


Abstract
Optimal technique for planar bone scanning improves image quality, which in turn improves diagnostic efficacy. Because planar bone scanning is one of the most frequently performed nuclear medicine examinations, maintaining high standards for this examination is a daily concern for most nuclear medicine departments. Although some problems such as patient motion are frequently encountered, the degraded images produced by many other deviations from optimal technique are rarely seen in clinical practice and therefore may be difficult to recognize. The objectives of this article are to list optimal techniques for 3-phase and whole-body bone scanning, to describe and illustrate a selection of deviations from these optimal techniques for planar bone scanning, and to explain how to minimize or avoid such technical errors.
Throughout the world, bone scanning is one of the most commonly performed nuclear medicine examinations. Patients with tumors, trauma, infection, and a variety of other indications undergo 99mTc-diphosphonate bone scanning. Most nuclear medicine departments use predefined protocols that are designed to yield high-quality images (1,2). When executing these bone scan protocols, nuclear medicine technologists usually do not encounter serious technical problems. Working together as a team, nuclear medicine technologists and physicians have great expertise in performing, reviewing, and interpreting planar bone scans. Nonetheless, technical errors that alter the appearance of planar bone scans do occur from time to time (3–7). The benefits of this examination are greatly influenced by the quality of the images. Therefore, a review of both optimal technique for planar bone scanning and technical errors is in order.
TECHNIQUES FOR PLANAR BONE SCANNING
This article presents what the authors believe to be optimal techniques for planar bone scanning (1,2). In particular, the following protocols are suggested: 3-phase planar bone scanning and single-phase, whole-body planar bone scanning. Tables 1 and 2 summarize the first protocol. The second protocol is as follows:
Patient voids just before the acquisition begins.
Technician ensures patient comfort and proper positioning, using additional supports to secure the position, as necessary.
Dual-head γ-camera equipped with low-energy high-resolution collimators is preferred.
A 20% energy window is centered at 140 keV.
A 256 × 1,024 × 16 or greater matrix is used.
Scanning speed is adjusted so that routine (obtained 2–5 h after injection) delayed anterior or posterior whole-body images contain >1.5 million counts. Most often, 10–15 min/m is chosen.
The scan extends from the skull to the ends of the feet, with the pathlength adjusted according to patient height.
Additional spot images are requested if needed.
A Protocol for Digital 3-Phase Planar Bone Scanning
Optimal Image Count for Planar Spot Acquisition
In our experience, these protocols have provided high-quality images for most of the patients referred to our own nuclear medicine department. However, unusual patients or exceptional clinical circumstances may require practitioners to use significantly altered protocols. For example, when called on to examine for possible osteomyelitis of the lumbar spine in a patient weighing over 227 kg (500 lb), one of us used a 1,665-MBq (45 mCi) dose of 99mTc-methylene diphosphonate (MDP) as part of a modified planar and SPECT bone scan protocol. Furthermore, the choice of techniques for bone scanning is critically dependent on the equipment in each nuclear medicine department. Finally, other legitimate approaches exist. For example, some practitioners will acquire an initial spot image of the chest for 500,000 to 1 million counts, after which the remaining spot views are acquired for the same time as the first view. In addition, some practitioners perform whole-body bone scanning with a series of overlapping spot images that cover the skeleton from the anterior and posterior views. Thus, the 2 protocols are presented not as optimal techniques for all places and situations but as a useful guide for readers interested in reviewing the approaches to bone scanning used in their own nuclear medicine departments. Furthermore, for the sake of brevity, pinhole-collimator and other more rarely performed techniques for planar bone scanning are not considered in this article.
When executing bone scan protocols, it is well for one to be aware of how key deviations from optimal technique can degrade image quality. Of course, there are a great number of ways in which one may fail to follow a bone scan protocol, and therefore all possible errors cannot be considered. However, a selection of the most common or important deviations from optimal technique is illustrated in this article. Furthermore, this article concentrates on technical errors related to imaging. For this reason, errors related to radiopharmaceutical preparation are not considered.
Flow-Study and Blood-Pool Imaging
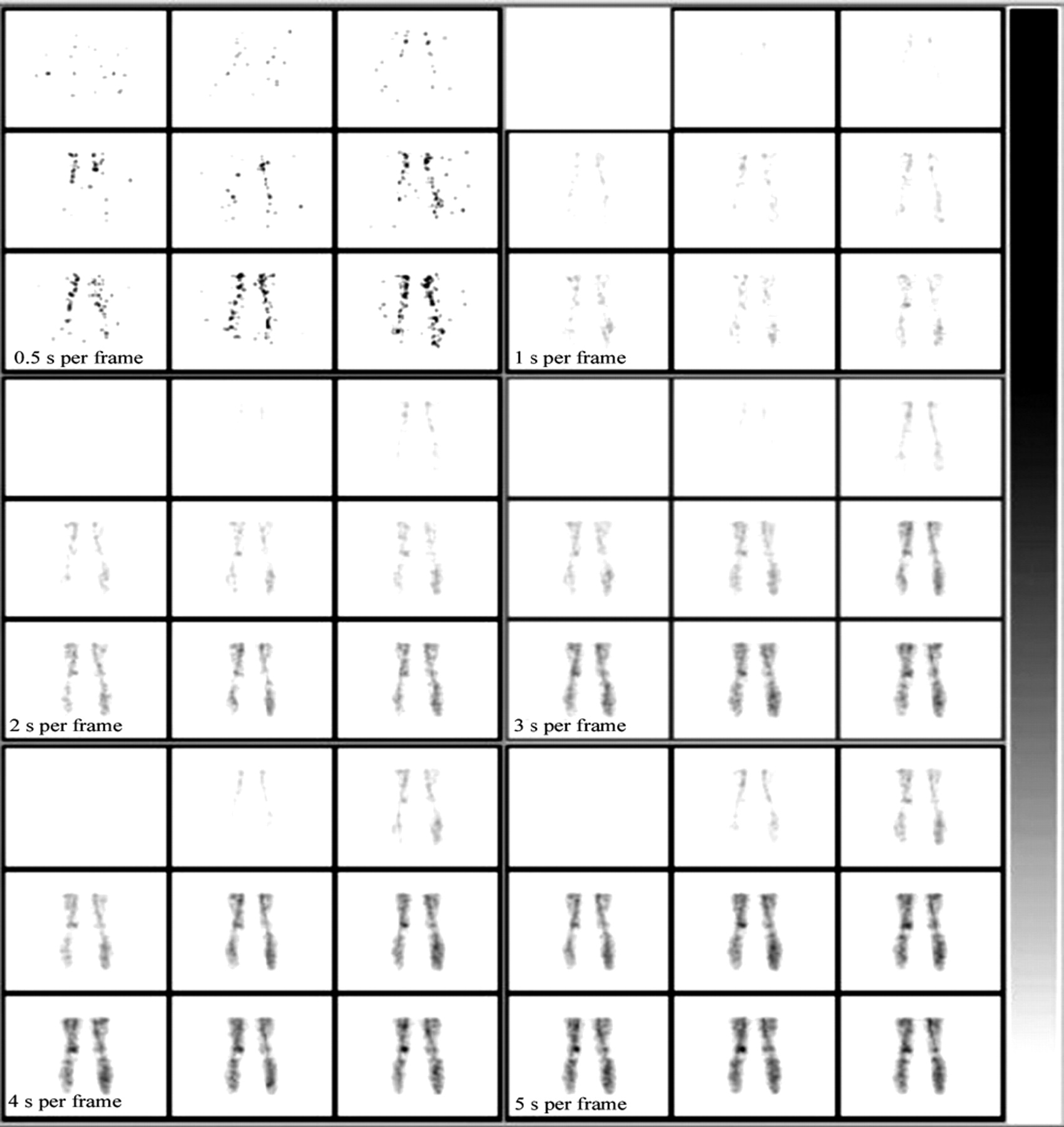
In a flow study, the site of venous injection should be away from the area of clinical concern. The patient should be made comfortable and instructed not to move. Usually, a tourniquet is needed when an antecubital venipuncture is performed. However, prolonged use of the tourniquet will produce reactive hyperemia distal to the site of injection, which will result in increased perfusion on the flow study and increased soft-tissue activity on the blood-pool images. To minimize this problem, the tourniquet is released for at least 1 min after the needle tip is placed in the vein, and the radiopharmaceutical is then injected (8,9). A sharp, single peaked bolus injection should be obtained. Upon intravenous injection of the radiopharmaceutical, the rapid-sequence flow study is captured digitally or on film. Digital imaging allows for postinjection reformatting of the images so as to obtain a slower framing rate. As is shown in Figure 1, images acquired digitally at a rapid framing rate of 0.5 s per frame suffer from low count density and lack of anatomic detail. At this most rapid framing rate, many pathologic states can be obscured. When reframed to 1.0-s intervals, the images show only some improvement. When one is searching for changes in arterial perfusion, such as renal artery or carotid artery stenosis, framing rates of 0.5 or 1.0 s per frame are required. However, imaging of musculoskeletal abnormalities usually does not require depiction of such short-interval changes in arterial perfusion. Rather, anatomic detail and precise localization are important. For example, the increased perfusion associated with osteomyelitis can be adequately imaged at 5.0 s per frame. In many departments, framing rates of between 2.0 and 5.0 s allow interpreting physicians to follow the radiopharmaceutical bolus and identify the relevant vascular and soft-tissue anatomy (2). We prefer 3.0 s per frame. In our department, all 3-phase bone scans are digitally archived. We have found that saving flow-study data framed at 3.0-s rather than 0.5-s intervals expedites both digital storage and any later retrieval.

