


Abstract
Objective:We present 3 cases of suspected radioisotope urinary contamination that occurred on a single day. Because net clearance is via the kidneys, the injected dose is excreted in patients’ urine. It is important to recognize the patterns of urinary contamination to avoid reporting false-positive abnormalities.
Materials and Methods:99mTc-Medronate was administered intravenously and whole-body bone scans and spot views were obtained 2–3 h later.
Results:Two cases of urinary contamination were confirmed, and the third case was false-positive with a urinary collection leg bag seen in an orthogonal view.
Conclusion:We believe that urinary contamination is probably the most common type of contamination. There are distinct urinary contamination patterns among male and female patients. It is unusual to find so many cases of contamination on a single day in our institution. Few statistics are widely available on the number or percentages of contamination for specific radiopharmaceuticals.
Radioisotope contamination is a daily occurrence in any nuclear medicine department. Patient contamination is easily identifiable with our sensitive cameras. Contaminated objects (floors, sinks, wheelchairs) around the department that are not routinely imaged are more difficult to identify. This is why daily wipe tests are mandatory. Contamination is an unwanted occurrence for the nuclear technologist, involving cleaning and interruptions in work flow.
On a single day, 3 of 10 (30%) bone scans performed were suspected of contamination. Two cases were proven to be contamination, and the third case was later shown to be a urinary collection leg bag. This exceptional day caused us to search the literature for reports of contamination. Several references were identified in standard textbooks (1–8).
A Medline search also identified references on radionuclide contamination involving 131I (9,10), radiopharmaceutical injections in the cardiology laboratory (11), and during ventilation/perfusion (V/Q) scans (12–13). One review article nicely categorized multiple artifacts, including