


Abstract
Objectives: It is widely accepted that exercise-induced stunning has an impact on left ventricular ejection fraction (EF); yet, despite the recommendations of the American Society of Nuclear Cardiology, many departments only perform gated SPECT on stress studies. The aim of this investigation was to determine the relationship between rest EF and stress EF in myocardial perfusion studies and to identify possible predictors of variability.
Methods: This study was a retrospective cross-sectional study of 133 patients (266 studies) undergoing myocardial perfusion SPECT. Automated computer-generated functional data (end-diastolic volume, end-systolic volume [ESV], and EF) for rest and stress studies were correlated as matched pairs and analyzed with respect to the following variables: age, sex, stress method, time between stress and scanning, and presence or absence of pathology scintigraphically. Differences in matched EF pairs (ΔEF) and transient dilatation were also determined.
Results: Matched pairs of rest EF and stress EF demonstrated excellent correlation (0.90) with no significant difference noted (P = 0.15). Bland–Altman analysis demonstrated a mean ΔEF of −0.65% (95% confidence interval [CI], −1.54% to 0.23%) with 94% of data points within the 95% limits of agreement. No statistically significant difference was determined between the mean ΔEF and the hypothetic mean of 0 (P = 0.15). A time between stress and scanning of <45 min was shown to be predictive of a negative ΔEF (P = 0.04). Transient dilatation was shown to be predictive of a negative ΔEF (P = 0.01). Resting ESVs between 25 and 50 mL were shown to be predictive of a negative ΔEF (P = 0.02). A stress EF of <50% was also shown to be predictive of a negative ΔEF (P = 0.003).
Conclusion: No statistically significant difference between stress and rest EF was demonstrated and no trend was identified toward either under- or overestimation of the stress EF with a ΔEF. A negative ΔEF was, however, predicted by transient dilatation of >1.0, a time between stress and scanning of <45 min, a stress EF of <50, and an ESV between 25 and 50 mL. Gated SPECT performed on both stress and rest studies may provide a mechanism to predict exercise-induced stunning and transient dilatation.
- ejection fraction
- rest versus stress
- myocardial perfusion
- gated SPECT
- exercise-induced stunning
- transient dilatation
Gated SPECT provides important diagnostic and prognostic information over SPECT alone by using electrocardiographically linked myocardial perfusion images to provide ventricular wall motion and thickening information. This additional information allows both regional perfusion and global function to be assessed simultaneously at no extra cost in terms of acquisition time (1).
Although the perfusion information obtained by the gated SPECT acquisition reflects the perfusion at the time of injection, the ventricular function information is that occurring at the time of the acquisition. As a result, the ventricular function generally reflects the resting condition of the myocardium whether the patient is injected at rest or stress (2). The time after stress that the SPECT acquisition is commenced is one factor that may determine whether the functional information is considered resting or poststress.
A large proportion of nuclear medicine departments perform gated SPECT only on the stress myocardial perfusion data. Wheat et al. (3) reported that 58.8% of departments in Australia perform gating on the stress study only. DePuey (4) reports that there is significant evidence to suggest that functional information acquired after stress is different than that acquired at rest. Consequently, the American Society of Nuclear Cardiology recommends that gated SPECT is performed on both stress and rest studies (5).
It is widely accepted that exercise-induced stunning has an impact on left ventricular ejection fraction (EF) determination; however, there is no agreement on the duration of this phenomenon (6). Lee et al. (7) report stunning after exercise to be problematic out to 1 h after stress. Johnson et al. (8) suggested that 36% of patients have their results affected by postexercise stunning.
There is a significant breadth of literature highlighting the underestimation of EF due to stunning after stress on gated myocardial perfusion SPECT functional parameters in patients with stress-induced ischemia (8–11); however, several authors have also reported this phenomenon in patients with myocardial infarction (10,12). It is important to note, however, that the myocardial perfusion defects themselves do not cause the variation in left ventricular EF (10). The difference between stress and rest EF calculations (ΔEF) for nonischemic patients has been reported as +1% (i.e., stress greater than rest), whereas ΔEF in patients with stress-induced ischemia has been reported as −4% (i.e., rest greater than stress) (P < 0.01) (9). Dziuk et al. (13), however, reported no statistically significant difference between nonischemic ΔEF (−6.0% ± 5.1%) and ischemic ΔEF (−5.0% ± 4.8%).
The aim of this investigation was to determine the relationship between rest EF and stress EF determined using quantitation of gated myocardial perfusion SPECT and to identify possible predictors of variability.
