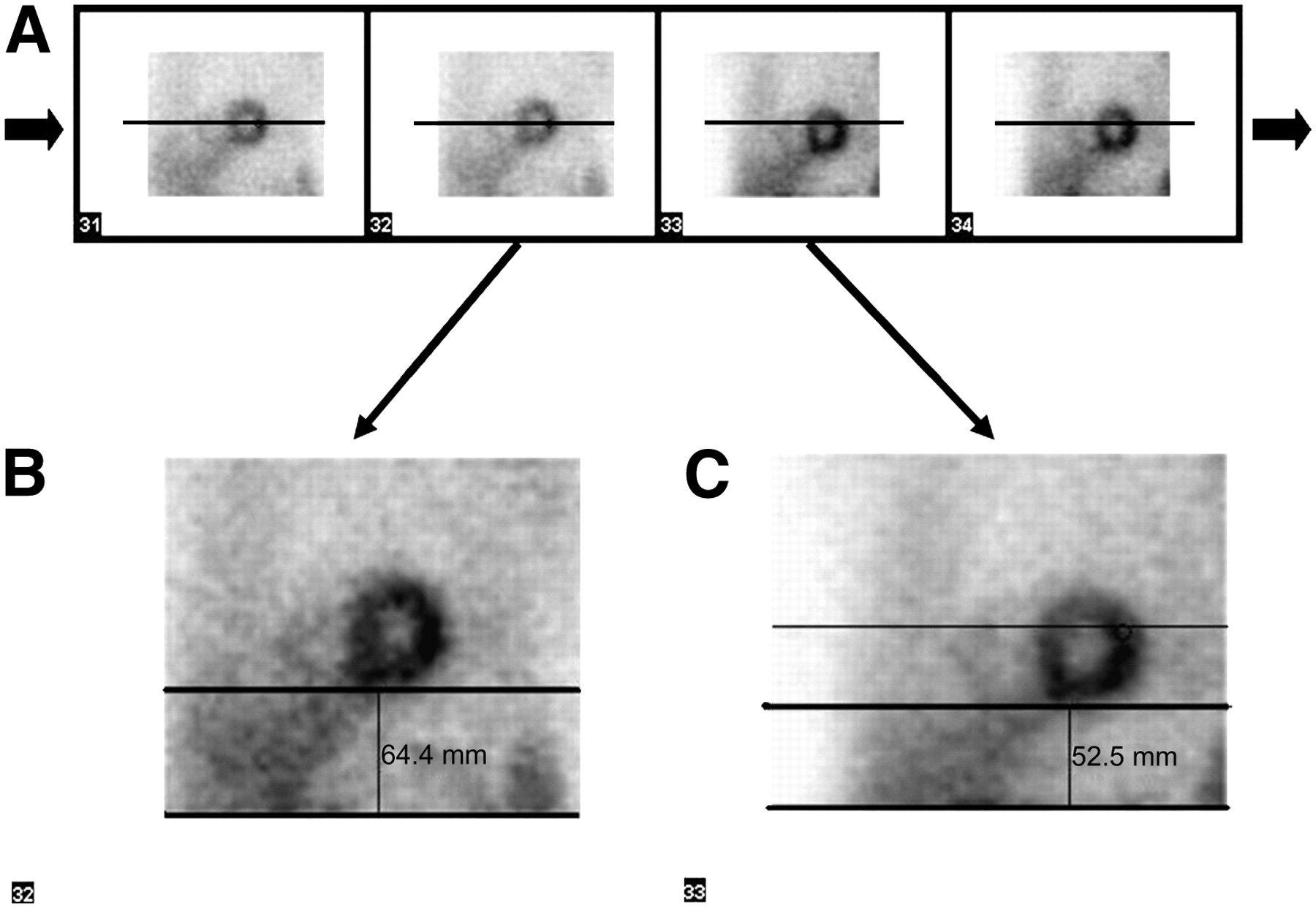
(A) Projection images derived from stress SPECT. (B and C) Thirty-second frame is last projection image of detector 2 (B), and 33rd frame is first projection image of detector 1 (C). Upward creep of heart can easily be detected by comparing distance between lower edge of image and lowest part of heart silhouette on these consecutive images.

