


Abstract
The uptake of 99mTc-methylene diphosphonate (MDP) in malignant pleural effusions and, rarely, in nonmalignant pleural effusions has been well documented in the literature. Although the exact mechanism of uptake in these conditions remains unclear, there have been attempts to use the bone scintigraphic features of pleural effusion to predict sensitivity and specificity for malignancy based on pleural fluid cytology. It has been suggested that activity in the chest increases with an increase in effusion volume. We report here, however, a case of malignant pleural effusion, that showed reduced hemithoracic activity in contrast to the expected increased activity. Our experience highlights the need for an open and inquisitive mind to avoid diagnostic pitfalls when confronted with a bone scintigram showing reduced uptake unilaterally or bilaterally in the chest.
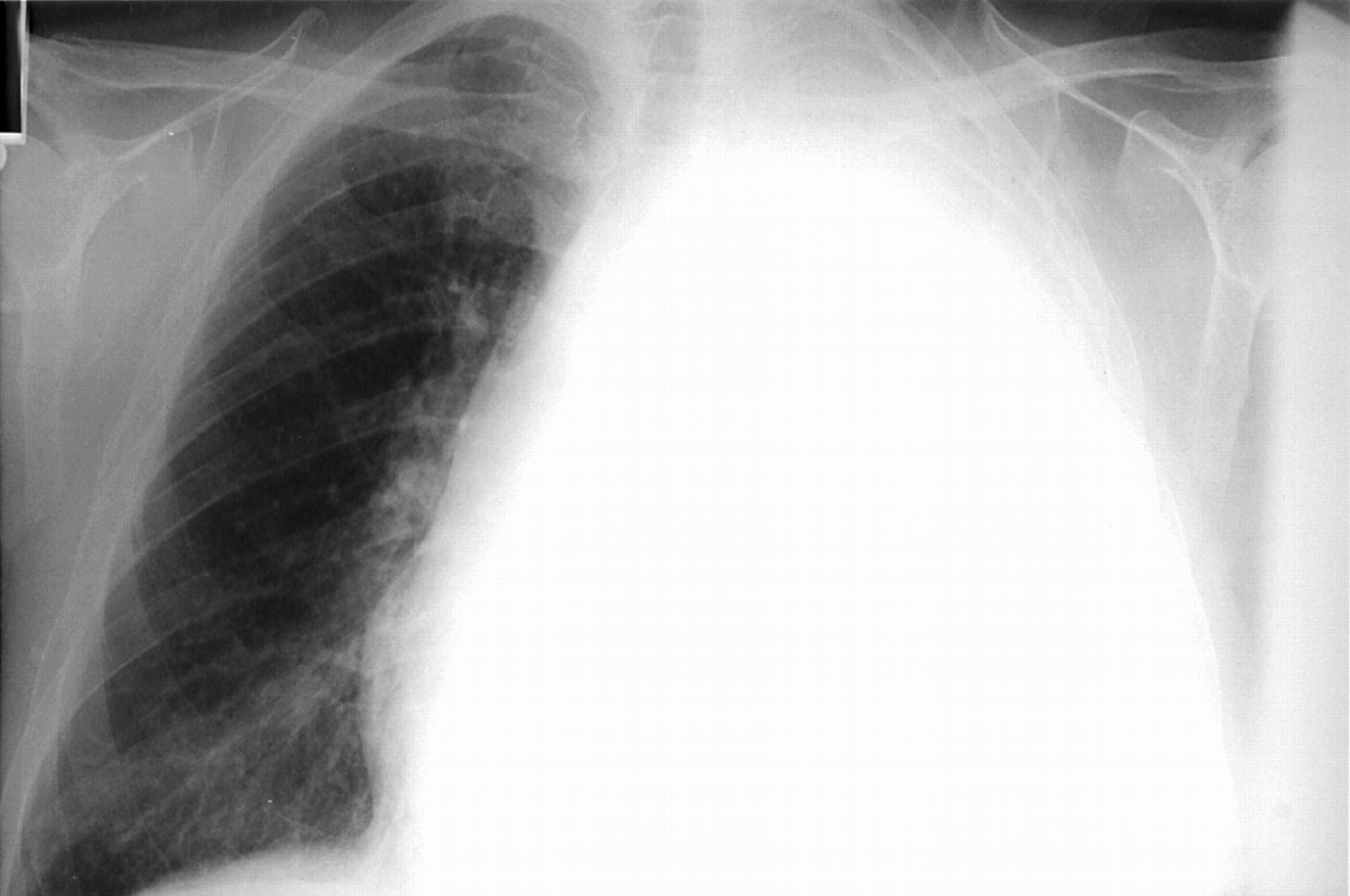
A 73-y-old man was referred to the nuclear medicine department for a bone scintigram with the provisional clinical diagnosis of skeletal metastasis. He had undergone a pneumonectomy for a cavitating adenocarcinoma (8 cm) in the left lower lobe 6 mo before, when several pleural deposits were also noted. The patient had no history of radiotherapy to the chest and refused chemotherapy. A chest radiograph on this occasion demonstrated a massive left pleural effusion (Fig. 1), which on aspiration was confirmed to be an exudate but negative for cytology.