MATERIALS AND METHODS
Study Population Demographics
This study was a retrospective cross-sectional study of 133 patients undergoing myocardial perfusion SPECT. The study population consisted of 266 myocardial perfusion studies (133 rest and 133 stress). The age of the study population was normally distributed (P = 0.06), with a mean of 67.9 y, a median age of 69.5 y, and an age range of 43–88 y. The study population consisted of 74 women (55.6%) and 59 men (44.4%).
Study Subjects and Protocol
All data were acquired following 2-d stress/rest or 2-d rest/stress myocardial perfusion SPECT protocols. All myocardial perfusion SPECT studies used a 740-MBq dose of 99mTc-tetrofosmin (Nycomed-Amersham). A triple-detector gantry was used to acquire all patient data. All data acquisitions used low-energy, high-resolution collimation with step-and-shoot mode, elliptic orbits, and a 64 × 64 matrix. The zoom was 1.23 and projections were acquired at 3° intervals for 20 s per projection to provide a total acquisition time of 15 min. All patients were positioned supine with their feet into the gantry for an 8-interval gated SPECT acquisition. Patient stress was achieved using dipyridamole (persantin) (27.8%), treadmill exercise (50.4%), dobutamine (2.3%), or a combined protocol of dipyridamole (persantin) and exercise (19.6%). All data were reconstructed using a 180° filtered-backprojection algorithm.
Automated computer-generated left ventricular volumes and left ventricular EFs were obtained from short-axis slices of electrocardiographically gated rest and stress myocardial perfusion SPECT datasets using quantitative gated SPECT (QGS) software (Cedars Sinai Medical Center, Los Angles, CA). Left ventricular EFs measured from gated myocardial perfusion SPECT using QGS have been reported to have good-to-excellent agreement with a variety of gold standards (14–18). The quantitated functional data (end-diastolic volume [EDV], end-systolic volume [ESV], and EF) for each patient study were evaluated as rest and stress matched pairs and analyzed with respect to the following variables: age, sex, stress method, time between stress and scanning, and presence or absence of pathology scintigraphically. The ΔEF (the difference between matched pairs) and transient dilatation (ratio of stress EDV to rest EDV) were also determined.
Data collection and analysis were approved by the Ethics in Human Research Committee of Charles Sturt University.
Statistical Analysis
The statistical significance was calculated using χ2 analysis for nominal data and the Student t test for continuous data. The F test ANOVAs were used to determine statistically significant differences within grouped data. A P value < 0.05 was considered significant. Normality of distribution was determined using the Shapiro–Wilk W test, with a P value < 0.05 indicating that the data vary significantly from normality. Confidence intervals (CIs) were used with 95% confidence. Bland–Altman analysis (19) was used to assess agreement between pairs. Relative risk (risk ratio) was used to determine the strength of association between exposure and outcomes, with a risk ratio of 1.5 indicative of the exposure of interest being 1.5 times more likely to result in the outcome of interest.
RESULTS
The mean time after injection that the stress acquisition was commenced was 49.7 min (95% CI, 44.7–54.8 min), with a range of 30–100 min. Patient datasets were normal for 67.9% (76/112) of patients (95% CI, 58.7%–75.8%), whereas fixed defects were demonstrated in 12.5% (14/112), reversible defects in 11.6% (13/112), and a mix of fixed and reversible defects in 8.0% (9/112) of patients.
The following results are summarized in Table 1. The rest EF demonstrated normal distribution (P = 0.80) about a mean of 56.9% (95% CI, 55.0%–58.9%), with a range of 22%–86%. The stress EF was normally distributed (P = 0.62) about a mean of 56.3% (95% CI, 54.3%–58.3%), with a range of 19%–93%. Both rest and stress EFs showed a median of 57%. Rest EDV demonstrated a mean of 100.2 mL (95% CI, 93.9–106.6 mL), a median of 94 mL, and a range of 37–211 mL. Rest ESV demonstrated a mean of 46.2 mL (95% CI, 41.5–50.8 mL), a median of 39 mL, and a range of 7–152 mL. Stress EDV demonstrated a mean of 99.5 mL (95% CI, 93.2–105.9 mL), a median of 92 mL, and a range of 30–209 mL. Stress ESV demonstrated a mean of 46.5 mL (95% CI, 41.8–51.2 mL), a median of 41 mL, and a range of 2–169 mL. Overlaps of 95% CIs do not support a statistical difference between means.