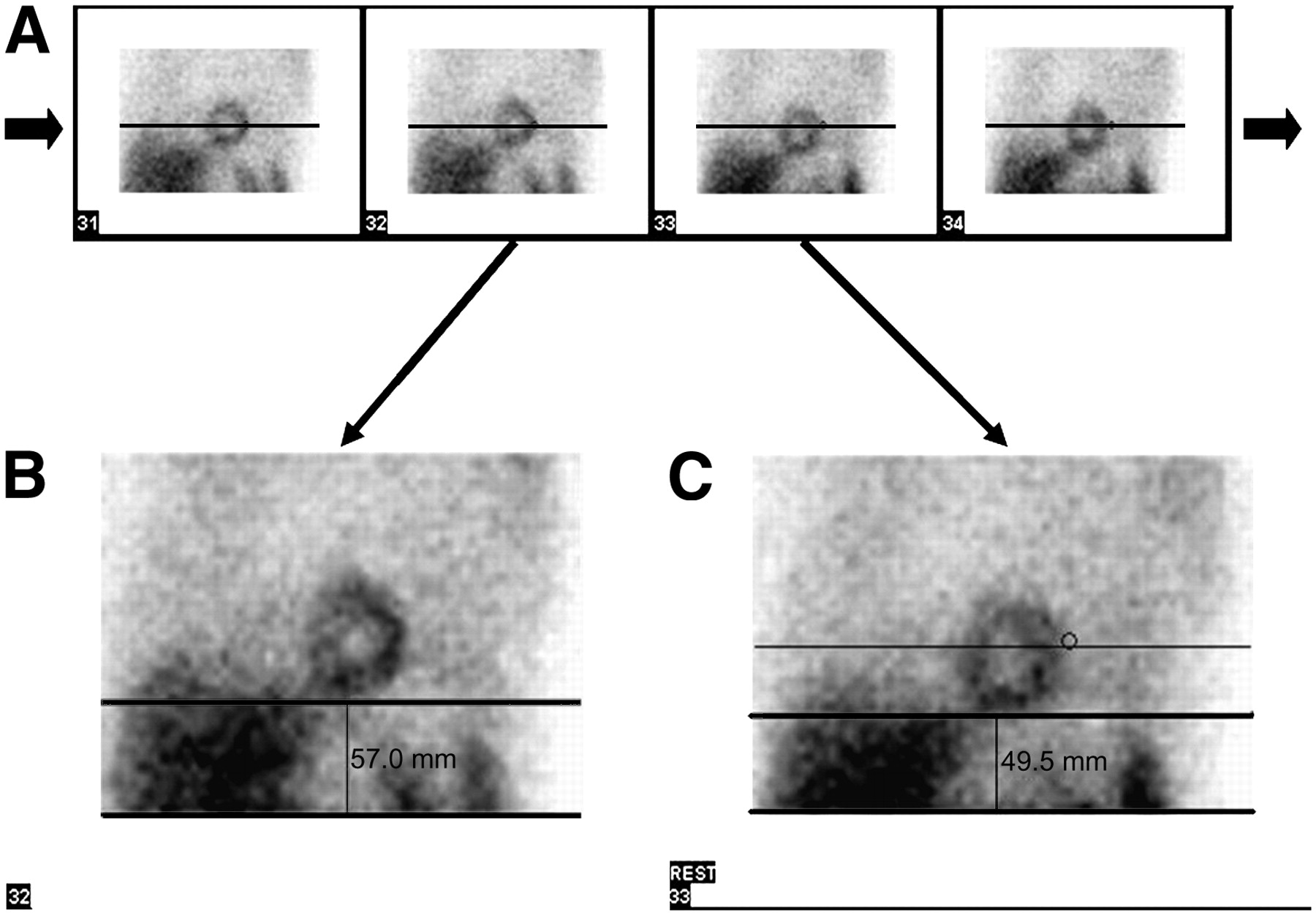
(A) Projection images derived from rest SPECT. (B and C) Thirty-second frame is last projection image of detector 2 (B), and 33rd frame is first projection image of detector 1 (C). Upward creep of heart can also be detected after rest SPECT because the phenomenon is physiologic and happens in varying degrees at every change in body position from erect to supine.
