


Abstract
Objective:Since the approval of mercaptoacetyltriglycine (MAG3) for routine clinical use, reports have appeared about hepatobiliary excretion deleteriously affecting available diagnostic and quantitative information. The purpose of this study was to evaluate gallbladder (GB) uptake of MAG3 in the clinical setting and its effect on the evaluation of relative renal function and imaging.
Methods:Sixty patients with varying degrees of renal impairment were studied. Routine renal function imaging was followed with anterior and right lateral 3-min abdominal images. Factors such as photolytic degradation, reconstitution steps, 99mTc O4 solution, age, and concentration are discussed. In addition, patient fasting state and radiochemical purity are evaluated. The GB uptake was determined as a percentage of the injected dose.
Results:The MAG3 quality control ranged from 90.9% to 99.0%. The GB uptake ranged from 0.0% (not visualized) to 0.71%. The effective renal plasma flow ranged from 88 to 743 mL/min. There was no correlation between the QC and the percentage of GB uptake (r = 0.12). The majority of patients in the nonfasting state showed minimal or reduced GB uptake when compared with the majority of patients in the fasting state.
Conclusion:Our data suggest that GB uptake of MAG3 is minimal, with no adverse effects on the diagnostic and quantitative analysis of renal function.
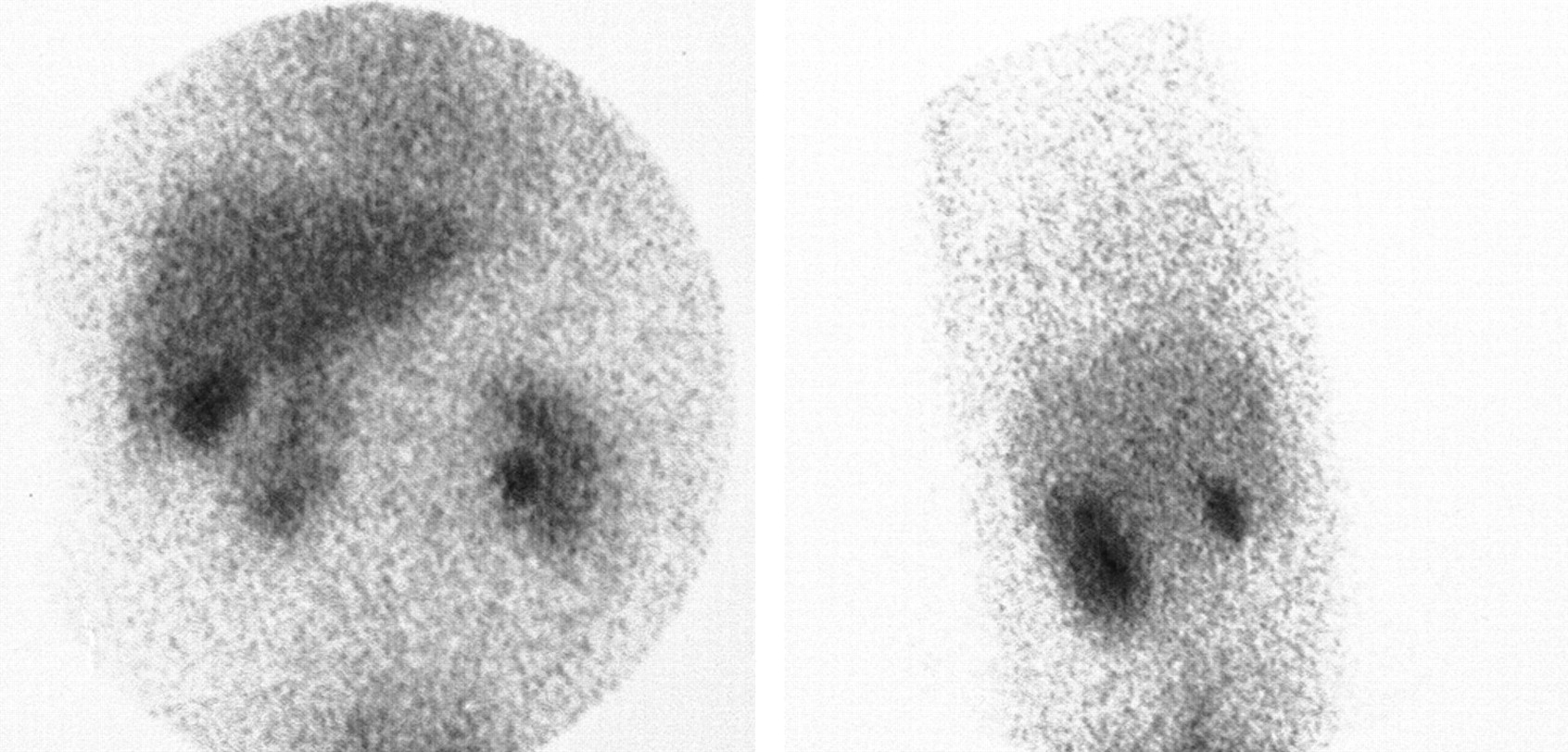
The elimination of nuclear medicine imaging agents from the body occurs primarily by 2 major routes of excretion: gastrointestinal (hepatobiliary) and renal (glomerular filtration and tubular secretion). In the early 1990s, 99mTc-mercaptoacetyltriglycine (MAG3), a renal tubular agent, was introduced to replace 131I-o-iodohippurate (OIH). Since the approval of MAG3 for routine clinical use, conflicting reports about the amount of hepatobililiary excretion have appeared in the literature. Marked excretion would affect the diagnostic and quantitative information available in the investigation of relative renal function and quantitative analysis. The findings of hepatobiliary excretion, as seen in Figures 1 and 2, have been reported (1), and the majority of such reports have been associated with the utilization of the commercial kit formulation.