Summary of Functional Data for Stress and Rest Studies
Matched pairs of rest EF and stress EF demonstrated excellent correlation (0.90) with no significant difference noted (P = 0.15) (Fig. 1). Rest and stress EDV matched pairs also correlated well (0.93) with no significant difference noted (P = 0.53), whereas ESV matched pairs showed a 0.94 correlation and no significant difference (P = 0.69).
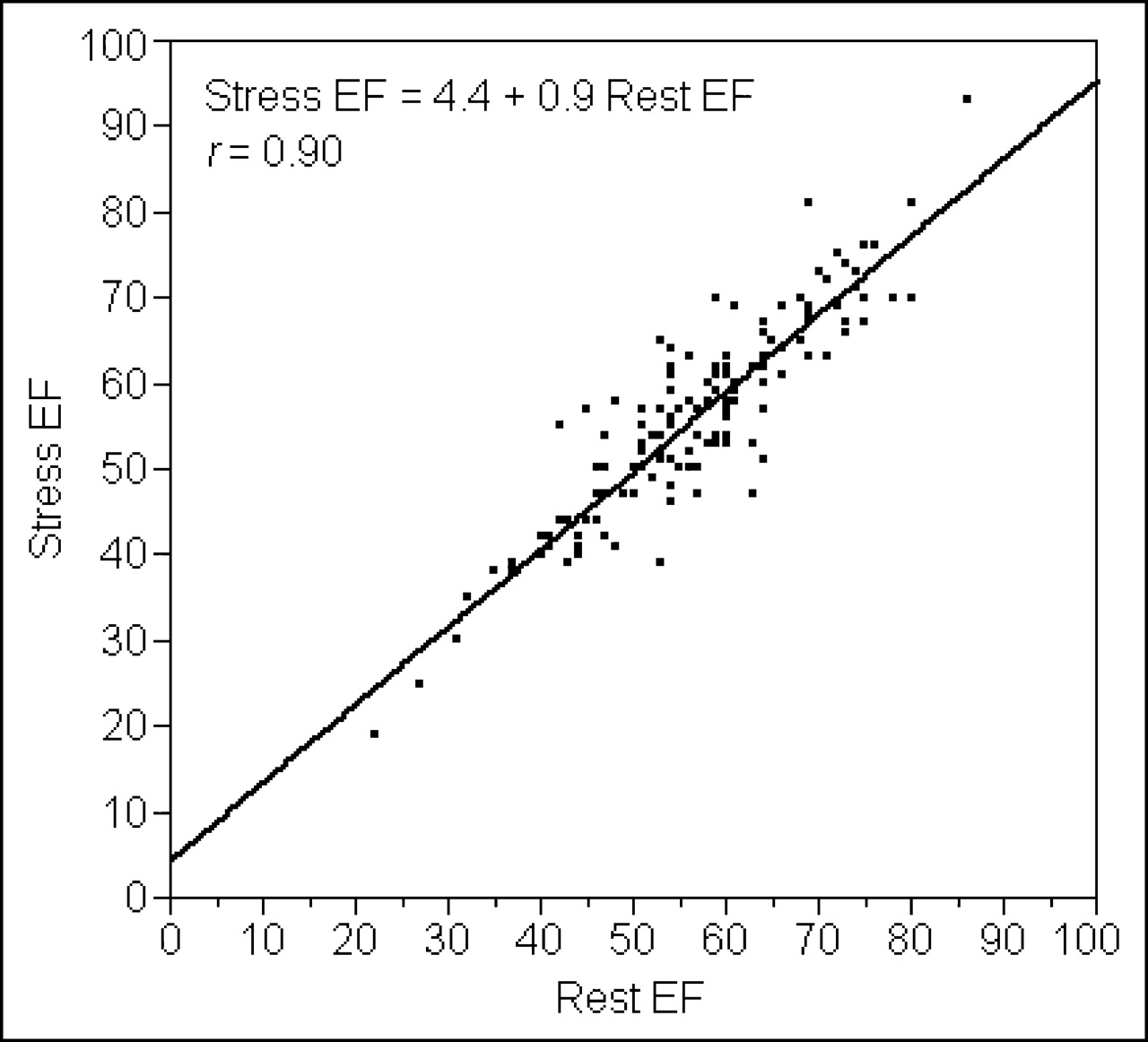
Bivariate fit of rest EF and stress EF for matched pairs.