Effect of framing rate on a flow study. Framing rates of 2 or more seconds per frame display more anatomic structure than is seen at 0.5 s per frame, while preserving much of the sequential changes in perfusion.
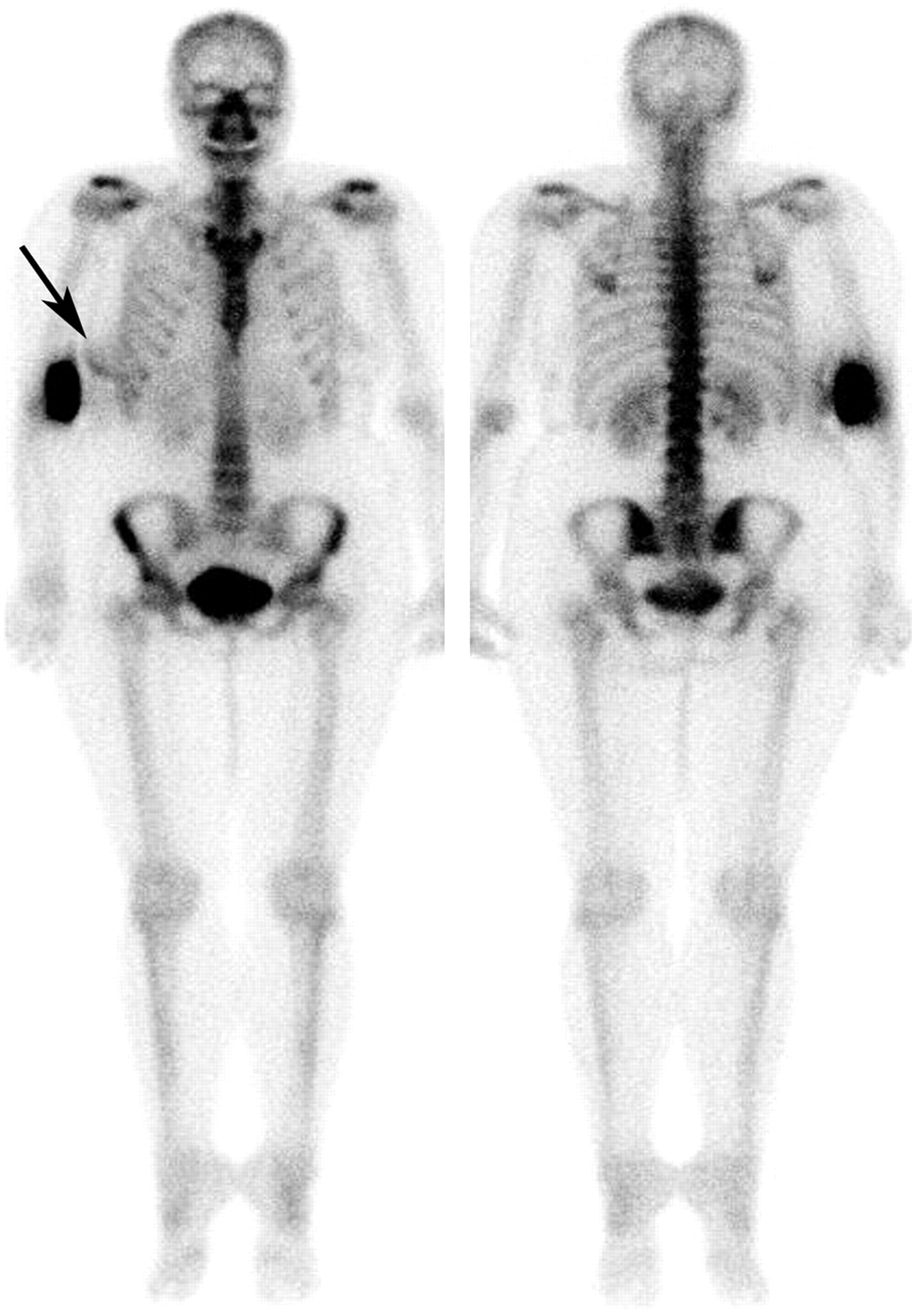
Even the most experienced nuclear medicine technologists will occasionally infiltrate a portion of the injected dose into the perivenous soft tissues. Sites of radiopharmaceutical injection should be marked so that infiltrated doses are not confused with pathologic findings. When 99mTc-MDP is infiltrated into antecubital soft tissues, lymphatic flow of the radiopharmaceutical to the axilla will occasionally result in axillary lymph node uptake (10). Less frequently recognized is apparent uptake in adjacent soft tissues produced by Compton scatter from an infiltrated dose (6). For example, Figure 2 shows a rim of activity along the lateral margin of the right breast due to Compton scatter from a partially infiltrated injection into the right antecubital vein. If not recognized as Compton scatter, this finding might be interpreted by physicians as significant breast abnormality.