Anterior and right lateral images taken after completion of routine renal function study. Images have been made darker to better show gallbladder.

Persistent activity in upper pole of right kidney, as if gallbladder is shining through. Urinary bladder activity has been digitally masked.
Because the plasma clearance of an agent reflects clearance by all elimination pathways, hepatocyte uptake and hepatobiliary excretion must be considered. If significant uptake occurs, the plasma concentration would be lower, making the renal uptake and hence the clearance calculation artificially lower. This, in turn, would underestimate the renal clearance, invalidating the accuracy of the results (2).
The purposes of this study were to evaluate the gallbladder (GB) uptake of 99mTc-MAG3 during renal imaging and to attempt to ascertain its significance in the clinical setting, particularly the effect it would have in the quantitative analysis of renal function as performed by the simple and now routinely used camera technique.
MATERIALS AND METHODS
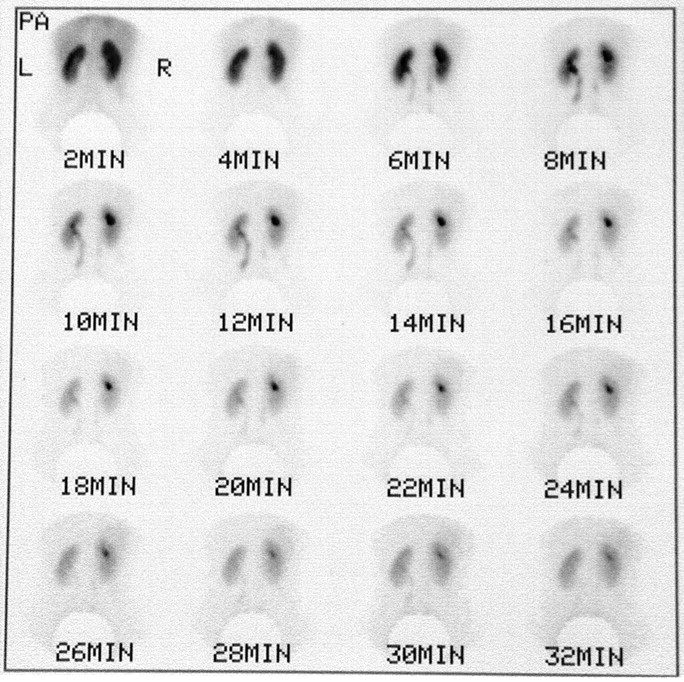
Sixty randomly selected patients with varying degrees of renal impairment were studied after a single injection of MAG3 (37 MBq per kidney). Our population consisted of 31 women and 29 men, with an age range of 25–76 y (mean, 48.9 y). Imaging was performed on seated patients, using a large-field-of-view camera (Elscint 409 M; Elscint, Hackensack, NJ) fitted with a low-energy, medium-sensitivity, medium-resolution, parallel-hole collimator. Data were acquired in a dynamic mode at 2 s per frame for 120 s, followed by 15 s per frame for 30 min, in a 128 × 128 matrix. The effective renal plasma flow (ERPF) was calculated by the camera technique. Routine renal function imaging was followed by an anterior and right lateral abdominal 3-min image in a 256 matrix. Patients with a transplanted kidney or known cholecystectomy were excluded from the protocol. The GB uptake was determined as a percentage of the injected dose, at 35 min after injection. The fasting state of the patient was noted. A fasting state was defined as a patient having nothing by mouth after midnight on the day before the test. A nonfasting state meant that patients followed their routine eating habits.
RESULTS
The MAG3 quality control (QC) ranged from 90.9% (2 studies) to 99.0% (mean, 96.52%; Sep-Pak method; Mallinckrodt Inc., St. Louis, MO). The percentage GB uptake ranged from 0.0% (nonvisualization) to as high as 0.71% (mean ± SD, 0.13% ± 0.15%) of the injected dose at 35 min. The global kidney uptake ranged from 3.9% to 14%. The global ERPF ranged from 88 to 743 mL/min. There was no correlation between the MAG3 QC and the percentage of GB uptake (r = 0.12). The majority of patients in the fasting state showed GB uptake but always <0.72% of the injected dose. The majority of patients in the nonfasting state displayed minimal or reduced GB uptake. The same patient in the fasting and nonfasting state (2 different hospital visits, 1 wk apart) is shown in Figure 3. Additional results are summarized in Table 1.