Bland–Altman analysis (19) was used to more thoroughly evaluate these relationships by relating the mean of matched pairs to the difference between matched pairs. The mean ΔEF was −0.65% (95% CI, −1.54% to 0.23%), with a median of −1.0% and a range of −16% to 13%, where a negative result indicates a rest EF greater than the stress EF (Fig. 2). The 95% limits of agreement contained 94% of the data points. No statistically significant difference was determined between the mean ΔEF and the hypothetic mean of 0 (P = 0.15).
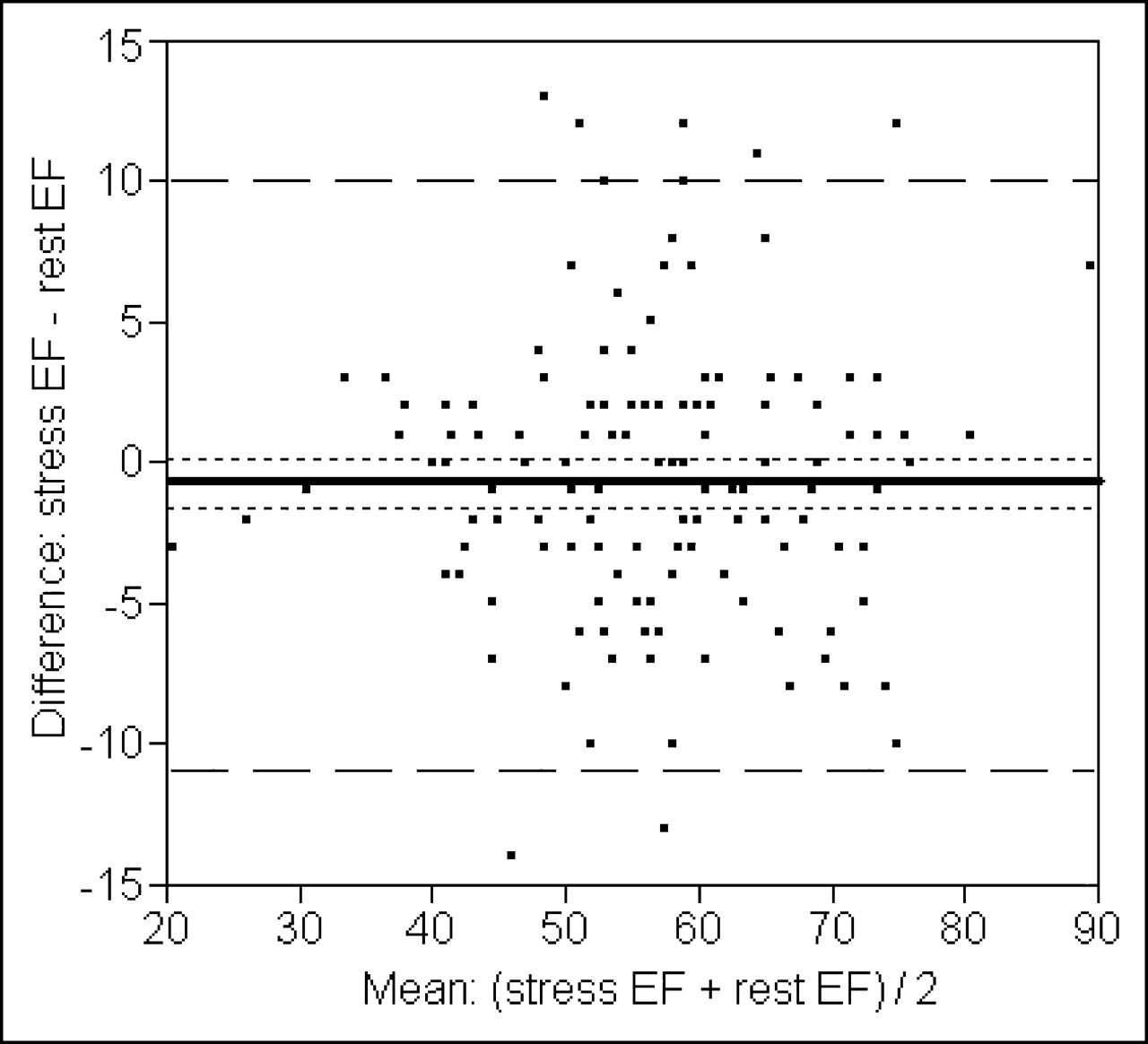
Bland–Altman analysis of mean of stress/rest matched pairs vs. ΔEF shows no trend toward under- or overestimation of stress EF. Mean stress EF was 56.3%, mean rest EF was 56.9%, and mean difference in EF indicated by solid horizontal line was −0.65%. Outer dashed lines represent 95% limits of agreement, whereas inner dotted lines represent 95% CI of EF difference.