urinary contamination (14). Urinary contamination on bone scans has been seen at menses with tampon use (15), with a femoral vein Hickman catheter overlying the pelvis (16), and on patient hospital gowns (14).
MATERIALS AND METHODS
All patients received approximately 925 MBq (25 mCi) 99mTc-medronate (technetium-99m MDP; Bracco Diagnostics Inc., Princeton, NJ) and delayed whole-body images and multiple spot images were obtained. In addition, patient 3 had blood flow and blood pool images of the feet and ankles immediately after the radiopharmaceutical administration.
FINDINGS
Case 1
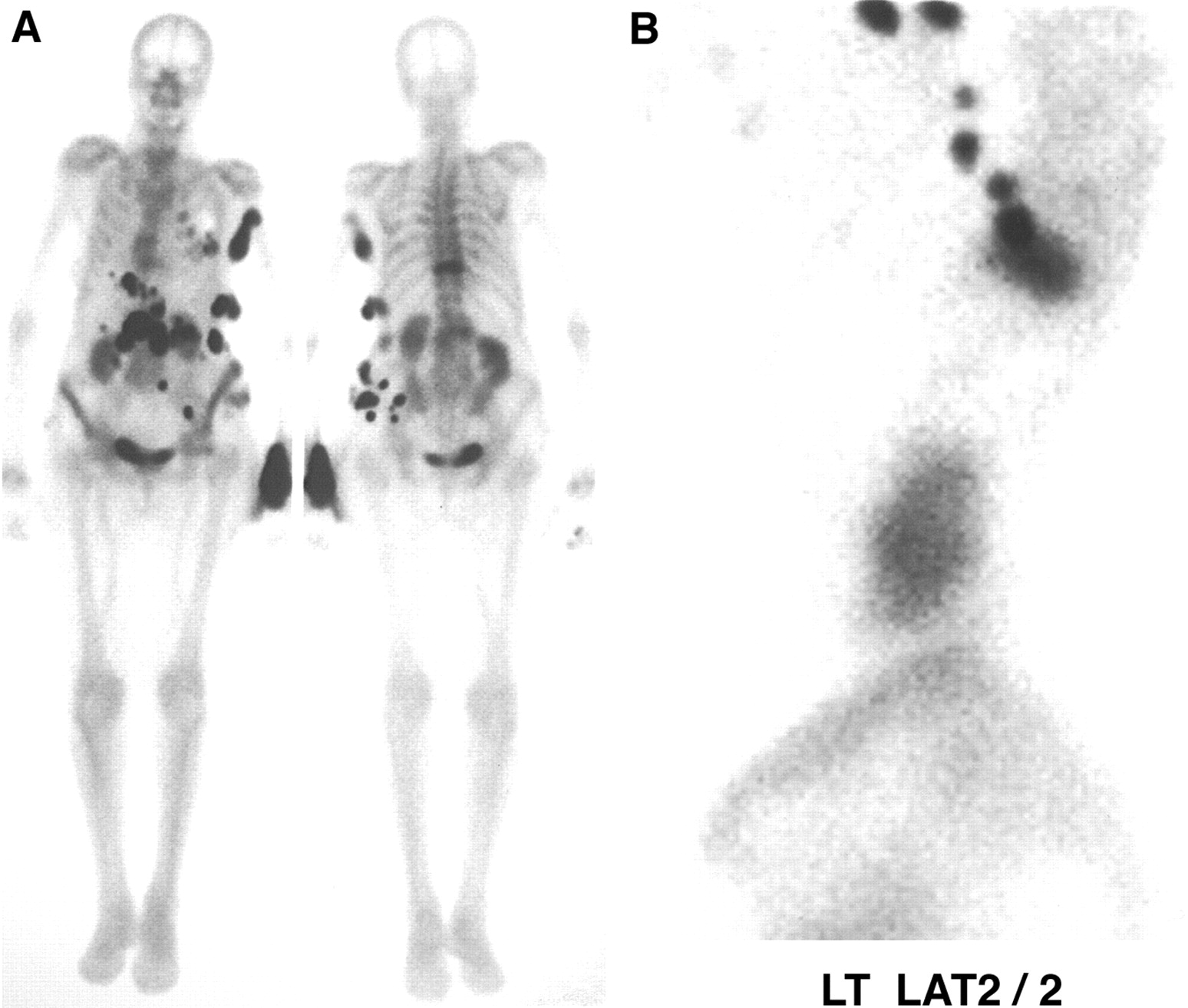
An 85-y-old woman with back pain from possible compression fractures was scheduled for a bone scan to confirm the cause of the pain. Delayed images demonstrated intense activity in the T11 vertebral body, consistent with a recent compression fracture and multiple left upper rib fractures. Abnormal, intense, glove-like activity was noted on the dorsum of the left hand. This proved to be a leaking injection site and