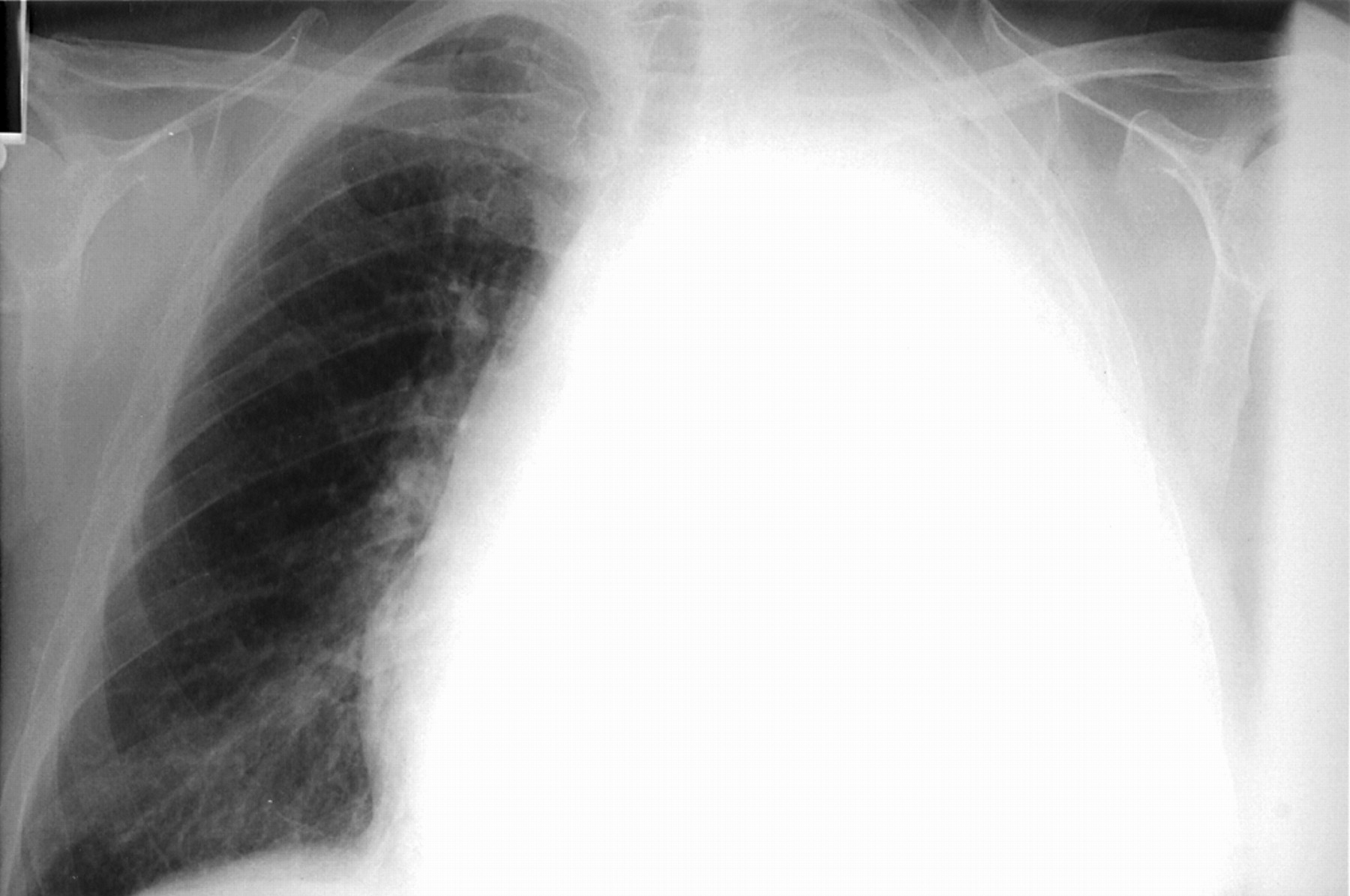
Chest radiograph showing massive left pleural effusion.