A weak positive correlation was noted between time after stress that scanning was commenced and ΔEF (correlation coefficient, 0.13)—that is, the longer the delay between patient stress and commencement of scanning, the less likely a negative ΔEF. A time between stress and scanning of ≤45 min was shown to be predictive of a negative ΔEF comparing the mean ΔEF (−0.96) to a hypothetic mean of 0 (P = 0.04). Comparing the mean ΔEF for times >45 min (1.0), however, was not predictive of a negative ΔEF (P = 0.46). An abnormal scan finding was not shown to be predictive of a negative ΔEF (P = 0.32). Interestingly, the mean time after stress that scanning was commenced for patients with normal results was 45.7 min compared with 61.7 min for those with reversible ischemia. This may be related to a greater need for observation or recovery for ischemic patients after stress.
There was a weak negative relationship (correlation coefficient, 0.24) between ΔEF and poststress transient dilatation of the left ventricle (Fig. 3), which suggests that patients with a negative ΔEF (stress EF lower than rest EF)—despite the stress study being performed at rest—are more likely to have transient dilatation of the left ventricle after stress. This is related to pathology or the stress method used. Transient dilatation was shown to be predictive of a negative ΔEF comparing the mean ΔEF for studies demonstrating transient dilatation ratios ≥1 (−1.6) with a hypothetic mean of 0 (P = 0.01). A transient dilatation ratio of <1 (0.16 mean ΔEF), however, was not shown to be a predictor (P = 0.81).

Bivariate fit of transient dilatation and ΔEF demonstrates weak negative correlation suggesting negative ΔEF may be associated with prolonged poststress transient dilatation.
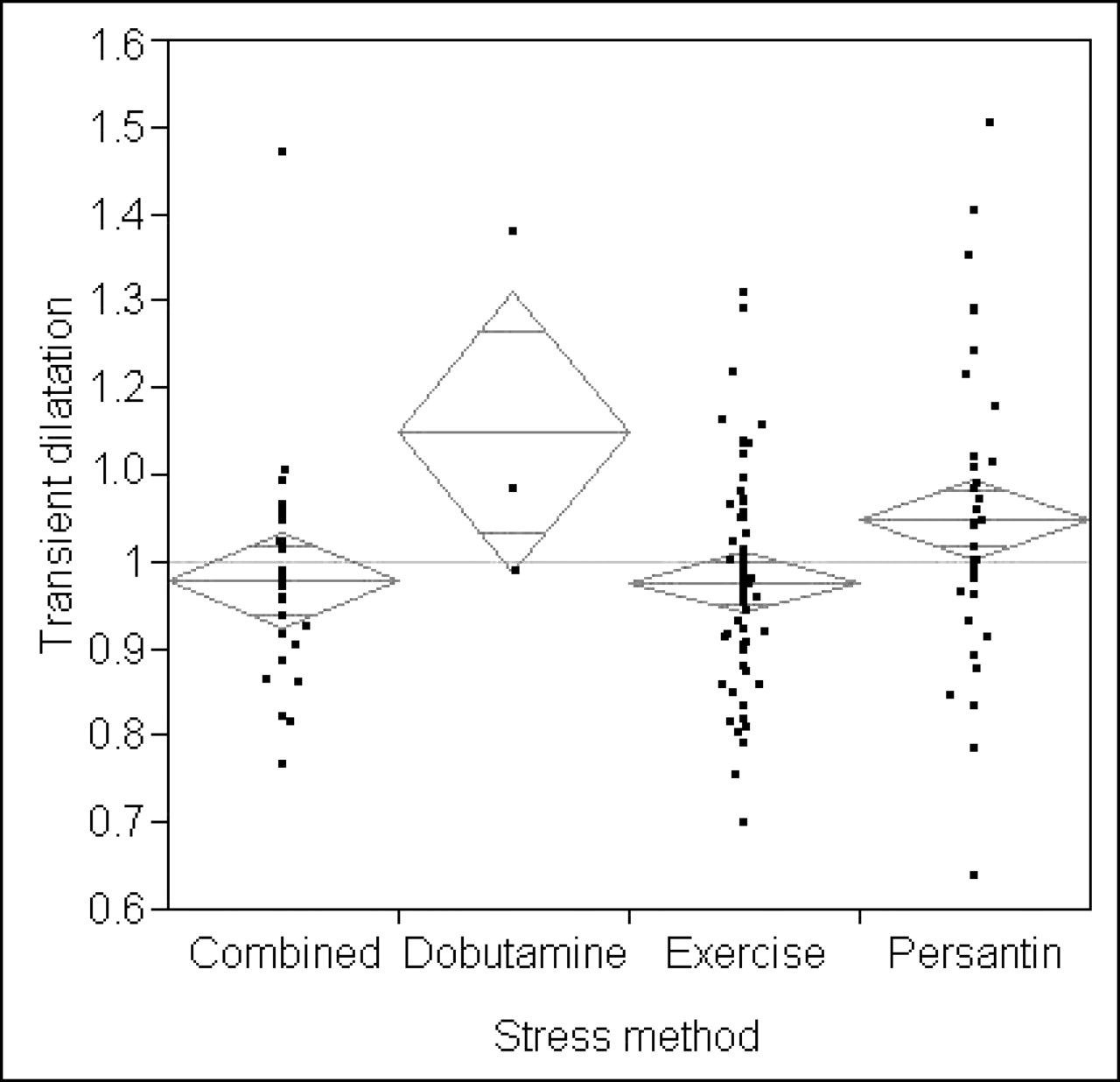