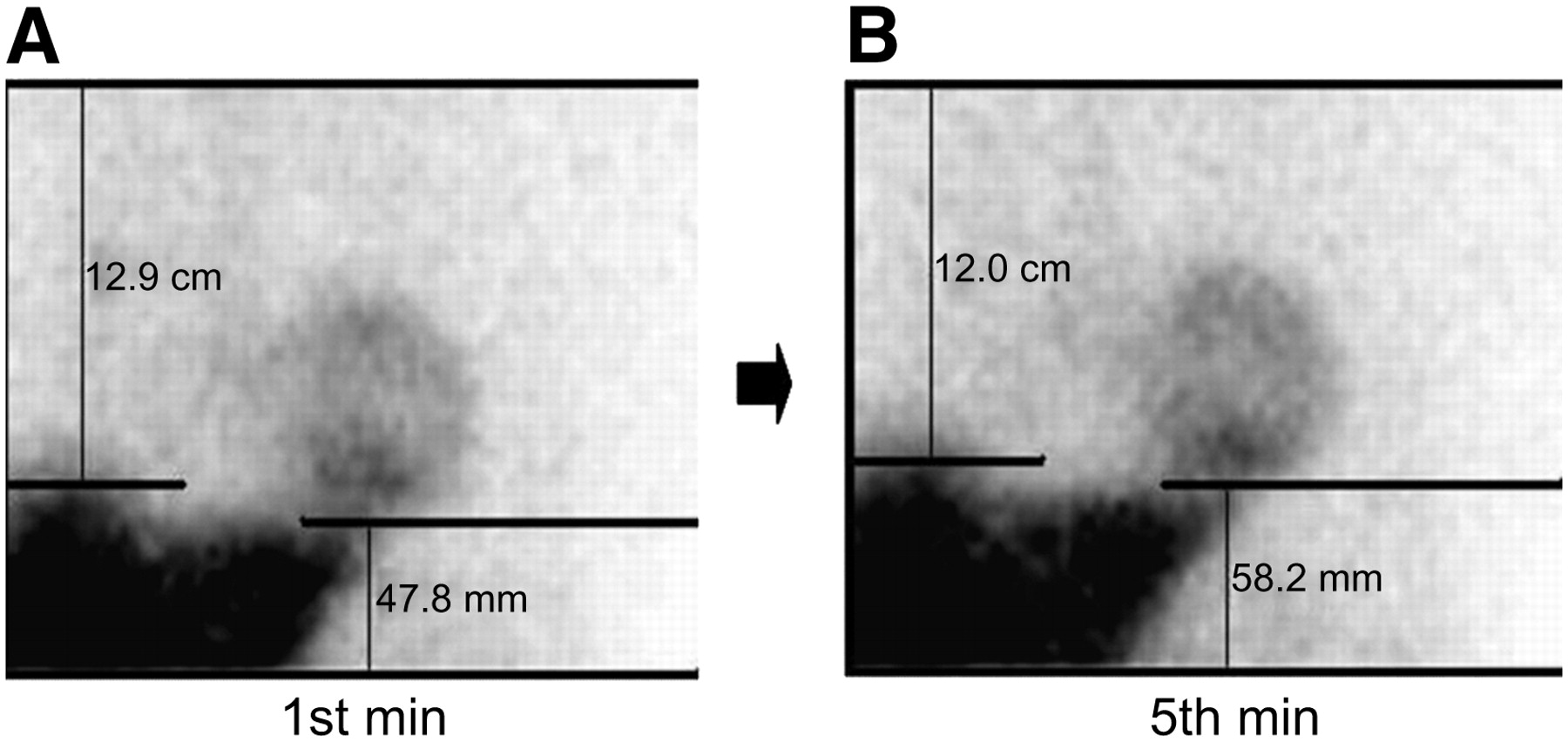
We also measured the distance between the upper edge of the liver and the upper edge of the image to detect upward creep of the liver on the first- and fifth-minute dynamic images in group A (Fig. 3).