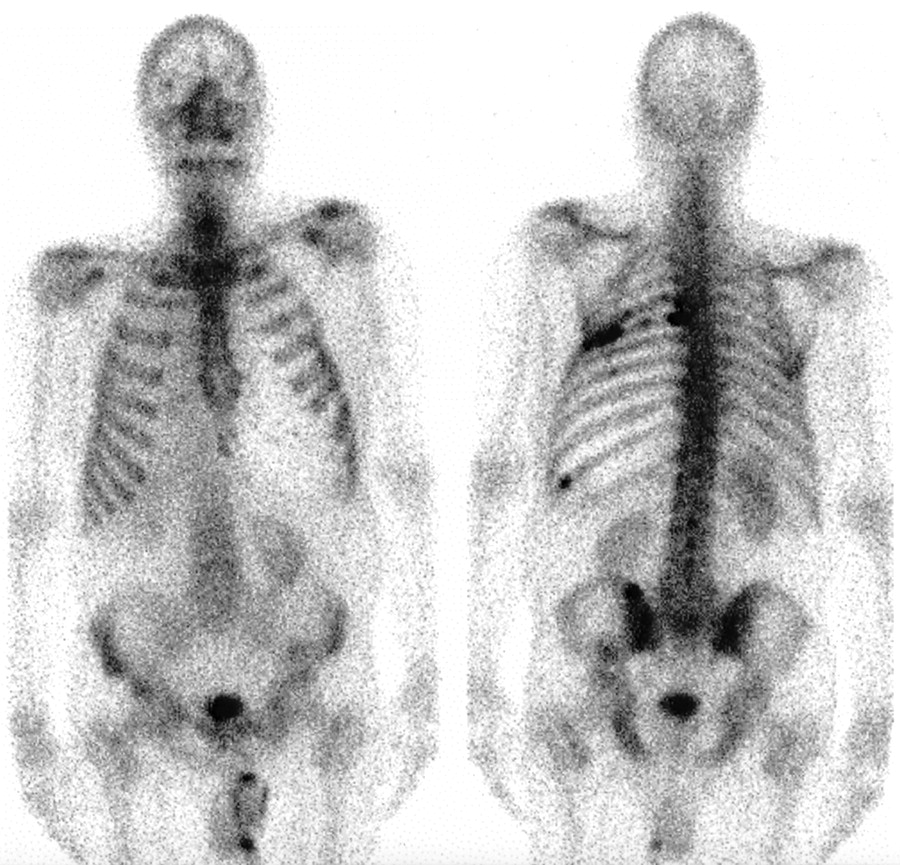
A bone scintigram was performed 4 h after the intravenous injection of 555 MBq (15 mCi) 99mTc-methylene diphosphonate (MDP) using a large-field-of-view gamma camera equipped with a general-purpose collimator. The resulting images demonstrated generally reduced accumulation of 99mTc-MDP in the left hemithorax (Fig. 2). In addition, focally increased uptake was noted in some ribs, consistent with previous thoracotomy with or without metastases.