Mean transient dilatation demonstrated a statistically significant difference in the grouped data (P = 0.02) when comparing stress methods with dipyridamole (persantin) stress testing, demonstrating a mean transient dilatation of 1.05 compared with 0.98 for exercise, 0.98 for combined exercise/dipyridamole (persantin), and 1.15 for dobutamine (Fig. 4). Specifically, a statistically significant difference in the mean transient dilatation ratio was noted comparing persantin stress with exercise stress (P = 0.01), persantin and combined persantin/exercise (P = 0.05), dobutamine and exercise (P = 0.04), and dobutamine and combined persantin/stress (P = 0.05). Stress method, however, was not shown to be predictive of a negative ΔEF (P = 0.37).
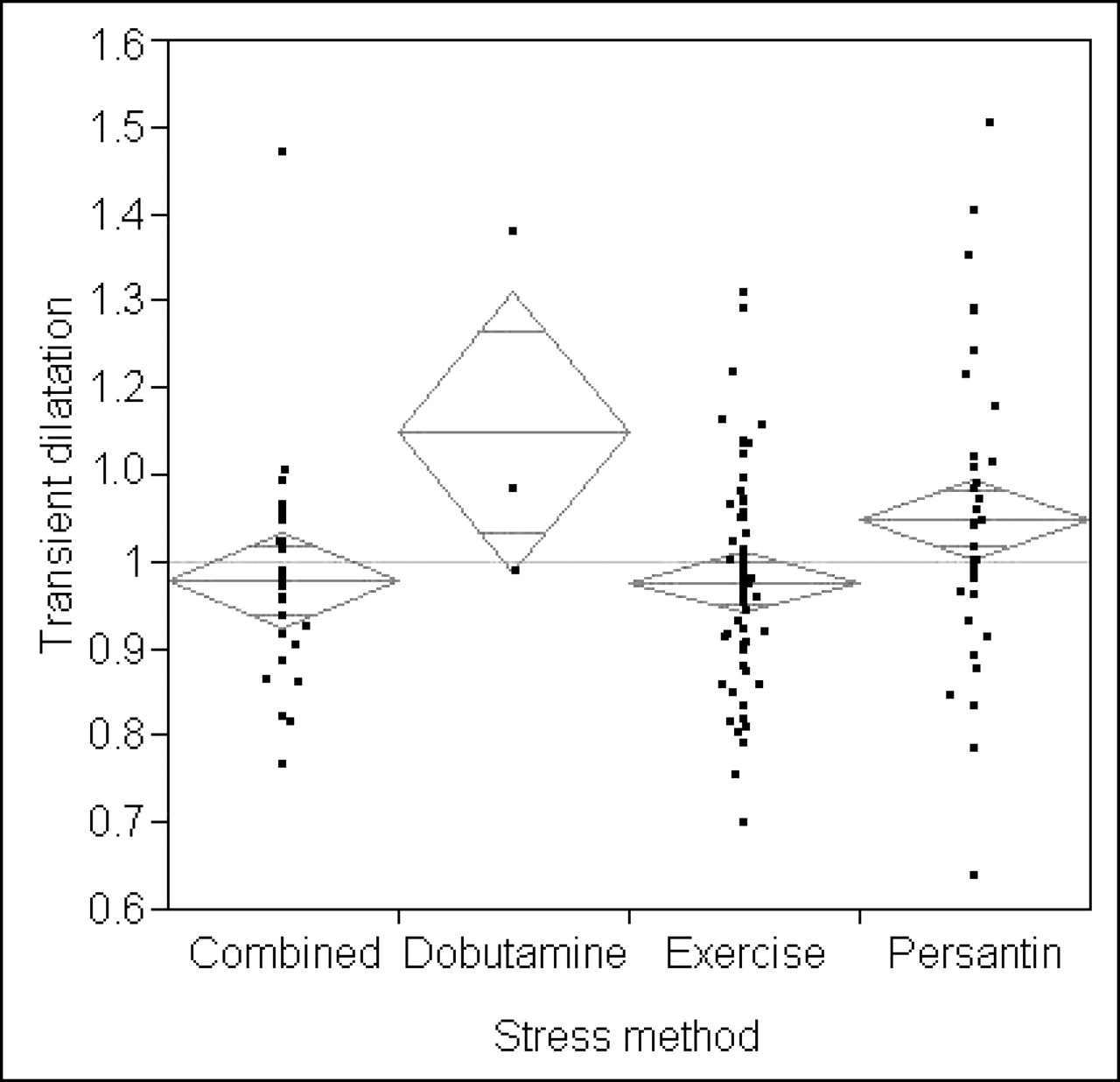
One-way ANOVA of transient dilatation by stress method demonstrating, despite small overlap of 95% CIs (diamonds), a statistically significant difference between mean transient dilatation for exercise stress and combined exercise/persantin compared with persantin stress (P = 0.02).
The presence of reversible defects correlated with a higher mean transient dilatation (1.1) when compared with fixed defects (0.99), no defects (0.99), and mixed fixed and reversible defects (0.98), although no statistically significant difference was noted in the grouped data (P = 0.07) (Fig. 5). Specifically, however, a statistically significant difference was noted in the mean transient dilatation ratio between studies with reversible defects and fixed defects (P = 0.048) and between reversible defects and normal studies (P = 0.01).

One-way ANOVA of transient dilatation by scintigraphic findings demonstrating overlap of 95% CIs (diamonds) and no statistically significant difference between mean transient dilatation across scintigraphic findings (P = 0.07) despite the higher mean score of the reversible category.
