


Abstract
A 55-y-old patient with multiple myeloma presented for restaging after chemotherapy and radiation. The patient had undergone vertebroplasty of multiple thoracic vertebrae because of painful compression fractures. The 18F-FDG PET images showed increased activity at the T8 and T10–T12 vertebral bodies. Comparison of the attenuation-corrected and non–attenuation-corrected images demonstrated that the activity was due to an artifact of attenuation correction. The CT scan correlated the sites of vertebroplasty to the 4 foci of increased uptake of 18F-FDG. The increasing use of vertebroplasty for malignant spinal fractures warrants vigilance for this artifact.
Improper attenuation correction of high-density materials within patients can result in artifacts on CT images. Vigilance for these artifacts is essential to prevent misdiagnosis of disease recurrence.
CASE REPORT
A 55-y-old patient with multiple myeloma received chemotherapy and radiation and then presented for restaging by 18F-FDG PET/CT. Studies have demonstrated the utility of 18F-FDG PET in the evaluation of multiple myeloma (1–4). Before the therapy, the multiple myeloma had caused extensive lytic lesions in the patient’s spine, resulting in compression fractures at multiple levels. Subsequently, the patient underwent vertebroplasty of multiple thoracic vertebrae to relieve the debilitating pain of these compression fractures. In vertebroplasty, a cement mixture consisting mostly of polymethylmethacrylate is injected through a needle into porous bone, with the porosity commonly caused by osteoporosis but also by malignancy as in this case (5–8). This cement reinforces the bone to reduce further fracture.
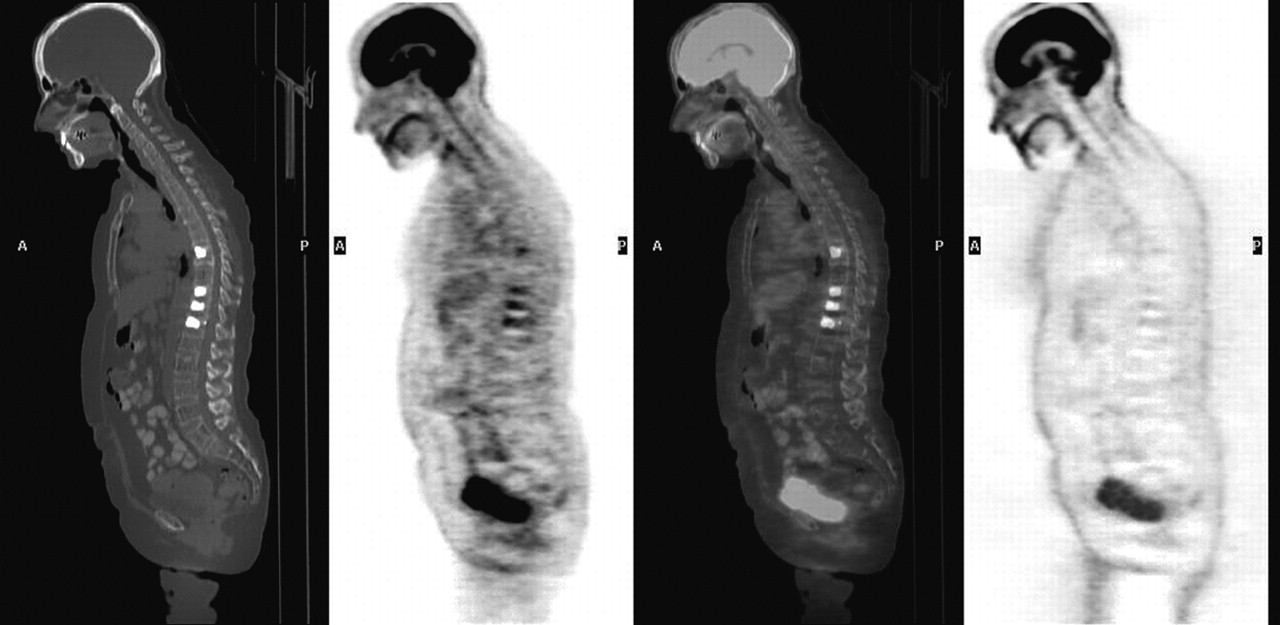
The PET/CT scan was performed on a Discovery ST 16-slice PET/CT camera (GE Healthcare), with the protocol for attenuation correction adjusted for use of oral contrast material. The 18F-FDG PET images showed increased activity at the T8 and T10–T12 vertebral bodies (Fig. 1). Comparison of the attenuation-corrected and non–attenuation-corrected images demonstrated that the activity was due to an artifact of attenuation correction (Fig. 1). The CT scan correlated the sites of vertebroplasty to the 4 foci of increased uptake of 18F-FDG. The cement for the vertebroplasty was determined to have a density of 2,000–3,000 HU (much denser than normal bone). PET/CT uses the transmission scan from the CT as a density map for attenuation correction of the measured activity (9). In this case, the attenuation correction algorithm added back too many counts to compensate for attenuation by the extremely dense cement.