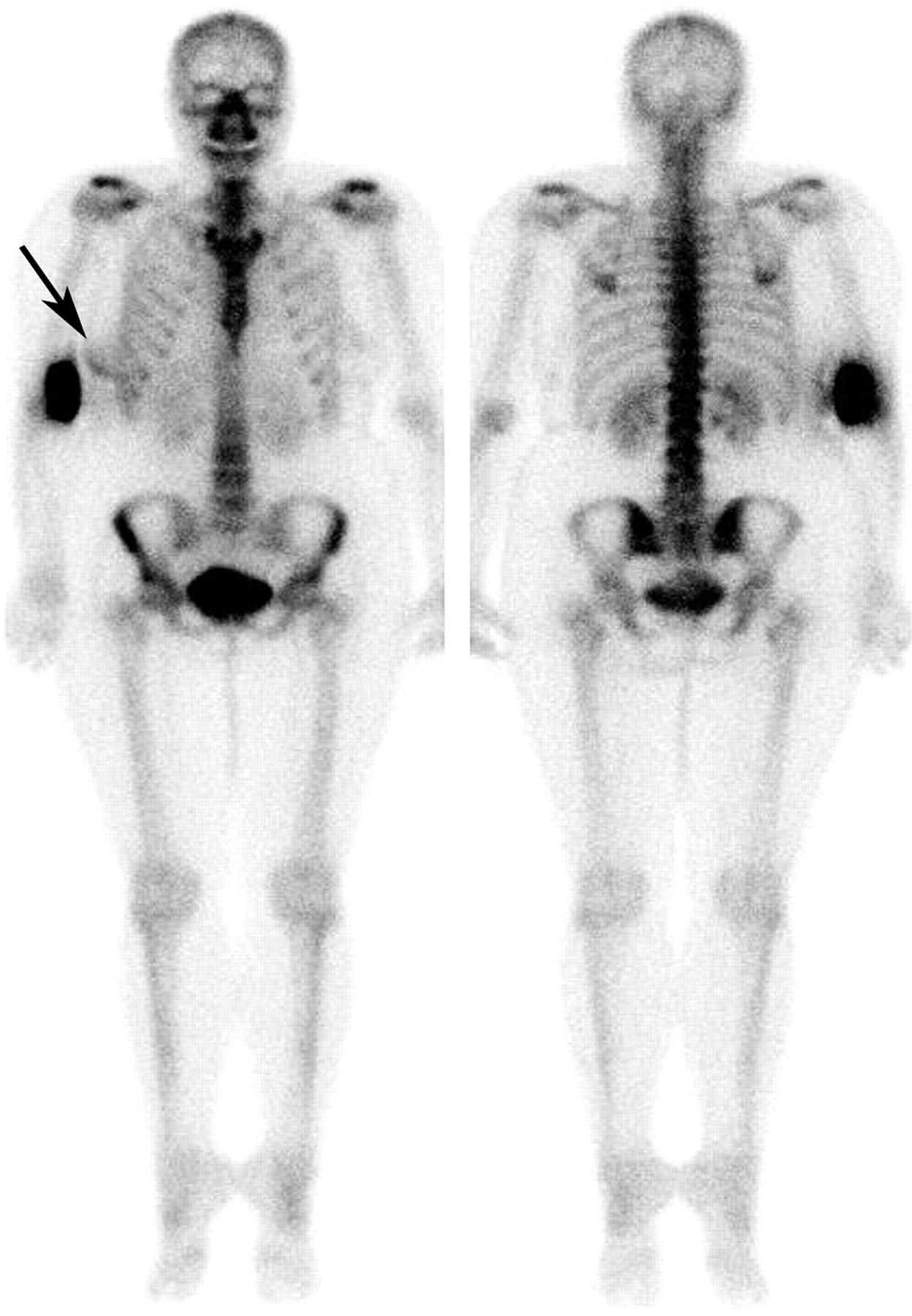
Compton scatter from a partially infiltrated dose (anterior view on left, posterior view on right). Because of this scatter from the site of infiltration in the right arm, there is apparent increased uptake in the adjacent right breast (arrow) that might erroneously be interpreted as a pathologic breast finding.
Inadequate or inappropriate positioning can create the appearance of lesions, that is, “false lesions.” For example, oblique rather than straight posterior positioning will create the appearance of increased uptake in the sacroiliac joint that is nearer the γ-camera. Unusual overlap of bony structures also can create false lesions. Equally troubling is inadequate positioning that obscures increased uptake at sites of true skeletal abnormality. General rules have been proposed for the positioning of patients undergoing bone scanning (11). In many instances, correct positioning requires that the clinical question be clearly understood and that patient positioning be chosen specifically to answer this question (12).
γ-Camera Setup for Delayed Bone Imaging
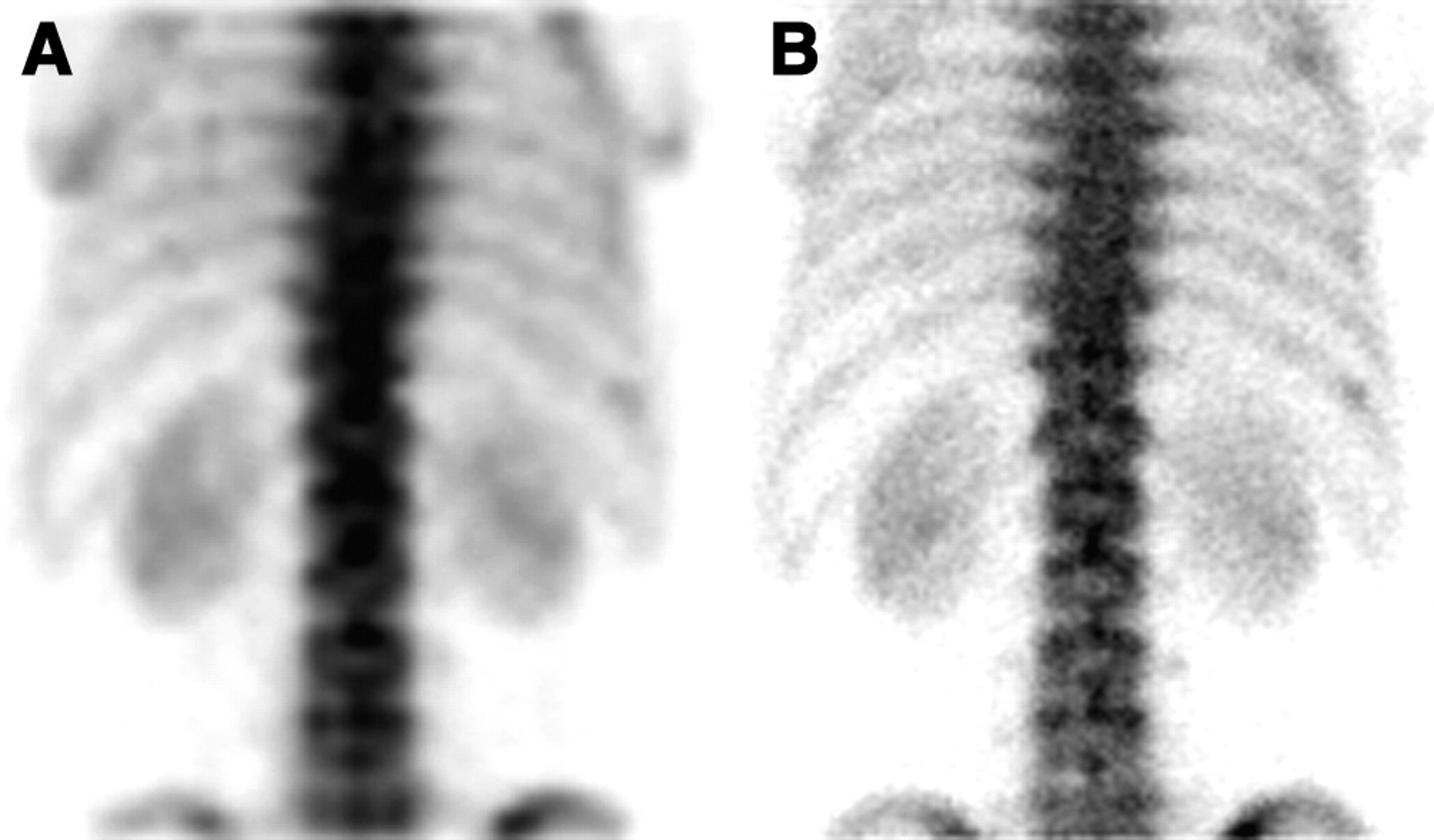