the source of gown contamination over the left axilla, abdomen, pelvis, and chest. The contamination was easily demonstrated by pulling the gown up and reimaging (Fig. 1).
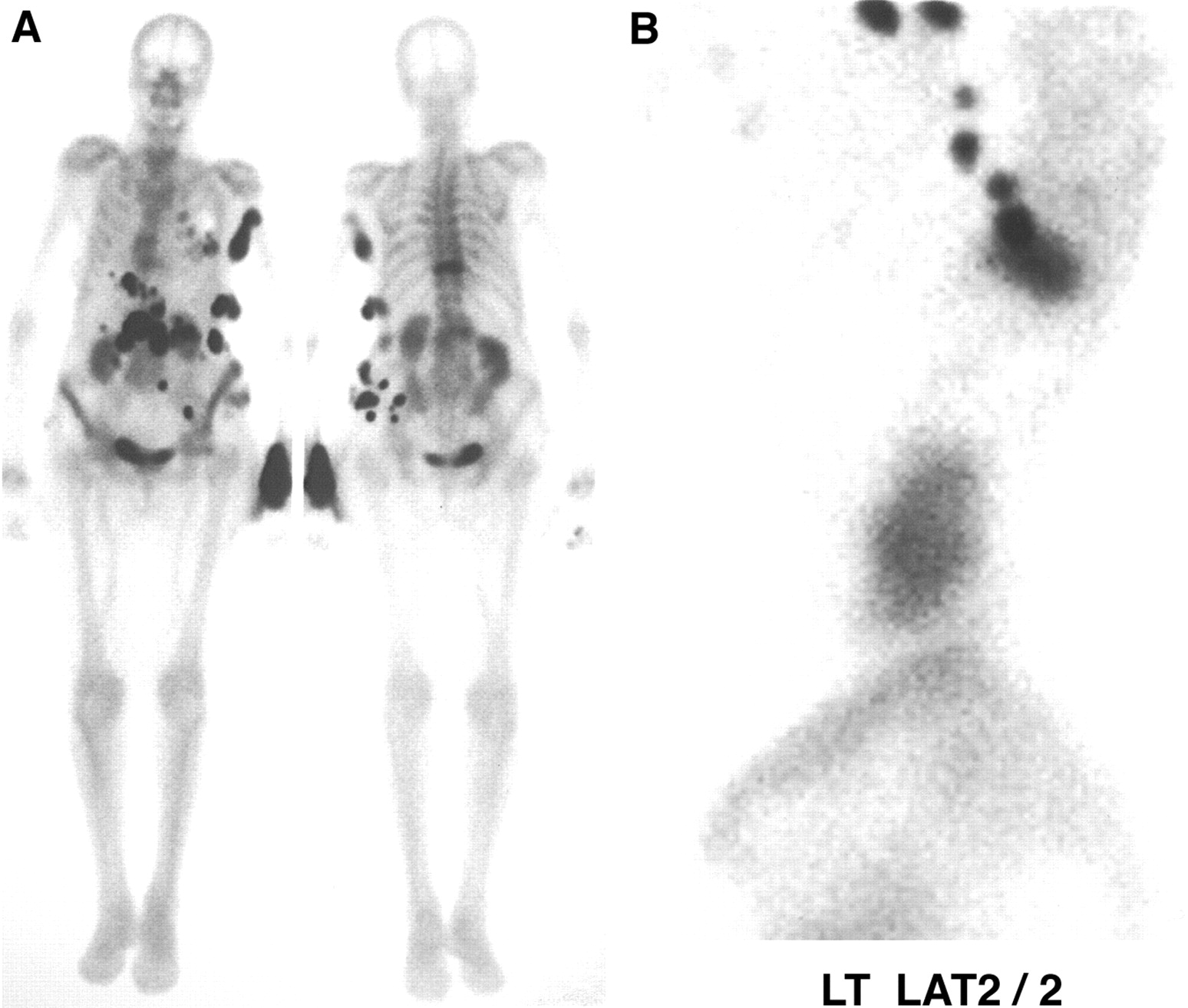
Case 1. (A) Contamination is evident at injection site, but rest of activity could have been mistaken for bone-forming metastases from osteosarcoma or simply leaking intravenous site. (B) As gown was moved, activity also moved, confirming contamination.
Case 2
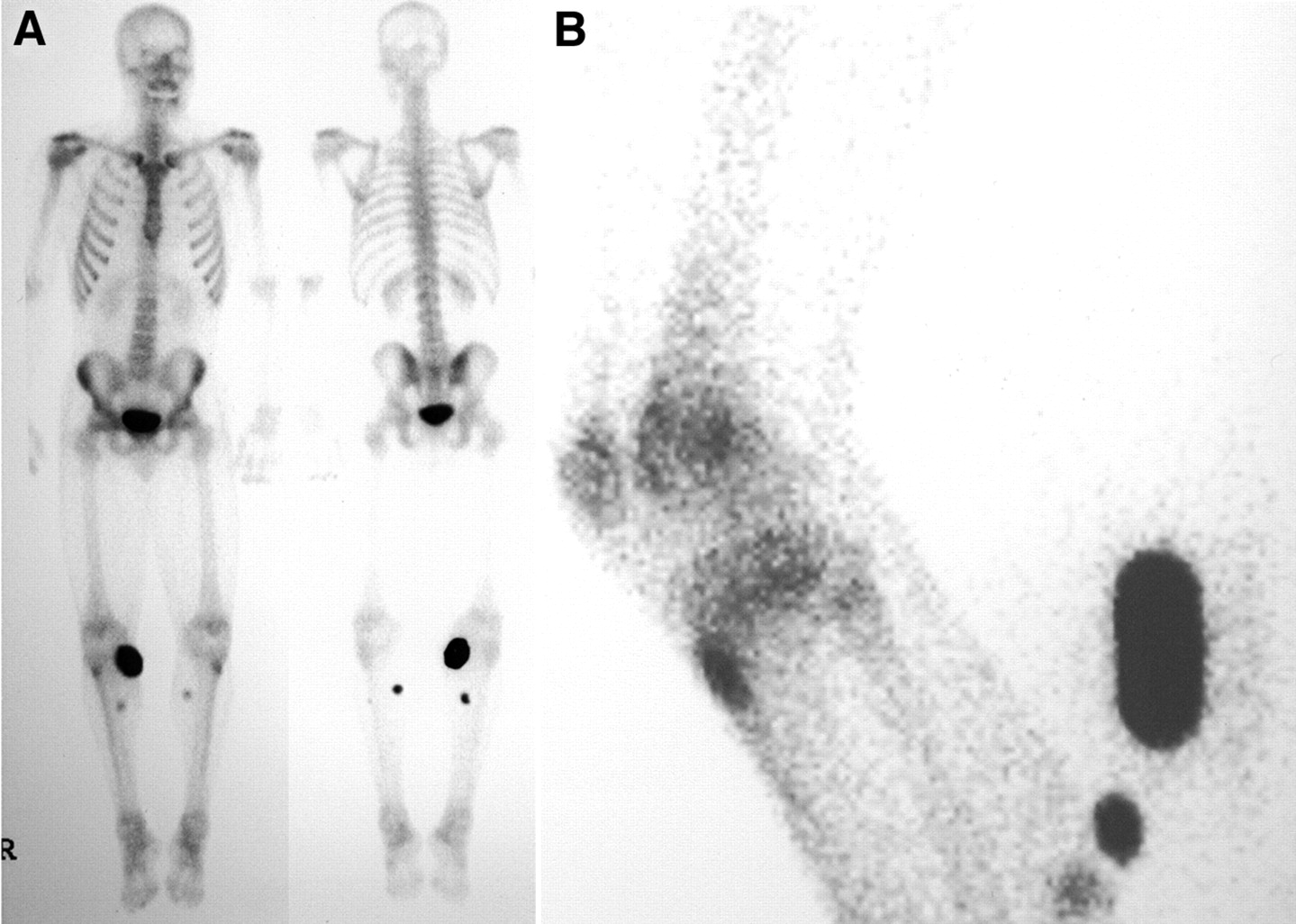
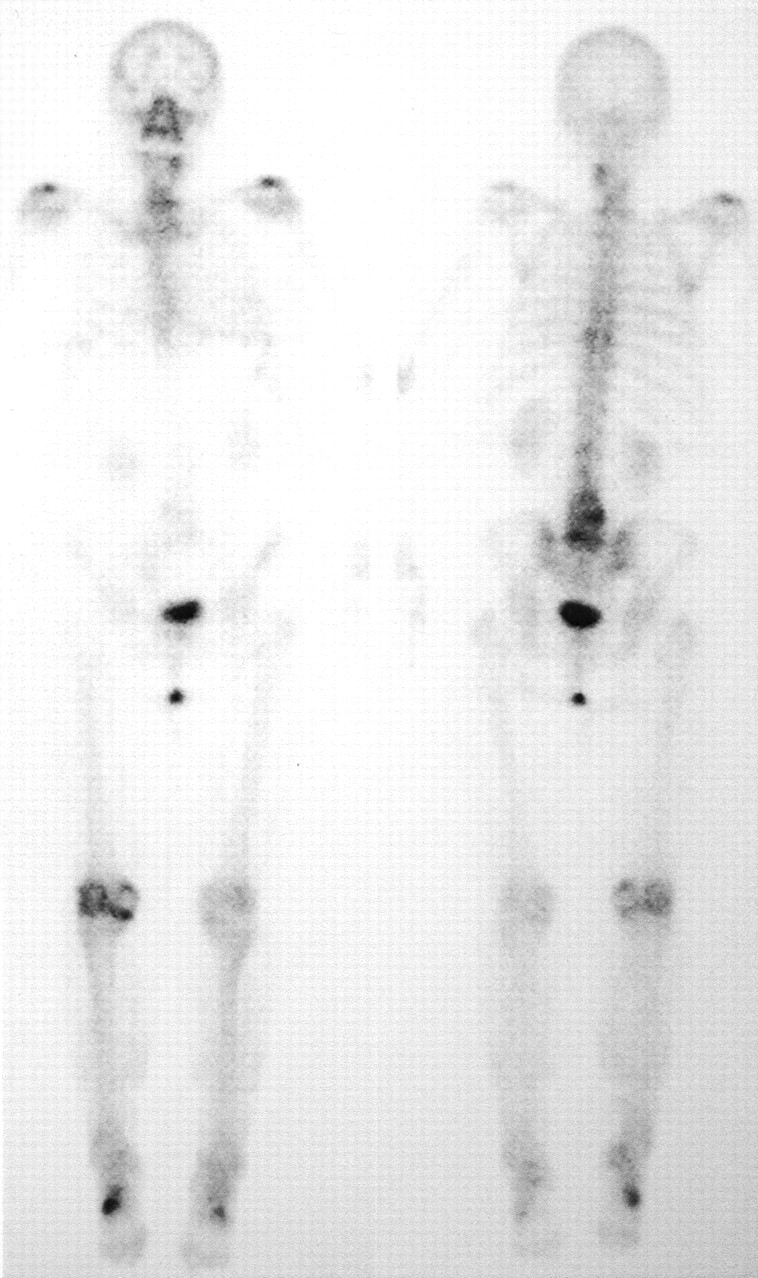
A 22-y-old man had a contusion on the right chest wall and lumbar spine secondary to a work-related fall from a truck. Mild abnormal increased activity was noted in the sternoclavicular joints and shoulders but not the ribs. Both kidneys and bladder were normal. Abnormal activity was noted over both legs, especially on the right leg inferior to the knee, as a result of urinary contamination on a protective sheet (Fig. 2).