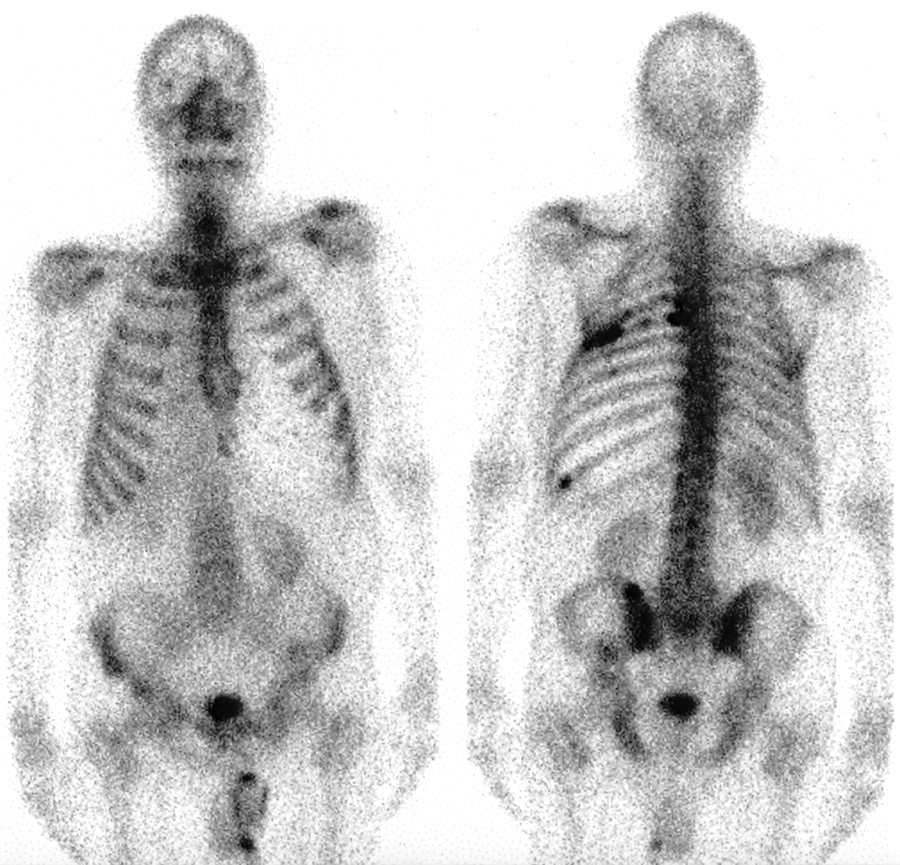
Anterior (left) and posterior (right) 99mTc-MDP bone images. Relative photopenia is visible in left hemithorax, and focal increased uptake is visible in ribs.
DISCUSSION
Increased thoracic uptake of bone imaging agents is well known to occur in a variety of situations, including pleural effusion. Although rare reports have been published on benign pleural effusions accumulating bone tracer, the current literature is dominated by studies demonstrating increased activity in malignant pleural effusions (1–4). The exact mechanism for the uptake is unknown but several factors are believed to be responsible. Altered capillary permeability in the pleura resulting from tumor invasion probably plays an important role (5), but metabolic effects (pH, etc.) induced by tumor cells may increase the amount of calcium and phosphorus in the effusion. Passive diffusion of 99mTc-MDP may be responsible for the uptake in benign effusion (3,5). In our patient, pleural deposits were observed during surgery, and this probably was responsible for causing the large effusion. The negative cytology of the pleural fluid, however, did not rule out a malignant cause, especially in the overwhelming clinical circumstances suggesting tumor involvement and in view of the known low yield from aspiration cytology.
To our knowledge, with the possible exception of one case report (6), there is a paucity of data in the literature showing reduced uptake of bone-imaging agents in pleural effusion. The previous study (6) showed reduced 99mTc-hexamethylene diphosphonate uptake in the hemithorax associated with massive pleural effusion in a patient known to have breast cancer. There was, however, doubt about the validity of the finding, as the patient had undergone a previous mastectomy on the same side, which also could cause chest wall photopenia. In the case of our patient, there were no mitigating circumstances for the reduced uptake other than the large effusion, which was confirmed by the radiograph and followed by aspiration.
The possible explanation for the reduced 99mTc-MDP uptake in this patient’s left chest is photon attenuation caused by the large pleural effusion, a situation analogous to a photon-deficient bladder during renography in patients with urinary retention who are unable to void before scanning. There is, however, no clear explanation as to why some patients with malignant effusion show increased uptake in the thorax compared with others demonstrating a relative photopenia. The clue may lie in the size of the effusion (i.e., the larger the collection, the higher the photon attenuation). Furthermore, there may be impaired diffusion of the bone tracer into the pleural cavity, which is filled with fluid under tension.
CONCLUSION
Malignant pleural effusions, contrary to common belief, may show reduced uptake on bone scintigraphy. The condition is often seen but rarely described. A photopenic hemithorax is probably the result of a large effusion, but further research is required to elucidate the mechanisms of in vitro as well as in vivo uptake with special reference to the type of cells, their number, rate of proliferation, and the pH of effusion.
Footnotes
For correspondence or reprints contact: Kottekkattu K. Balan, MD, Department of Nuclear Medicine, Box 170, Addenbrooke’s Hospital, Cambridge 2QQ, U.K.
E-mail: kottekkattu.balan{at}addenbrookes.nhs.uk





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.