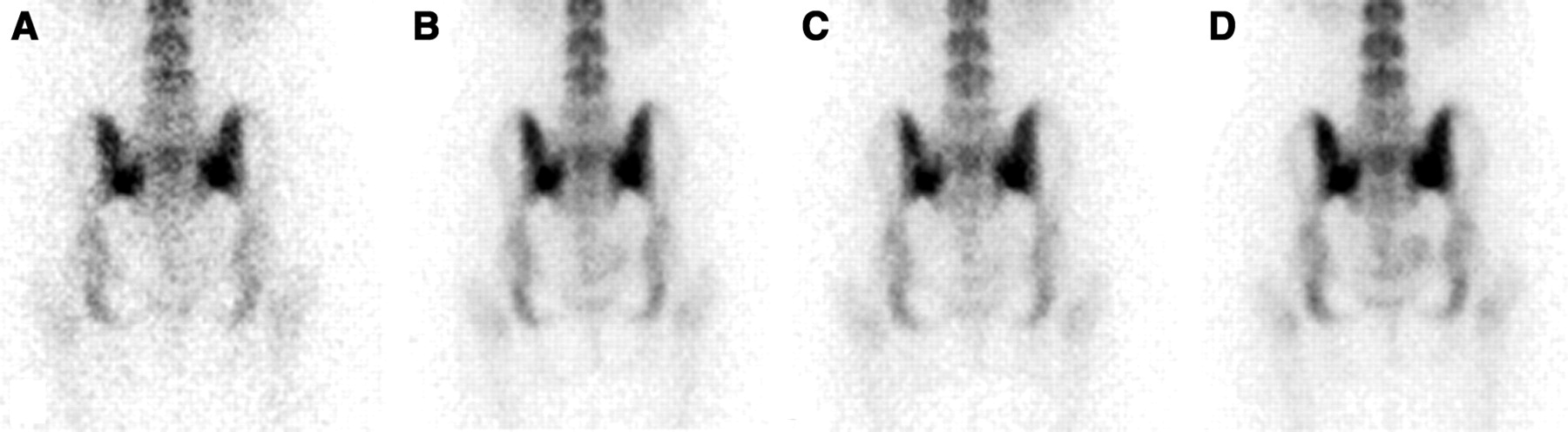
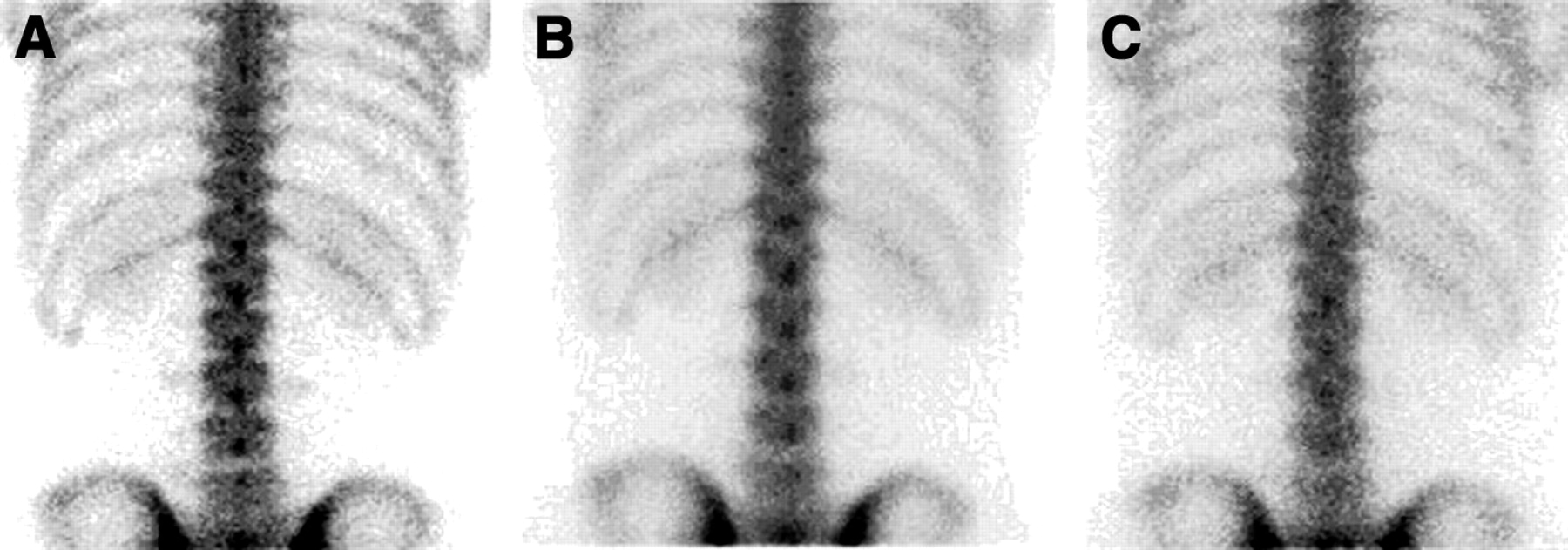
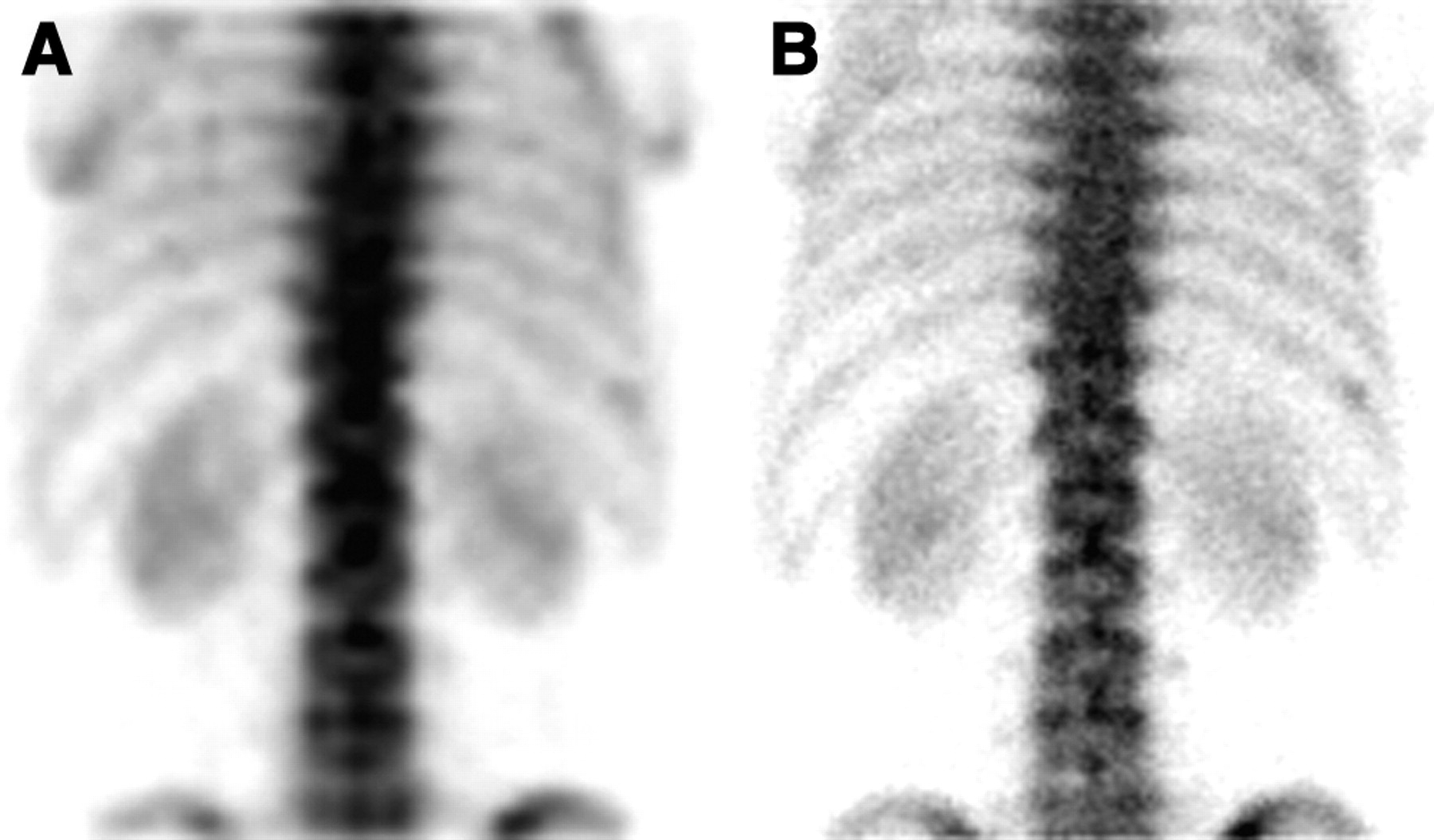
Errors in preparing the γ-camera for delayed planar imaging may have a dramatic impact on image quality. For example, inappropriate collimator choice will degrade image resolution. Figure 3 shows posterior planar lumbar-spine images obtained as ordered with a low-energy high-resolution collimator. The figure also shows simulated errors using a low-energy general-purpose collimator and a medium-energy collimator. Resolution is degraded when the general-purpose or medium-energy collimator is used. We agree with O’Connor et al. that for most planar and whole-body imaging, the high-resolution collimator appears to offer the best compromise between resolution and imaging time (3). However, even when the high-resolution collimator is used, resolution of the spine will be degraded when the collimator is not as close to the patient as possible (6). Figure 4 shows the same patient imaged with a high-resolution collimator just touching the back or either 10, 20, or 30 cm behind the back. The anatomic detail of the lumbar spine