Case 2. (A) Abnormalities seen only in anterior and posterior views could have been mistaken for sites of trauma. (B) Lateral view shows activity posteriorly on protective sheet.
Case 3
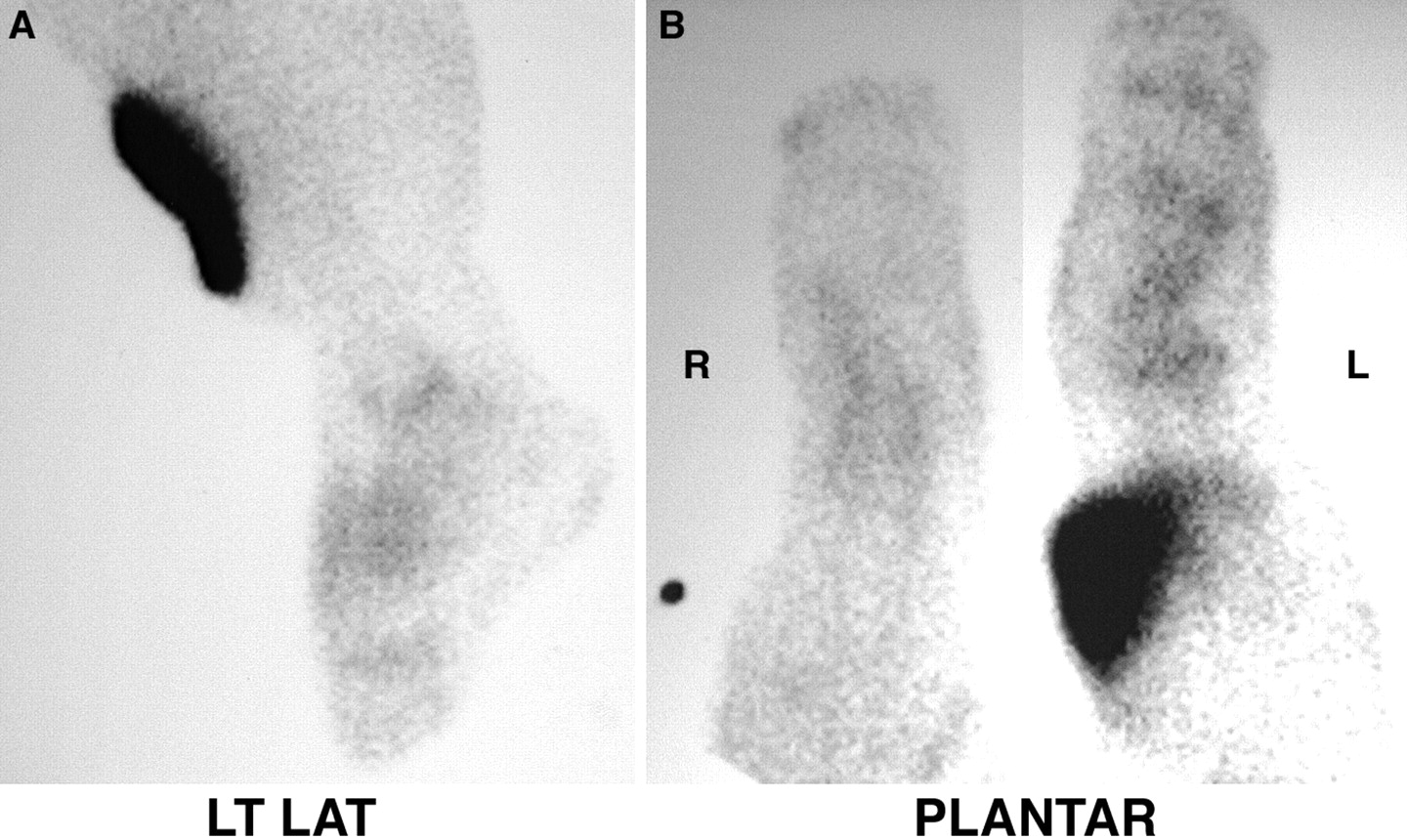
A 33-y-old man presented with persistent left foot cellulitis and was imaged to exclude acute osteomyelitis. The blood pool images showed faint focal activity in the left leg above the ankle. Although the delayed images did not show significant activity in the legs or feet, localized leg activity clearly represented a urine bag best seen on a left lateral view (Fig. 3).

Case 3. (A) Originally believed to be urinary contamination, leg bag is clearly seen on lateral view. (B) Posterior view of urinary bag.
RESULTS
A common source of contamination results from the intravenous injection of the radioisotope. Contamination may result from injection site dose infiltration, a leaking intravenous tube, or bleeding from the puncture site because of inadequate hemostasis.
Because all bone agents are excreted through the genitourinary (GU) tract, we obtain an incidental view of the entire GU system from the kidneys to the external genitalia. Some authors report up to 40% of GU abnormalities detected. Not every bone scan detects a GU abnormality. Others may show a urine leak or urinary diversion simulating a leak. Intense abdomen or pelvic activity may represent an unusual case of contamination, bladder rupture, tortuous or dilated ureters, or surgical urinary diversion.
Urinary contamination is a relatively common finding. Some patients are quite fastidious, others are not as careful, and still other patients have renal failure and produce very little urine. Some patients have urinary tract obstructions or Foley catheters.
Distinct male (Fig. 4) and female (Fig. 5) patterns of urinary contamination were noted. Among patients with minimal urinary contamination, females produce a short linear area, whereas males have a more random pattern that represents the more mobile external genitalia. In cases of gross contamination, no distinct male or female patterns of contamination were noted.

Male urinary contamination pattern.