Resting EDV was shown to be predictive of a negative ΔEF comparing the mean ΔEF for studies with an EDV of <100 mL (−1.2) with a hypothetic mean of 0 (P = 0.05). A rest EDV of >100 mL (P = 0.94), a stress EDV of <100 mL (P = 0.29), and a stress EDV of >100 mL (P = 0.32) were all shown to be not predictive of ΔEF. Resting ESV was shown to be predictive of a negative ΔEF comparing the mean ΔEF for studies with an ESV of <50 mL (−1.4) with a hypothetic mean of 0 (P = 0.02). A rest ESV of >50 mL (P = 0.34), a stress ESV of <50 mL (P = 0.43), and a stress EDV of >50 mL (P = 0.18) were all shown to be not predictive of ΔEF.
Resting EF was shown to be predictive of a negative ΔEF comparing the mean ΔEF for studies with an EF of ≥50% (−1.1) with a hypothetic mean of 0 (P = 0.04). Stress EF was also shown to be predictive of a negative ΔEF using the mean ΔEF for studies with an EF of <50% (−2.55) (P = 0.003). A rest EF of <50% (P = 0.96) and a stress EF of ≥50% (P = 0.95) were not shown to be predictive of ΔEF.
DISCUSSION
Hachamovitch et al. (20) reported that the addition of gated information provided statistically incremental prognostic value with a 5-fold increase in prognostic information. Using an automated gated SPECT algorithm, Sharir et al. (21) showed that a left ventricular systolic volume of ≤70 mL was related to a low mortality rate even in patients with severe perfusion abnormalities. Sharir et al. also showed survival benefits when the left ventricular EF is ≥45%. These conclusions rely on the determination of function information—including the EF and ventricular volumes—to be robust between rest and stress studies, for the gamut of coronary pathologies and through procedural variations. Gayed et al. (10), however, concluded that myocardial perfusion defects, regardless of size and extent, seem to affect the accuracy of left ventricular EF calculation using QGS.