progressively degrades as the distance between the patient and the collimator increases. Patients sometimes become concerned when the collimator is brought close to their back for a posterior view of the lumbar spine. However, leaving a space of even 10 cm between the patient and the face of the collimator will significantly degrade image quality. The goal is to keep the patient-to-collimator distance as close as is reasonably achievable (6). Furthermore, physicians supervising a planar bone scan usually will not identify this technical error from a review of the images.
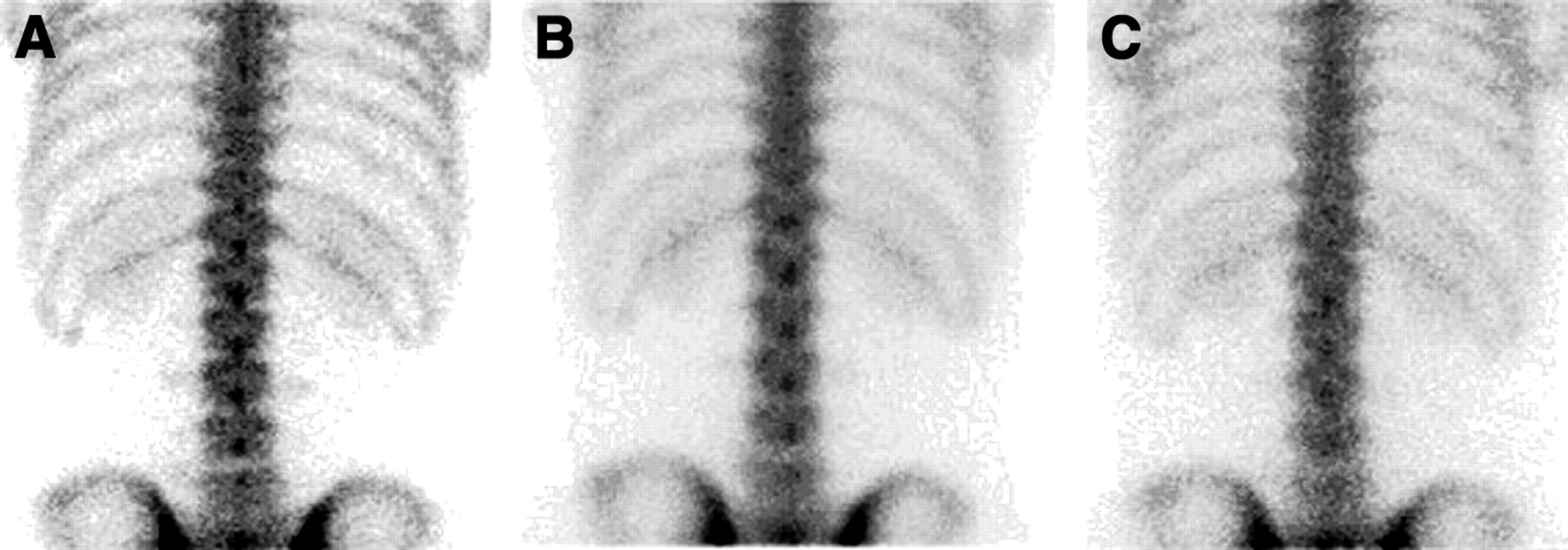
Effect of collimation on the resolution of planar bone scans: low-energy high-resolution collimator (A), low-energy general-purpose collimator (B), and medium-energy collimator (C).
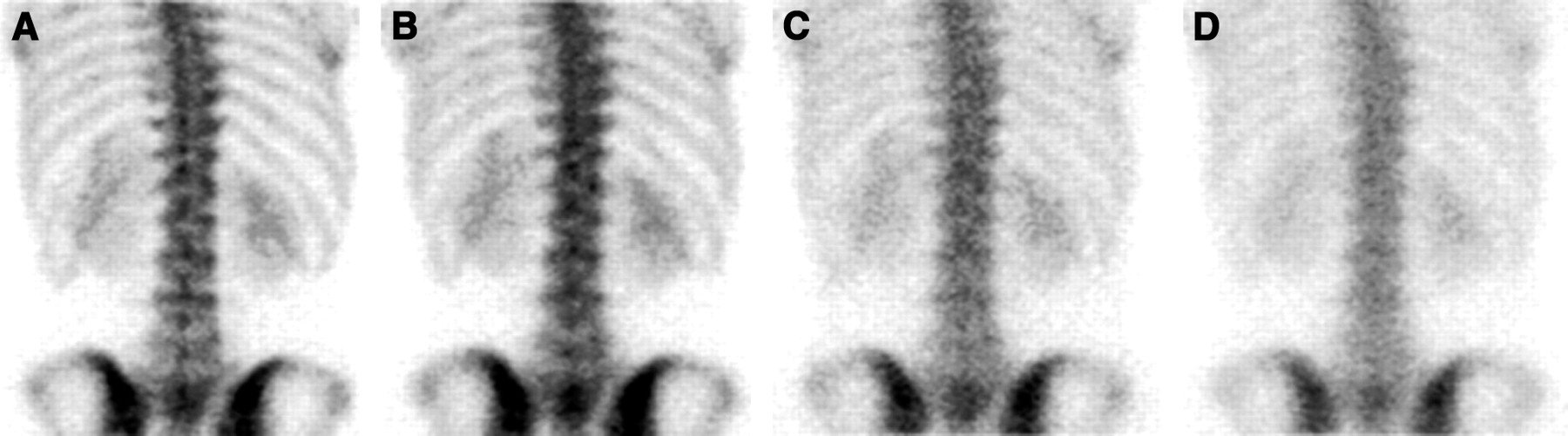
Effect of distance from the patient on the resolution of planar bone scans: just touching the back (A), 10 cm behind the back (B), 20 cm behind the back (C), and 30 cm behind the back (D). The anatomic detail of the lumbar spine progressively degrades as the distance between the patient and the collimator increases.