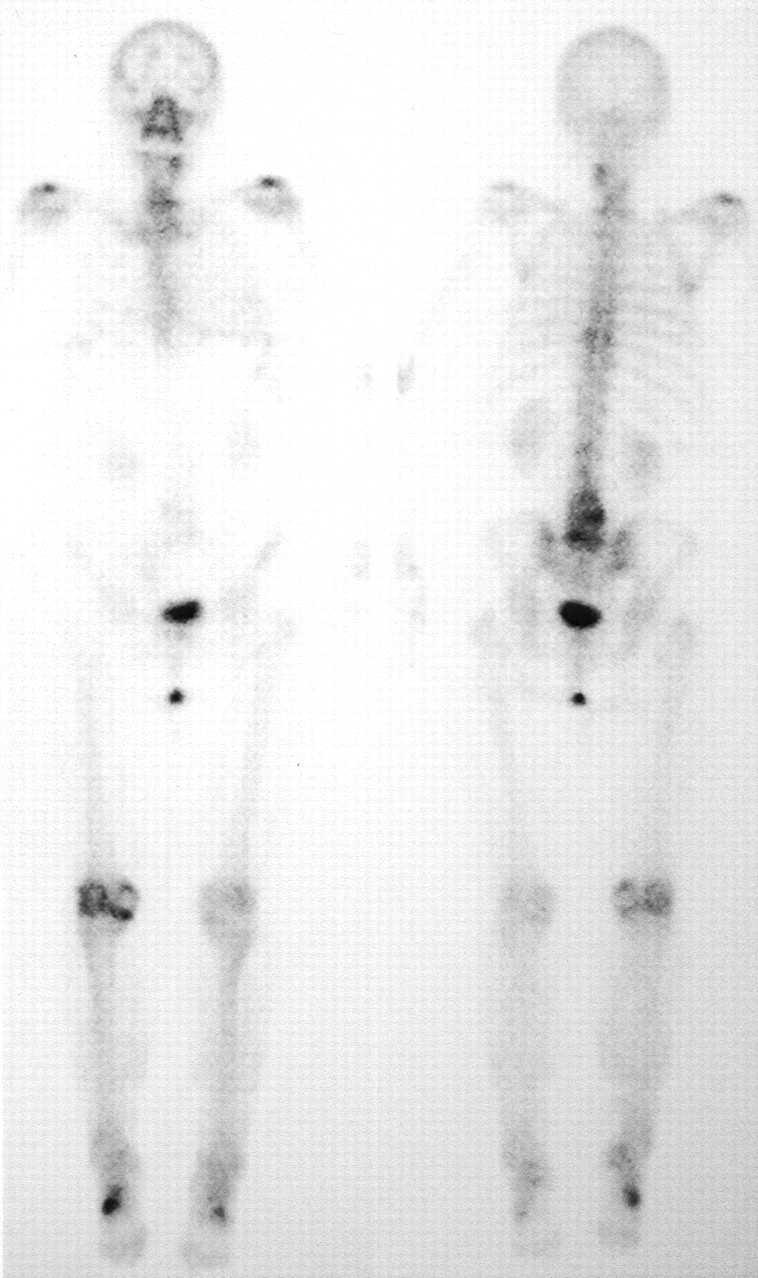
Female urinary contamination pattern.
DISCUSSION
Contamination is seen every day in our department. One author has classified the types of problems associated with radiopharmaceuticals, including contamination (17). We once believed that infiltrated doses were more common with each year’s new students, but we are beginning to rethink that hypothesis. An infiltrated dose can lead to axillary lymph node activity unrelated to possible neoplastic activity.
CONCLUSION
It is important to recognize contamination and differentiate it from a true abnormality. In one of our cases, a leg bag simulated soft-tissue activity that could have been interpreted as cellulitis. A small study looking at 2 different departments for incidental contamination for two 1-mo periods demonstrated our belief that the frequency of contamination varies with the radiopharmaceutical (18). A study dedicated to the topic of contamination would be helpful to establish the frequency of and site location for each radiopharmaceutical. Types and locations of contamination may be radiopharmaceutical dependent.
Footnotes
For correspondence or reprints contact: Michael E. Spieth, MD, Department of Radiology, Nuclear Medicine Section, Marshfield Clinic, 1000 North Oak Ave. H-IN-NM, Marshfield, WI 54449.
E-mail: spieth.michael{at}marshfieldclinic.org





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}