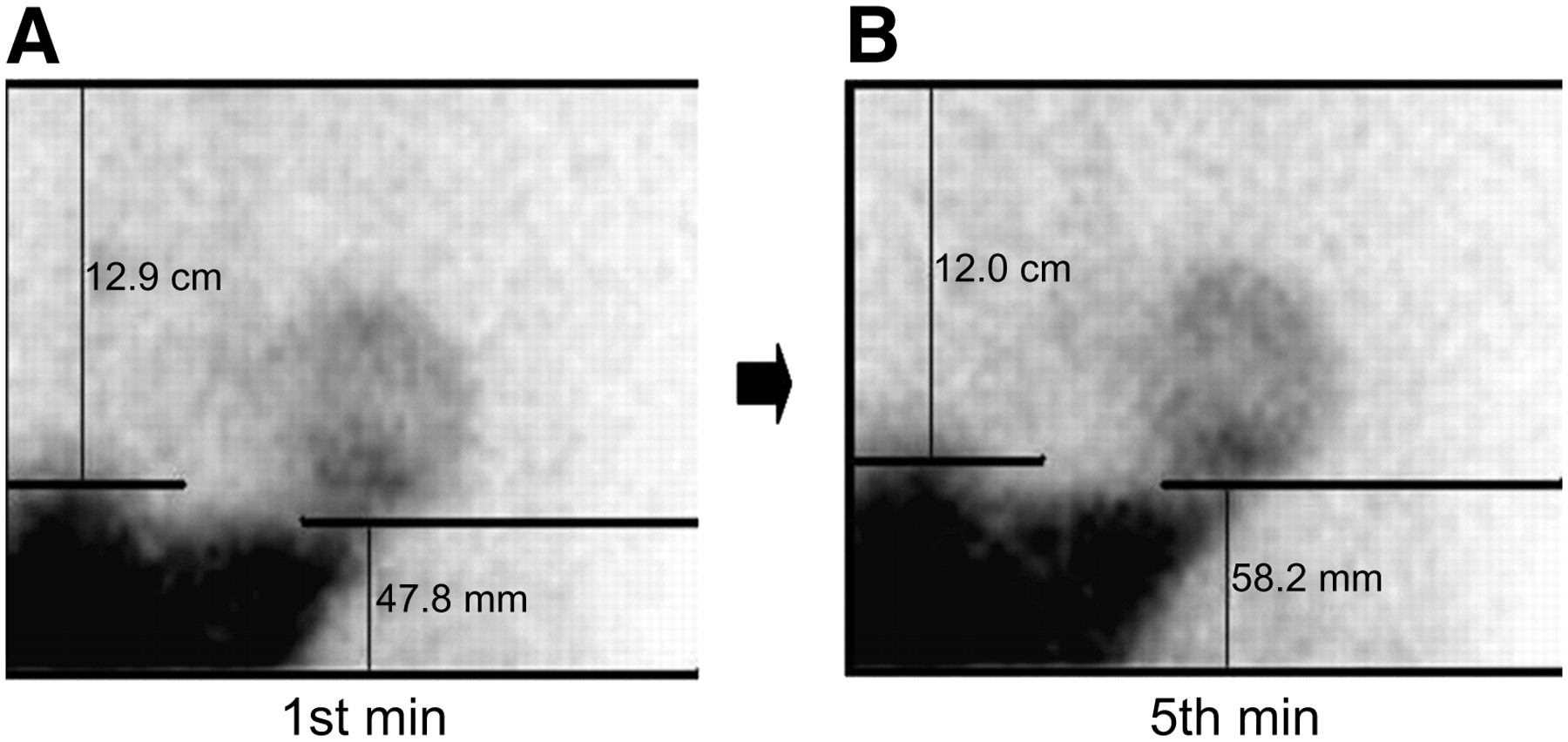
Images derived at first min (A) and at fifth min (B) of dynamic study of patient in group A demonstrate vertical motion of liver and heart. Considering positions of both organs according to diaphragm, detection of vertical motion of both organs at same time signifies diaphragmatic relaxation.
Scintigraphic images were analyzed by 2 experienced observers in a masked manner, and the results were reported as normal, ischemia, or infarct.
Statistical Analysis
Descriptive statistics were expressed as mean ± SD, median, and proportions. Distributions of continuous variables were evaluated by the Kolmogorov–Smirnov test, and Levene's test was used to determine the equality of variances. Differences between the measurements derived from consecutive cine images (the 32nd and 33rd frames) were tested for significance using the Wilcoxon signed rank test.
The significance of difference between measurements derived from the cine images of groups A and B was tested using the Mann–Whitney U test. The difference between measurements derived from the dynamic images was tested for significance using the Wilcoxon signed rank test, and the χ2 test was used to compare nominal variables. Statistical analysis was performed using the SPSS 10.0 Statistical Package (SPSS Inc.) for Windows (Microsoft). Values of p less than 0.05 were considered statistically significant.
RESULTS
Daily quality control tests (8) eliminated the possibility of any malfunctions of the γ-camera during the study period. No visible patient motion was detected in either group. The clinical characteristics of the study population are presented in Table 1.