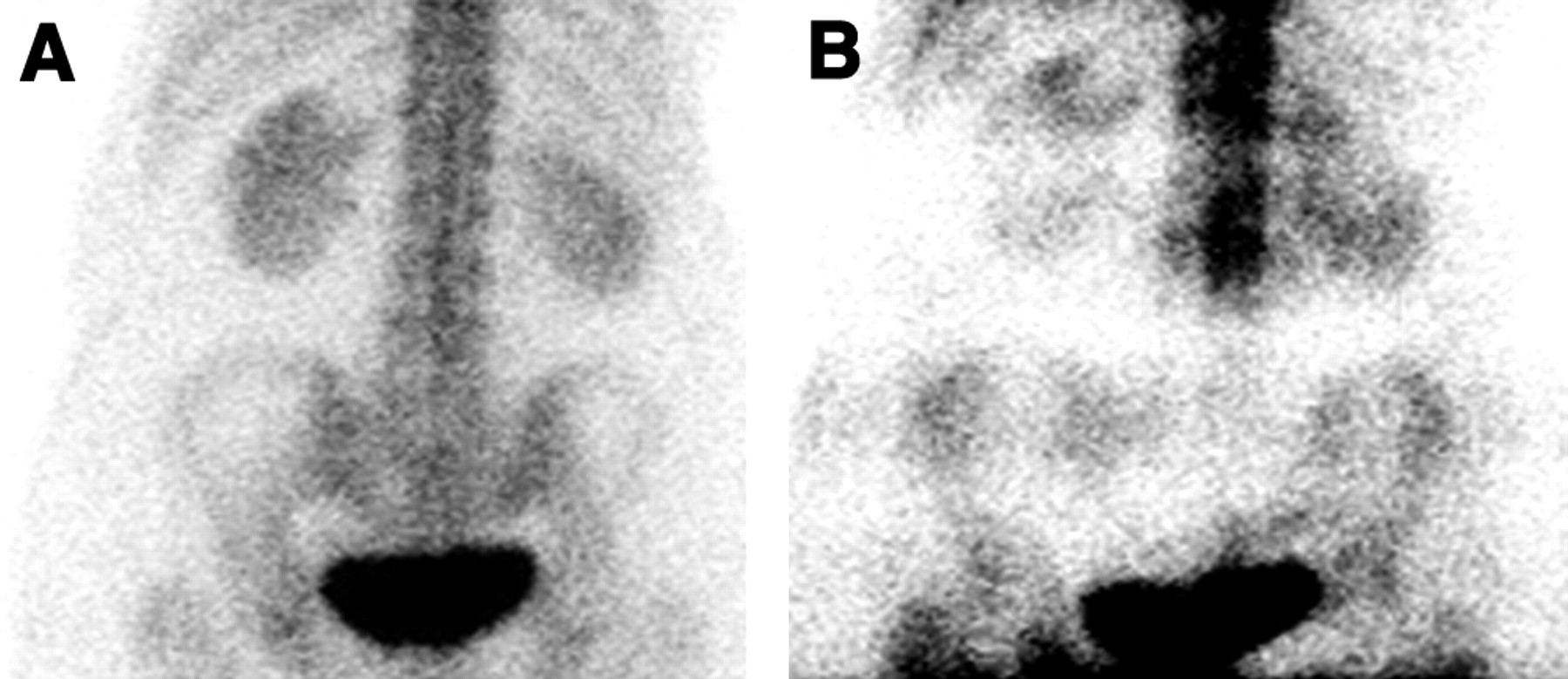
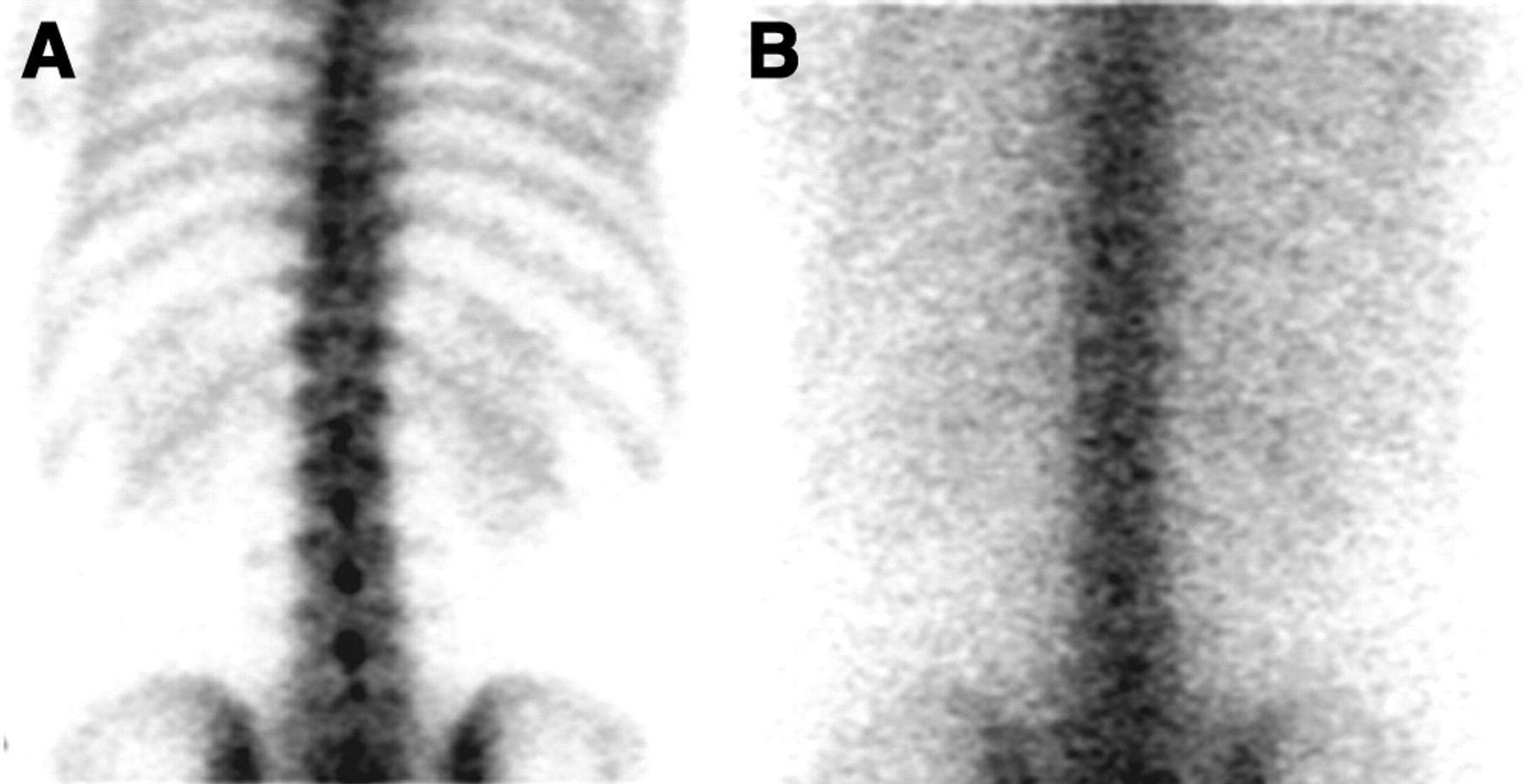
With use of a modern digital γ-camera, it is rare for a study to be selected using the wrong energy peak. Previously, this error was occasionally encountered when the daily quality control flood field uniformity obtained at the 122-keV photopeak of 57Co was followed by 99mTc-diphosphonate bone imaging. If the technologist did not adjust the γ-camera for a 20% energy window centered on the 140-keV photopeak of 99mTc, then an off-peak image with excessive soft-tissue scatter and some reduction in 99mTc photopeak counts was obtained (Fig. 5). Furthermore, some older γ-cameras show substantial nonuniformities when such off-peak images are acquired. Soft-tissue scatter degrades image quality by reducing contrast (13).