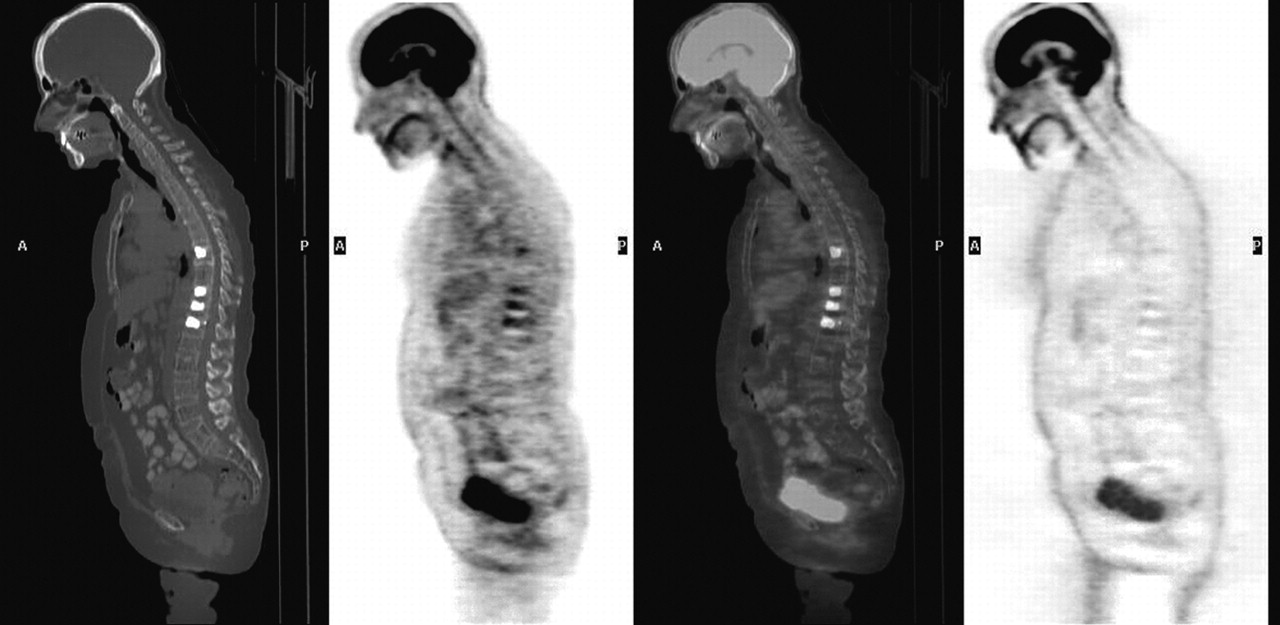
Images of CT, attenuation-corrected PET, fused PET/CT, and non–attenuation-corrected PET in sagittal plane are shown, respectively, from left to right. Increased activity at T8 and T10–T12 was not present on non–attenuation-corrected images and therefore was an artifact of attenuation correction from vertebroplasty material.
DISCUSSION
The increasing use of vertebroplasty for benign and malignant compression fractures warrants vigilance for this artifact. If the artifact had not been caught in this case, the patient would have been misdiagnosed with recurrence of disease and received more chemotherapy. Finally, the lesson learned from this case can also be applied to other causes of artifactual metastases from improper attenuation correction of high-density materials within patients (10–13).
Footnotes
For correspondence or reprints contact: Phillip H. Kuo, MD, PhD, Department of Diagnostic Radiology, Yale University School of Medicine, 333 Cedar St., P.O. Box 208042, New Haven, CT 06520-8042.
E-mail: phillip.kuo{at}yale.edu





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.