DePuey (4) reported that there is significant evidence to suggest that functional information acquired after stress is different from that acquired at rest; however, this investigation demonstrated no statistical difference between stress and rest in terms of functional information (P = 0.15 for EF). Moreover, Bland–Altman analysis demonstrated no trend toward either under- or overestimation of functional parameters determined on the stress data with a ΔEF of −0.65% (95% CI, −1.54%–0.23%) and a P value of 0.15 compared with a hypothetic mean of 0. Despite no statistical correlation being noted when comparing ΔEF with age (P = 0.45), sex (P = 0.51), stress method (P = 0.72), time after stress that scanning is commenced (P = 0.43), or the presence or absence of cardiac pathology (P = 0.40), several possible predictors of a negative ΔEF were identified (Table 2).
Statistical Significance and Relative Risk Calculated for Independent Predictors of a Negative ΔEF
For rest EDVs between 70 and 100 mL, 71.4% (10/14) demonstrated a time after stress that scanning was commenced of <45 min. A rest EF of >70% was always (18/18) associated with both an EDV of <100 mL and an ESV of <40 mL. A stress EF of <50% was associated with an EDV of >100 mL in 81.8% (27/33) of cases and an ESV of >40 mL in 97.0% (32/33) of cases. A rest EF of >70% may simply appear predictive because of possible errors calculating higher EFs (e.g., statistical errors, edge detection errors, low counting rates, small hearts, etc.)—hence, the association with smaller hearts. A stress EF of <50% is perhaps more predictive of a negative ΔEF because of the possibility of an underlying pathologic process that decreases stress EF compared with rest (e.g., poststress stunning)—hence, the association with larger hearts.
Interestingly, stress volumes were not shown to be predictive of a negative ΔEF, whereas rest volumes were shown to be predictive. One might postulate that the stress volumes have suffered the impact of stunning and, thus, are not predictive. It follows that the rest volumes within the normal range are most likely to demonstrate a negative ΔEF. One speculates that this resulted from less reliable calculations in smaller hearts, whereas resting pathology may be present in larger hearts, each confounding the outcome of interest. Transient dilatation, therefore, predicts a negative ΔEF because it presents the possibility of both stress-induced stunning and inadequate time after stress for recovery of function. Surprisingly, pathology was not shown to be predictive of a negative ΔEF, but this observation may be confounded by the longer mean time after stress scanning was commenced for studies demonstrating ischemia (61.7 min) compared with normal studies (45.7 min).
Independent predictors of variations in ΔEF include the presence of ischemia or increased heart rate during the stress acquisition compared with the rest (9). There are several causes of increased heart rate during the stress study that are not related to stress-induced ischemia (e.g., inadequate time for recovery after stress, stress-induced anxiety, nausea after pharmacologic stress, anxiety of the scan, etc.) (22). The findings of this study support an impact of stress-induced stunning on ΔEF.
A stress EF alone may be an unreliable tool for evaluating cardiac function in the patient with stress-induced stunning. Moreover, stress-induced stunning cannot be readily identified without the rest EF. Performing both a rest EF and a stress EF on patients may allow identification of poststress stunning that may aid in diagnosis, particularly in multivessel disease. Determination of the ΔEF may offer a prognostic indicator, improving stratification and patient management, although evidence supporting this hypothesis was beyond the scope and resources of this study.
CONCLUSION
No statistically significant difference between stress and rest in terms of EF (P = 0.15) was demonstrated and no trend was identified toward either under- or overestimation of the stress EF, with a ΔEF of −0.65% (95% CI, −1.54% to 0.23%). A negative ΔEF was predicted by transient dilatation of >1.0, a time between stress and scanning of <45 min, a stress EF of <50, and an ESV between 25 and 50 mL. Transient dilatation was predicted by a finding of ischemia, dipyridamole (persantin) stress, and a time between stress and scanning of <45 min. Gated SPECT performed on both stress and rest studies may provide a mechanism to predict exercise-induced stunning and transient dilatation.
Acknowledgments
The authors thank the partners and staff at Central Coast Nuclear Medicine for the use of their time, expertise, and resources.
Footnotes
For correspondence or reprints contact: Janelle M. Wheat, BAppSc, MMedRadSc, School of Clinical Sciences, Locked Bag 588, Charles Sturt University, Wagga Wagga 2678, New South Wales, Australia.
E-mail: jwheat{at}csu.edu.au
REFERENCES





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.