Effect of using a 57Co photopeak on planar bone scans: a 20% 140-keV photopeak (A) and a 20% 122-keV photopeak (B). Using a 57Co photopeak of 122 keV both increases soft-tissue scatter in the image and causes a loss of 99mTc photons. Image quality is dramatically reduced.
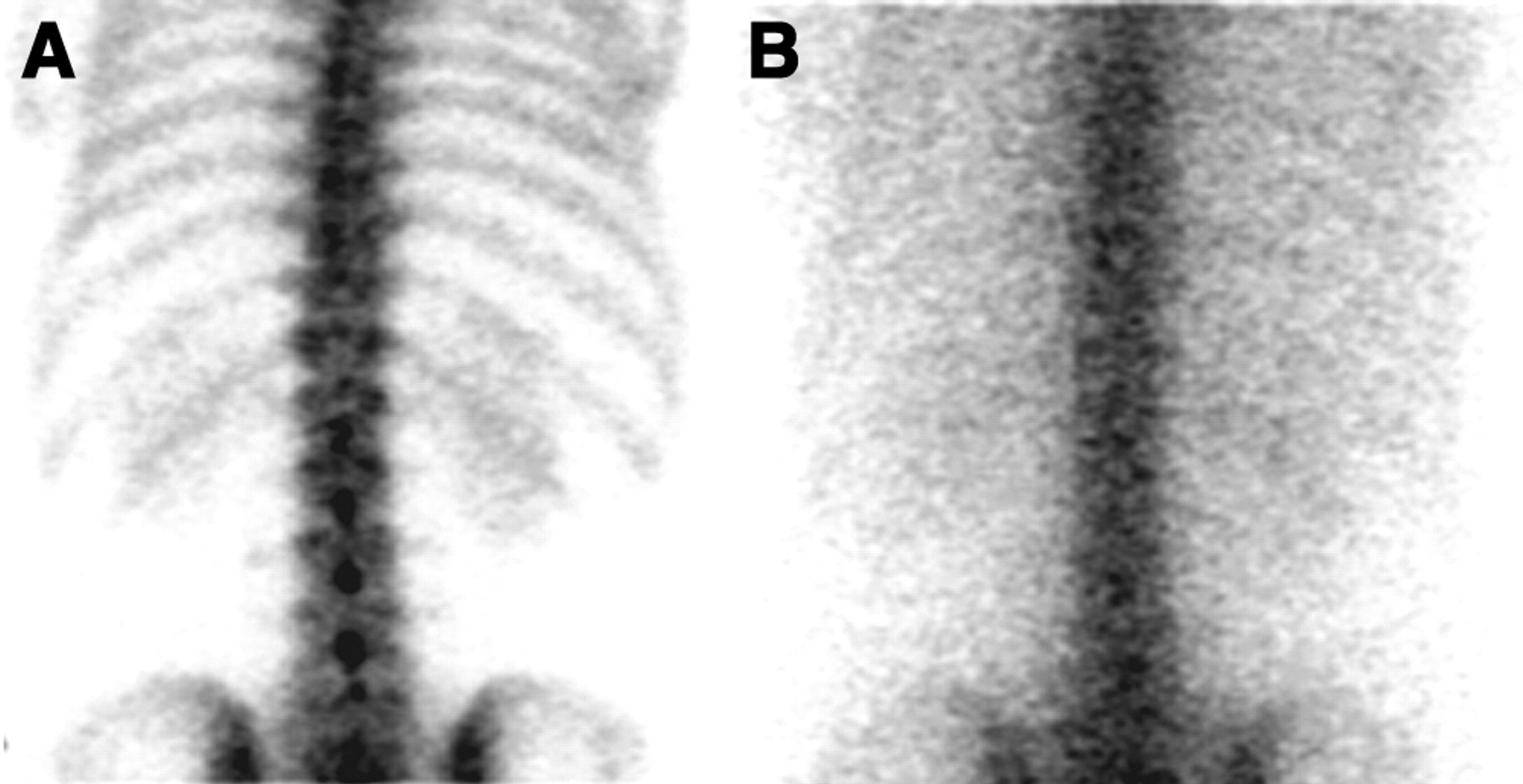
With a digital γ-camera, inappropriate choice of matrix size also will degrade image quality. The matrix size is usually 256 × 256 for spot images and 1,024 × 256 or 2,048 × 512 for whole-body images. To obtain the best resolution for a specified system and collimator, the matrix size should be chosen so that the pixel size is one third to one half the system resolution determined by the full width at half maximum. Too small a pixel size causes noisy images, whereas too large a size causes loss of resolution (7). For example, planar bone scans obtained with a 64 × 64 matrix are clearly inferior to scans obtained with a 256 × 256 matrix (Fig. 6). Furthermore, most integrated γ-camera systems have a large storage capacity, which eliminates the need to use byte-mode acquisition for static images.
Effect of matrix size on planar bone scans. Posterior views of the lumbar spine obtained using a 64 × 64 (A) and a 256 × 256 (B) matrix demonstrate a loss of anatomic detail for the former.
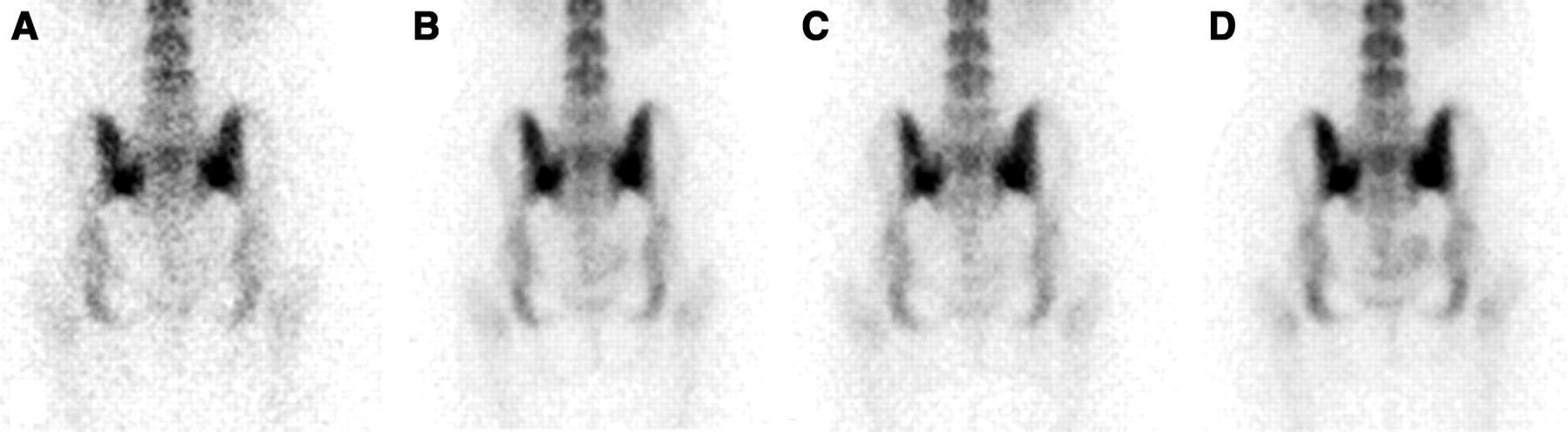
For an adequate spot image of the lumbar spine, 500–1,000 kcts is a reasonable range. However, we believe that when using a high-resolution collimator and a modern large-field-of-view γ-camera, a 500-kct study produces for most patients an acceptable planar image of the lumbar spine in a reasonable time. Figure 7 shows how lower-count studies result in inferior images, often referred to as count limited.