Clinical Characteristics of Study Population
Upward creep was found in 53% (54/101; range, 1.4–14.5 mm) and 55% (56/101; range, 1.3–14.5 mm) of patients in group A and in 89% (88/99; range, 2.6–22.3 mm) and 86% (85/99; range, 1.5–18.4 mm) of patients in group B in stress and rest SPECT studies, respectively. The difference between the measurements derived from consecutive cine images (the 32nd and 33rd frames) was statistically significant (p < 0.001) in the stress and rest cine images of both groups (Table 2). Allowing a 5-min bed rest before acquisition in group A caused a prominent, statistically significant (P < 0.001) decrease in upward creep of the heart (Table 2).
Results of Measurements* from Cine Images
Upward creep of the liver was also detected between the first- and fifth-minute images of the dynamic acquisition (Table 3), and the increase was statistically significant (p < 0.001).
Results of Measurements* from Dynamic Images
DISCUSSION
The results of this study showed that a 5-min bed rest before SPECT acquisition decreases upward creep of the heart by more than 50%. Gravity has important physiologic effects on the functions and positions of organ systems, and a 5-min bed rest before SPECT acquisition seems to provide enough time for the heart to adapt itself to its new position caused by the effect of the change in gravitational direction on the organs. In our study, we also showed upward creep of the liver on dynamic acquisitions by tracking the dome of liver. Upward creep of the liver also signifies vertical motion of the diaphragm, which comes into close physical contact with the heart. Besides gravity, many other factors, such as pulmonary volume effects and diseases, can probably affect the range of vertical motion of the diaphragm or heart after a change in posture (20–22).
It has been reported that upward creep is probably related to a transient increase in mean total lung volume after exercise (1), and translation of the heart has usually been reported to be common during imaging after exercise (4,5). However, we detected vertical motion of the heart after both rest and stress SPECT acquisitions. Thoracic-abdominal functional reserves of respiration dependent on the spatial positioning of the body were found to be the factor that determines the magnitude with which the thorax and diaphragm contribute to the breathing volume (14). If we consider the underlying physiologic mechanism for upward creep, this kind of motion should be expected in every change of body position from erect to supine.
Poststress motionlike artifacts have been reported to be caused by the use of a dual-head γ-camera for 201Tl myocardial SPECT (23). Actually, the use of a dual-head γ-camera does not cause this motionlike artifact but instead helps to detect this physiologic phenomenon.
Patient motion remains a significant source of unsatisfactory cardiac SPECT examinations. Motion-induced perfusion defects are affected by the type, amount, and timing of motion and the number of camera detectors (4,11). The different motion correction techniques are not perfect, and manual correction by an experienced technologist has proven to be the most accurate (24). Although detection is important, postacquisition attempts to correct such artifacts are incomplete and, optimally, must be prevented (2). Therefore, our approach is a physiologic method and is a preventive measure for an expected motion artifact. It also obviates motion correction programs. Moreover, it does not prolong the study time significantly in routine cardiology practice.
Although the frequency of upward creep has been estimated to be 16%–29% (1,5), it was much more common in our study both for group A and for group B. A possible explanation for this discrepancy may be our use of a dual-head γ-camera for stress and rest SPECT acquisitions, allowing us to detect the beginning and end points of physiologic vertical motion of the heart by comparing the first frame of the first detector with the last frame of the second detector. The greatest amount of motion is seen between these 2 consecutive frames because of the interval between them. Therefore, dual-head γ-cameras are optimal for detecting physiologic vertical motion of the heart.
Mester et al. have reported that clinically significant upward creep of the heart during stress SPECT acquisition was relatively rare (5). A possible explanation for this discrepancy between their results and ours may be that they performed a supine ergometric stress test on their patients and started the tomographic image acquisition within 5 min. Besides, they used a single-head γ-camera in their study, and motion artifacts affect acquisitions with double-head detectors more than acquisitions with single-head detectors (25). The number of affected frames depends on the type (returning or nonreturning) and the time sequence of the motion. It has also been reported that with regard to upward creep, the defect was more extensive in motion simulations using a double-head detector than in those using a single-head detector (26).
CONCLUSION
Although myocardial perfusion imaging with SPECT is an accurate and reliable diagnostic study, artifacts must be avoided, or detected and corrected, to minimize the rate of false-positive results. The current study analyzed the effect of a physiologic measure to decrease the upward creep of the heart that occurs during SPECT acquisitions. We can say that at least a 5-min bed rest in the supine position on the imaging table before both rest and stress SPECT acquisitions significantly decreases vertical motion of the heart and may help avoid misinterpretations of myocardial perfusion SPECT results.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 12, 2006.
- Accepted for publication September 5, 2006.





{kind=link}
{kind=link}
{kind=link}