Anterior images of same patient 5 d apart. Right image shows nonfasting state.
Results from Analysis of Static Images Acquired After Completion of Renal Function Study
DISCUSSION
Nuclear medicine imaging and diagnosis has evolved toward increasing camera and computer sophistication with currently commercial camera-based techniques available for measuring glomerular filtration rate with 99mTc diethylenetriaminepentaacetic acid and ERPF with 99mTc-MAG3. Although camera-based clearances are not as accurate as those based on plasma samples, they are highly reproducible with stable-disease patients (3). This study addresses MAG3 elimination by the hepatobiliary system and its possible effects on calculations of relative renal function and quantitative analysis by the camera technique.
With hepatobiliary excretion of MAG3, the radiopharmaceutical would accumulate in the GB. Its concentration and radioactivity would increase over time. When acquiring a renal study in the posterior view, the GB activity would shine through, overlying the kidney and falling primarily in the field of view of the upper pole of the right kidney (as seen in Figs. 1 and 2). This could possibly result in a false diagnosis (e.g., obstructive uropathy pattern) in addition to an underestimation of renal clearance, which would invalidate the accuracy of the results obtained by the camera method.
Although 57% of our patients displayed some GB uptake, this was always <0.72% of the injected dose and at no time interfered with the renal clearance calculation or suggested a false diagnosis such as an obstructive uropathy curve pattern. Accumulation and retention of activity in the upper pole of the right kidney does not necessarily mean that it is the result of GB activity shining through. This phenomenon is not uncommon and could easily be the result of such factors as isolated obstructed calyces or merely retention of intrarenal activity. If the origin of the activity is in question, a right lateral image can be acquired at the end of the study. Retention of activity also can be seen in the upper pole of the left kidney (Fig. 4). This cannot be interpreted as coming from an extrarenal source.

Persistent activity in upper pole of left kidney, representing retention in calyx. Urinary bladder activity has been digitally masked.
Because the hepatobiliary elimination of 99mTc-MAG3 activity has been associated with the excretion of radiolabeled impurities, it is important to understand the following factors that could affect the labeling efficiencies of MAG3.
Solutions of sodium pertechnetate 99mTc that contain oxidizing agents (sodium hypochlorite or hydrogen peroxide) should not be used (4), because these reduce the labeling efficiency. Reconstitution with 10 mL saline optimizes the labeling efficiencies (QC averages of 96.7% versus 91.1% if reconstituted with 5 mL). Using <4 mL is contraindicated, because this usually produces a labeling efficiency of <90% (5). 99mTc concentrations of 2.0–3.6 GBq in 5 mL produces lower labeling efficiencies (QC in the range of 89.7%–93.7%). On the other hand, concentrations between 1.9 and 3.6 GBq in 10 mL produce higher labeling efficiencies (QC in the range of 97.7%–99.2%) (6).
The radiochemical purity decreases as time between steps in MAG3 preparation increases (7). Because of photolytic degradation, it is necessary to minimize any direct light exposure to both the cold kit formulation and the radiopharmaceutical to prevent the formation of impurities (8,9). The addition of 2 mL (or more) air to the reaction vial is essential and necessary to prevent the progressive formation of 99mTc-labeled impurities (4,7). Finally, the nonfasting state will tend to reduce the hepatobiliary excretion of MAG3 (2,10).
CONCLUSION
Our data show that GB uptake of 99mTc-MAG3 is sporadic and minimal, with no adverse effects in the diagnostic and quantitative analysis of renal function. Careful control of the factors affecting the labeling efficiency of MAG3 and performing the study in the nonfasting state will reduce hepatobiliary excretion. However, additional studies, perhaps with a right angle detector throughout the length of the procedure, would be needed to determine the onset and the course of GB uptake of MAG3, especially within the first 4 min of the study, because most calculations of relative renal function and quantitative analysis are performed during the early phases of the procedure, using the camera technique (11,12).
Acknowledgments
The authors wish to thank Jeffrey M. Boorstein, MD, PhD, and Julie Wisenbrown, CNMT, for their assistance in the preparation of this manuscript.
Footnotes
For correspondence or reprints contact: Alberto J. Arroyo, BA, FSNMTS, NCT, CNMT, Department of Nuclear Medicine, Division of Radiology, St. Vincent Mercy Medical Center, 2213 Cherry St., Toledo, OH 43608.
E-mail: alberto_arroyo@mhsnr.org.





{kind=link}
{kind=link}
{kind=link}
{kind=link}