Effect of count density on planar bone scans. Posterior views of the pelvis were acquired for 100,000 counts (A), 250,000 counts (B), 350,000 counts (C), and 500,000 counts (D). With increasing count density, image quality improves.
Imaging the Patient
For delayed planar bone scanning, the patient should be made comfortable and should be instructed not to move or talk. A pillow behind the knees often will make a patient with low-back pain more comfortable on the imaging table. Furthermore, the judicious use of arm boards, straps, tape, and sand bags may help a patient to remain motionless in the desired position. Bilaterally symmetric positioning often is important, and at times taping the patient’s feet together is the best way to obtain pelvis views with the legs held motionless in neutral position. However, despite the best of efforts, some patients move during the acquisition of planar nuclear medicine images. Often this produces a blurred image somewhat like a photographic double exposure (Fig. 8). In most instances, any patient motion during image acquisition is easily recognized.
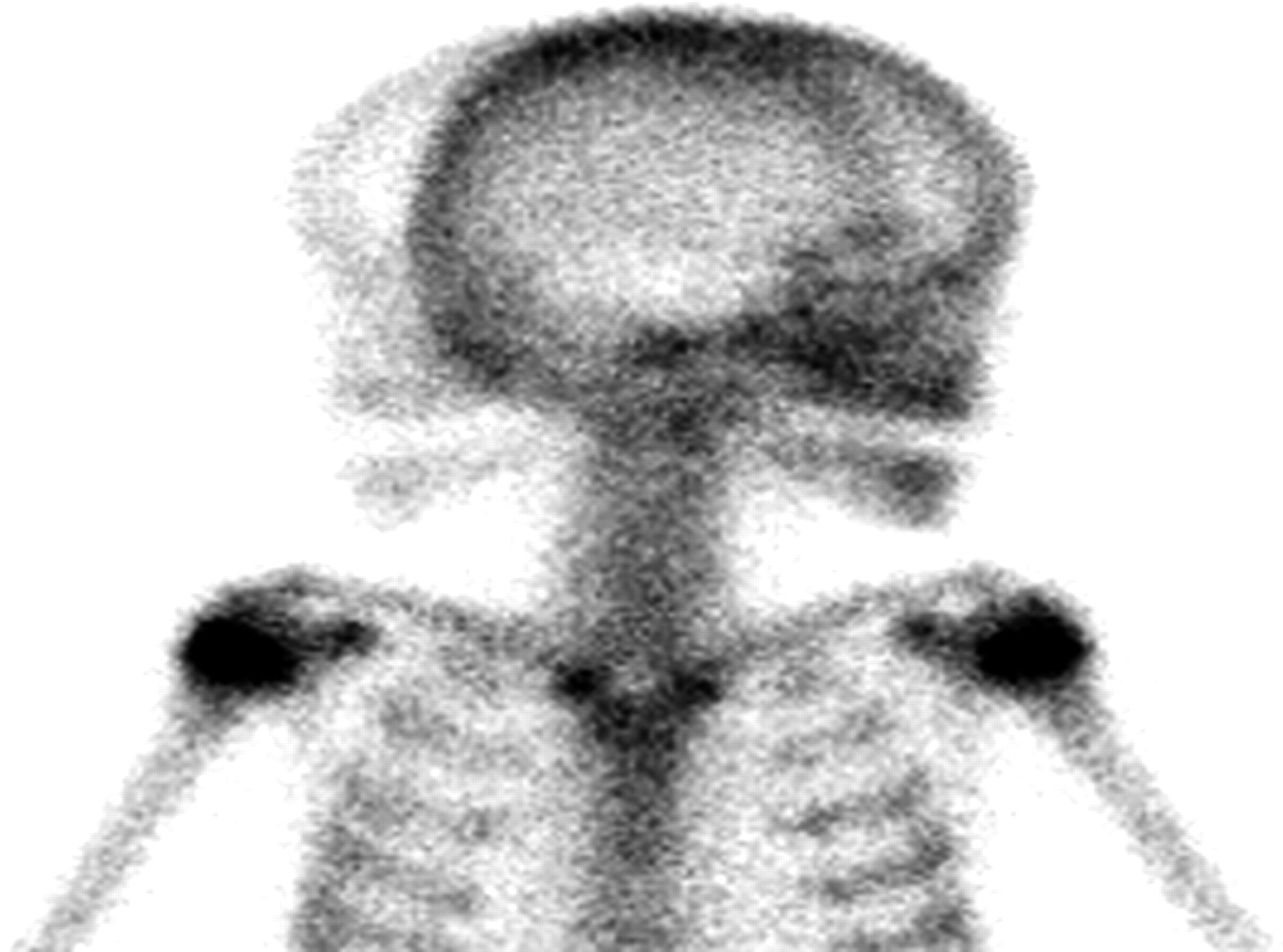
Movement of the patient’s head during planar bone scanning.
The patient undergoing bone scanning should be well hydrated. Between the time of radiopharmaceutical injection and 3-h delayed imaging, the patients should drink at least two 237-mL (8 oz) glasses of water, which will lead to bladder emptying and reduced radiation exposure (2). Furthermore, the patient should drink plenty of fluids during the 24 h after bone scanning. Patients are asked to void just before planar bone scanning begins. Thus, before imaging, patients void radioactive urine. If skin or garments are contaminated with this radioactive urine, then an artifact, which may be confused with a skeletal finding, is introduced (6).
CONCLUSION
In most busy nuclear medicine departments, planar bone scanning is performed daily without any technical difficulties. In fact, planar bone scanning is commonly considered to be one of the most reliable and easily performed nuclear medicine examinations. Nonetheless, one would be well advised to minimize the most commonly encountered imaging artifacts, such as patient motion and skin contamination with radioactive urine. Other potential pitfalls in planar bone scanning, such as excessive distance between the patient and the collimator, produce images of degraded resolution or quality. Furthermore, rarely encountered problems, such as Compton scatter from activity at a partially infiltrated intravenous injection site, may be a source of confusion and diagnostic misadventures. This brief article has by no means considered all potential mishaps that can occur during a bone scan. There are many other technical mistakes that practitioners encounters no more than once during their career in nuclear medicine. Without reading the legend, can you guess the nature of the extremely rare technical problem illustrated in Figure 9?
Footnotes
For correspondence or reprints contact: Sleiman Naddaf, MD, Department of Nuclear Medicine, Faculty of Medicine, Kuwait University, P.O. Box 24923 Safat 13110, Kuwait
E-mail: snaddaf{at}hsc.kuniv.edu.kw
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH SEPTEMBER 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}