


Abstract
Objective:A 66-y-old man was diagnosed with esophageal carcinoma and underwent a right thoracotomy and esophagectomy. Postoperatively, a recurring right pleural effusion developed. Because an attempt at lymphangiography failed, lymphoscintigraphy was suggested. Because of the inability to obtain radiolabeled albumin, dextran, or nanocolloid, we used filtered sulfur colloid. (0.1 um). The study confirmed the diagnosis of chylothorax.
CASE REPORT
A 66-y-old man presented with a 2-mo history of weight loss and dysphagia to solids. A CT scan and subsequent endoscopy demonstrated a 4-cm esophageal mass consistent with esophageal carcinoma. Preoperatively, it was noted that the patient also had severe coronary artery disease and a left upper lung mass. Initially, the patient had coronary bypass grafting and underwent a left upper lobe wedge resection. Approximately 2 weeks later, a right thoracotomy and esophagectomy were performed. The surgery was completed without complication. The patient developed bilateral pleural effusions; the one on the right was worse.
The drainage indicated that the right effusion was chylous, so a radiologic lymphangiogram was ordered to better evaluate the leak. Unfortunately, there was significant difficulty in cannulating the lymphatic channels and the test was not completed. Lymphoscintigraphy was suggested and, after discussion, a lymphoscintigram with 99mTc filtered sulfur colloid was proposed. Radiolabeled human serum albumin, dextran and nanocolloid were not available.
MATERIALS AND METHODS
99mTc sulfur colloid was made per the package insert directions from the kit (CIS); a routine quality control (QC) procedure was performed. The sulfur chloride was then filtered through two 0.1-μm filters (Gelman Science Acrodisc; Ann Arbor, MI) as per our typical protocol for sentinel node lymphoscintigraphy. Approximately 7%–15% of the activity remained after filtering. 99mTc sulfur colloid was divided into 4 insulin syringes. The patient was then injected bilaterally in the first and second web-spaces of the feet. Serial whole-body imaging was performed at 4 and 24 h.
IMAGING RESULTS
Abnormal accumulation of activity is seen in the lower right hemithorax (Fig. 1). Expected activity in inguinal lymph nodes is also noted. No other areas of abnormal accumulation are identified. A region of interest was drawn around the thoracic activity and compared with a region including the total injected activity. There was approximately 1% of injected activity present in the thorax at 4 h.
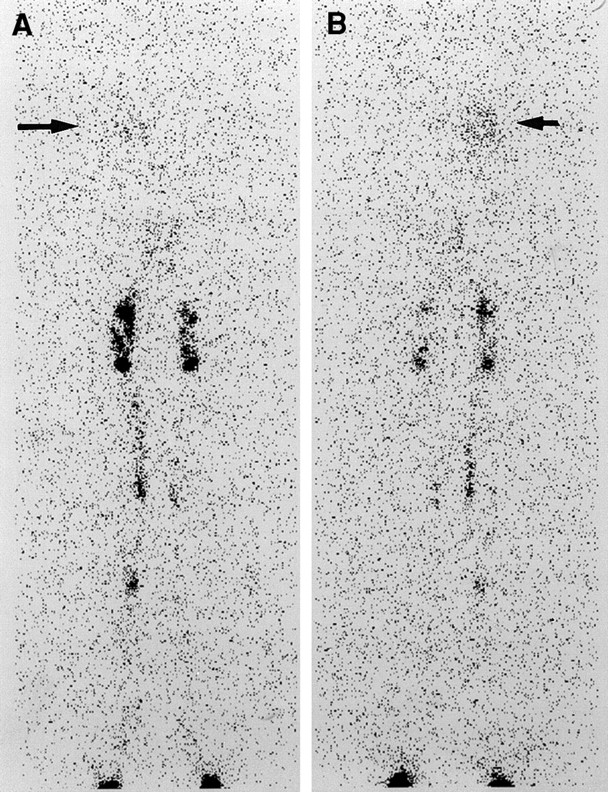
Anterior and posterior whole-body images at 4 h. Radioactivity is seen in the right thorax (arrow) corresponding to the known chylothorax.
Follow-up
The patient had a ligation of the thoracic duct and talc pleurodesis of the left side. Because this procedure did not completely resolve the patient’s problem, a radiographic lymphangiogram with CT imaging was performed; this confirmed an extravasation into the right thorax at the T10 level.
Subsequently, a right thoracotomy, thoracic duct ligation and talc pleurodesis were repeated. Since this procedure, the patient has been stable with no further leakage demonstrated.
DISCUSSION
Chylothorax, a pleural effusion containing chyle, can occur secondary to trauma, neoplasm, malformations of the lymphatic system and surgical procedures involving the pleural space.
Lymphangiography is considered the gold standard in investigating chylothorax, as well as being used to assess other pathologies such as chyloperitoneum, chyluria, thoracic duct patency, abnormal leg lymphatics, and detection of abnormal retroperitoneal lymph nodes.
It is a difficult procedure, requiring cannulation of the lymphatic channels, that can potentially cause adverse effects such as local tissue necrosis, fat embolism to the lungs, hypersensitivity reaction or worsening of lymphedema from the contrast material.
Lymphoscintigraphy has been described previously using radiolabeled human serum albumin, dextran or nanocolloid. It is quick, minimally invasive, and does not have any known side effects. It has become difficult to procure human serum albumin or dextran to do these studies. An attempt was made to use filtered 99mTc sulfur colloid identical to material used in sentinel lymph node lymphoscintigraphy in melanoma or breast cancer.
Our method is similar to what has been described by Hung et al. (3).
Although a portion of the radiopharmaceutical may have been too large and trapped in the inguinal lymph nodes, enough traveled into the thoracic duct to demonstrate the lymphatic leak. A direct comparison with other radiopharmaceuticals was not performed, but if the other materials are not available, adequate studies can be performed with filtered 99mTc sulfur colloid.
Footnotes
For correspondence or reprints contact: Dr. Bohdan Bybel, Department of Nuclear Medicine, Cleveland Clinic Foundation, 9500 Euclid Gb3, Cleveland, OH 44195; Phone: 216-444-2099; E-mail: bybelb@ccf.org.





{kind=link}